-
17 February 2025 | Country Update
Elective Reform Plan with measures to expand planned care in England and reduce waiting times -
08 October 2024 | Policy Analysis
Independent investigation of NHS performance and long-term plan in England -
07 February 2024 | Country Update
Dentistry recovery plan for England -
27 September 2023 | Policy Analysis
General practice access delivery plan -
02 February 2023 | Policy Analysis
Access crisis in UK health services
7.2. Accessibility
All individuals, irrespective of their nationality or immigration status, are eligible to access primary, emergency and compulsory psychiatric care, free of charge. Whether someone is covered by the NHS for secondary care services is determined by whether they are classified as “ordinarily resident”. The United Kingdom law defines this as any person who is “normally residing in the United Kingdom (apart from temporary or occasional absences), and their residence here has been adopted voluntarily and for settled purposes as part of the regular order of their life for the time being, whether for short or long duration” (UK Government, 2021f). This means that undocumented migrants are left without access to many NHS services, including maternity care services, a policy that has been described by Maternity Action as undermining trust and creating a climate of fear among vulnerable pregnant women (Wise, 2019). It is not known exactly how many undocumented migrants are in the United Kingdom. Estimates from the Greater London Authority report 594 000–745 000 undocumented migrants in the United Kingdom in 2017 (Jolly, Thomas & Stanyer, 2020), whereas the Pew Research Center estimates between 800 000 and 1.2 million undocumented migrants in the same year (Pew Research Center, 2019).
As discussed in section 3.3.1 Coverage, there are some benefits that are not covered by the NHS. Benefits that are explicitly excluded are: prescription charges in England, dental care and optometry (see Box3.1). However, exemptions exist for young and older people, and those on low incomes. There are also variations in local commissioning policies for certain types of care, including fertility treatments and some types of elective surgical care, resulting in so-called postcode lotteries (see section 7.1 Health system governance), wherein some areas will cover certain services or treatments that are not available in a neighbouring region. In addition to this, initiatives such as “do not do” recommendations from NICE (NICE, 2014) and the NHS England Evidence Based Interventions programme (NHS England, 2020c), that aim to reduce the provision of low-value where there is limited or no evidence of clinical or cost-effectiveness, result in the denial of certain types of care to patients. Access to these types of care, often called procedures of low clinical value through the NHS is often strictly adjudicated, and subject to independent funding requests whereby an independent board assesses individual cases and decides whether reimbursement using public funds is appropriate.
Box3.1
The United Kingdom reports one of the highest levels of unmet need for a medical examination due to cost, waiting times or travel distances, at 4.5% in 2019 (Fig7.1). This differs between high-income and low-income households, with 3.3% of high-income households reporting unmet need compared with 4.9% of low-income households.
Fig7.1
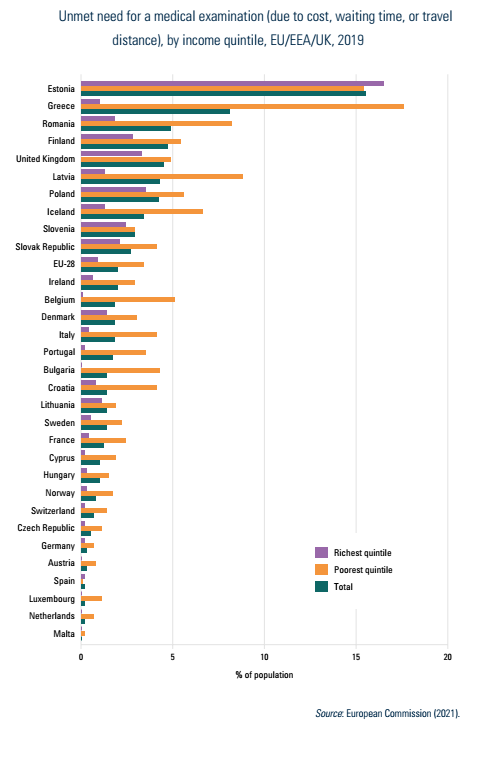
Understanding the trends in accessibility shown in Fig7.1 is a complex issue with a number of explanatory factors. Although care is largely free at the point of service across the United Kingdom, there are often substantial waiting times, particularly for elective care. Before the COVID-19 pandemic, there were around 4 million people on an NHS waiting list in England alone, and the number of people waiting longer than 18 weeks had risen from a historic low point of 6% in 2012 to 17% in February 2020 (NHS England, 2021e). This situation has worsened during the pandemic as noted above, with approximately 5 million people on an NHS waiting list in England as of September 2021 (NHS England, 2021e). For primary care, data from June 2021 in England reveal that approximately 46% of booked appointments are conducted on the same day and 76% are conducted within one week (NHS Digital, 2021b). Apart from during the beginning of the COVID-19 pandemic, when demand for primary care services reduced and the proportion of patient appointments conducted the same day peaked at 63% in April 2020, these statistics have remained relatively stable over the last five years.
Waiting times also vary across the United Kingdom constituent countries, with the highest waiting times experienced in Northern Ireland, where before the pandemic, 100 times more people were waiting over a year for a consultant-led outpatient appointment than in England, despite having a considerably smaller population (FactCheckNI, 2019). Wales and Scotland use different targets, but waiting times are more comparable to England, with 16% of people waiting more than 26 weeks for elective care in Wales in February 2020 (StatsWales, 2021c) and 20% of people waiting more than 18 weeks for elective care in Scotland in February 2020 (Public Health Scotland, 2021b). Waiting times for primary care services in each United Kingdom constituent country are not published in a consistent manner, and therefore cross-country comparisons are not feasible.
For the many individuals who are subject to long waiting times or who seek care not routinely available on the NHS, the alternative is to seek care in the private health care sector, either through out-of-pocket payments or supplementary private medical insurance (see section 3.5 Voluntary health insurance). Analysis of the United Kingdom private health care market has shown that revenue generated from these out-of-pocket payments grew in real terms by an average of 7% per annum between 2010 and 2019 (Heath, 2021), showing a growing demand for accessing elective care in the private health care sector through self-payment mechanisms. As this option is more freely available to those with higher incomes, this will contribute to disparities in unmet need for health care experienced by different income quintiles, as highlighted in Fig7.1.
The United Kingdom is known to have lower levels of hospital beds and staff than other comparable high-income countries (see section 4.1.1 Infrastructure, capital stock and investments and section 4.2.2 Trends in the health workforce). There is also significant variation between the United Kingdom’s constituent countries. In 2020, England had 2.3 hospital beds per 1000 population compared with 3.8 per 1000 population in Scotland, 3.4 per 1000 population in Wales and 3.1 per 1000 population in Northern Ireland (Fig4.2). In 2019, England had 6.7 nurses per 1000 population, compared with 9.1 per 1000 population in Scotland, 8.4 per 1000 population in Wales and 9.3 per 1000 population in Northern Ireland (Fig4.9). The factors behind these disparities are not fully understood, but a combination of different levels of funding per capita in each United Kingdom constituent country (see Table3.2), and poor planning in relation to capital investment and training places are likely to have contributed. There are also substantial in-country differences, with nursing vacancy rates in 2020 varying between 13% in London and 8% in the North of England (NHS Digital, 2021d). The number of patients per GP also varies greatly between regions in England, from 1768 patients per GP in the Vale of York CCG to 2862 per GP in the North East Essex CCG (Nuffield Trust, 2021c).
| Fig4.2 | Fig4.9 |
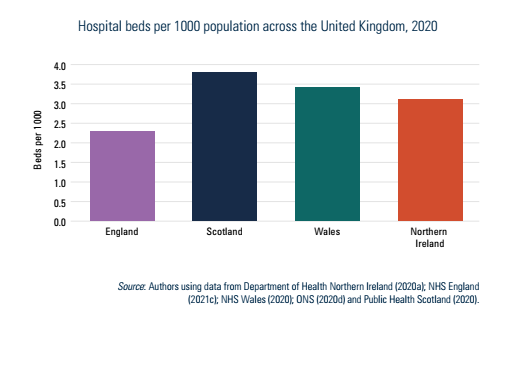 | 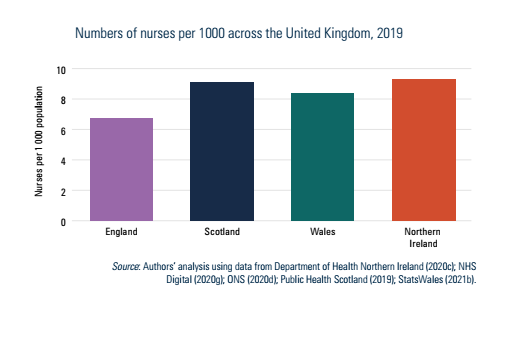 |
Table3.2

On 6 January 2025, NHS England published the “Reforming Elective Care for Patients” plan [1]. This outlined its approach to meeting the government's commitment to deliver the formal target for fewer than 95% of patients to be waiting less than 18 weeks from referral to elective treatment by March 2029 – a target announced as one of six national “milestone” priorities for the UK by the Prime Minister. The proportion is currently below 60%, following a prolonged decline both before and following the outbreak of COVID-19. Polling shows that waits for planned care [2].
An interim target requires 65% of patients to receive treatment within 18 weeks of referral by March 2026. Each NHS trust is expected to achieve a minimum five percentage point improvement against the 18-week target by the same date.
The plan commits to creating 17 new and expanded surgical hubs by June 2025 to expedite common surgical procedures on separate sites to the provision of acute care. It calls for five additional Community Diagnostic Centres. This continues a previous policy of introducing these focused, small locations which aim to move patients through all required diagnostic procedures at one site on a single occasion: more than 165 already exist. It mandates that all Community Diagnostic Centres (CDCs) operate 12 hours per day, seven days a week, delivering same-day tests and consultations.
Around 75% of adults in England are registered for an NHS app. The plan aims to make this a central tool for managing elective care, allowing patients and proxy carers to book, change, or cancel appointments directly. Patients will be able to select from a broader range of NHS and independent sector providers for treatment. Diagnostic test bookings and sharing of results will also be integrated into the app. The plan emphasizes real-time updates on waiting times and appointment availability to improve transparency and enable more informed decision-making about treatment options and locations.
There are also commitments to:
- Work with patient representatives on a set of minimum standards for experience in elective care by September 2025.
- Collect and publish data on health inequalities, recognizing the longstanding issue in the NHS of inequality in access between more and less deprived areas for elective care.
- Work with the independent sector, with whom an accompanying memorandum of understanding was drawn up, to expand choice, with private providers committing to improve their capacity for patients with more complex problems, and for orthopaedics and gynaecology where waits are particularly long [3].
Authors
References
[1] https://www.england.nhs.uk/wp-content/uploads/2023/04/reforming-elective-care-for-patients.pdf
[2] https://www.nuffieldtrust.org.uk/news-item/public-satisfaction-with-the-nhs-what-do-the-findings-from-the-2023-british-social-attitudes-survey-tell-us
[3] https://www.gov.uk/government/news/deal-between-nhs-and-independent-sector-to-cut-nhs-waiting-lists
On 25 September, the UK Department of Health published a review of National Health Service performance in England by the prominent surgeon Lord Ara Darzi [1]. This was commissioned by the Secretary of State for Health in July, following the electoral victory of the Labour party, presented as a stock-take of their inheritance from the previous Conservative party government [2].
The report warned that the English National Health Service (NHS) is “in serious trouble”, with a crisis marked by unprecedented public dissatisfaction, poor access to care, and declining health outcomes. It also made recommendations for a forthcoming 10-year plan for the service, expected in 2025 following a public engagement process.
Waiting times for GP appointments, community services, and mental health care have surged, with millions waiting for treatment, particularly among vulnerable populations like children. The NHS has not met key performance targets since 2015, leading to further erosion of public confidence. Cancer survival rates remain below those of comparable countries, and the rate of inclusion has slowed over the last 15 years. Despite recent increases in staffing, productivity appears lower than before the COVID-19 pandemic, which has left a difficult legacy of higher need, staff stress, and delayed treatment.
Lord Darzi noted that deteriorating population health, associated with worsening of the social determinants of health, such as housing and income, had exacerbated the situation. The report also pointed to diminished and limited managerial capacity, praising management generally for attempting to “keep the show on the road”, and to a lack of capital investment. It concluded that the move to “Integrated Care Boards” bringing together purchasers and providers “has the makings of a sensible management structure” and applauded the shift towards collaboration over competition. However, it noted that despite attempts to shift care from hospitals to community and primary care, spending and staffing had become even more concentrated in hospitals.
Specific policy recommendations were outside the report’s scope, but it provided a set of themes for a comprehensive 10-year health plan to address systemic issues and strengthen the NHS. These were:
- Re-engage staff and re-empower patients.
- Lock in the shift of care closer to home by hardwiring financial flows, reflecting a government commitment to expanding the share of the budget spent outside hospital.
- “Simplify and innovate care delivery for a neighbourhood NHS”, with multidisciplinary care across primary, community and mental health care.
- Drive productivity in hospitals through better management and capital investment.
- Improve the use of technology, particularly by expanding electronic records and digital data to services outside hospital, and by adopting AI.
- Contribute to the nation’s prosperity by reducing the number of people economically inactive due to health needs.
- Clarify roles and accountabilities, rebalance management capacity, and improve capital approvals so that the health service is better able to deliver on policies.
References
NHS England and the Department of Health and Social Care published Faster, simpler and fairer: our plan to recover and reform NHS dentistry [1]. The policy aimed to respond to a long-term trend where a large and growing proportion of the population are unable to access the National Health Service’s primary dental care, due to low participation of dentists in the state-supported system.
This document promised a higher minimum (GBP 28) level for the “Unit of Dental Activity”, the simple base unit at which dental activity is paid. This is a response to a situation where an unreformed contract means some areas of the country pay far less than others, leading to highly uneven access. It also committed to bonus payments for treating patients who had not been seen in the preceding two years, in order to incentivise addressing the problem of people outside the state system, and introduced dental vans as a travelling solution for isolated areas with poor access while more progress could be made.
On workforce, the plan reiterated a commitment to a 40% increase in training of dental therapists and other associate professionals, as well as dentists themselves, by 2031/32. It introduced GBP 20 000 “golden hellos” for 240 posts in priority areas, and announced a consultation on mandatory public sector work requirements for dentistry graduates. Accompanying guidance stated that it was permissible for dental therapists and other professionals to open and close courses of NHS treatment, something previously often understood to require a fully qualified dentist.
The plan also contained oral hygiene outreach activities in nurseries and child support centres, and teams in school to apply preventative fluoride varnish to 160 000 children. There will be consultation on an expansion of water fluoridation, initially to the north-east of England.
The plan confirmed a pledge for longer term reform to the dental contract. It was criticised by experts and key institutions, including the Health and Social Care Committee of the UK Parliament, for delaying these larger reforms [2]. The existing contract has not been changed since 2006 despite being widely perceived as deeply flawed [3]. Its limitations have been associated with a long-term decline in access, a shift of staff and patients to the self-pay private sector, and a lack of incentives for prevention.
Authors
References
Context
Over several years before and following the most challenging phases of the COVID-19 pandemic, access and continuity in primary medical care in England and public satisfaction have steadily declined. While the proportion of appointments taken up the same day remained constant [1], the large-scale GP patient survey showed people found it harder to make contact, get an appointment, and see the doctor of their choice [2]. An important point of context is the steadily declining numbers of general practitioners relative to the size of the population in England.
Impetus for the reform
The delivery plan was motivated by a political and policy drive to improve access to general practice. The British Social Attitudes Survey showed public satisfaction, previously high, declining to an all time low in 2022 [3].
Main purpose of the reform
The delivery plan, published in May 2023, emphasized improving access to appointments as its overarching goal. It sought to do this by removing and rerouting some activity to free up clinician time and capacity; by improving the technology used for contact and triage; and by increasing total workforce capacity. Its targets and actions focused on achieving these intermediate goals, rather than setting an explicit commitment or ambition for improving access.
Content and characteristics
Measures to reduce demands on general practice staff included new provisions for community pharmacists to prescribe medicines including antivirals and antibiotics for seven self-limiting conditions, including sore throat and uncomplicated urinary tract infection. This is described as the “Pharmacy First” initiative and is to be permitted through directives expanding the scope of pharmacist practice for specific patient groups – an established mechanism. There was also a commitment to expand existing initiatives for pharmacists to manage blood pressure consultations and ongoing oral contraception.
A funding increase of £645 million over two years has been allocated for these pharmacy initiatives, and other group directions will enable pharmacy technicians to dispense medicines, aiming to free the time of fully qualified pharmacists.
There are also measures and processes to reduce administrative work relating to patients referred to secondary care. This includes requiring secondary care providers to issue their own referrals for related or immediate needs, and their own recalls to patients after treatment, rather than sending patients back to general practice.
A programme of supporting practices to adopt cloud-based telephony services described as “Modern General Practice Access” is included within the plan, with £240 million in existing funds reallocated as funding. Practices signing up within two months were to receive support with procurement, contracts, training and transition funding. Fully funded online consultation tools will also be provided.
On workforce capacity, an existing programme reimbursing 50% of payroll and other costs for employing non-medical staff including pharmacists, mental health workers and paramedics was extended with additional funding. The plan set out the introduction of more streamlined review and approval processes tailored to individuals seeking to return to work having left general medical practice. The plan also emphasizes the earlier extension of tax allowances for pensions among higher earners, seen as relevant to many doctors, and the gestures to the Long Term Workforce Plan published the following month, which expanded GP training.
Implementation steps taken
NHS England has implemented the process of practices bidding for and receiving support for adopting digital telephony [4]. A consultation has been opened on group directions to enable pharmacy technicians to dispense medicines.
Outcomes to date
Assessing the impact on patient experience of access relies primarily on England’s large annual patient surveys, not yet available for this period. Activity data is likely to be analyzed in future for further changes, but any changes would be expected to be at an early stage. No specific evaluation has been commissioned of the delivery plan as a whole. The Department of Health and Social Care has commissioned an evaluation of the new “Pharmacy First” provisions [5].
Authors
The UK’s publicly funded national health services – in Scotland, England, Wales and Northern Ireland – are experiencing a crisis in access to urgent care, planned care, and primary care. This represents an exacerbation in the wake of COVID-19 and pre-existing failures to deliver waiting time commitments. Urgent and emergency care performance has been placed under further pressure by seasonal respiratory illnesses as of winter 2022–23.
Planned care waits over a year remain many times more common in both Scotland and England than before the pandemic, and have worsened considerably in Wales and Northern Ireland where they have always been prevalent. The proportion of people waiting less than four hours in emergency departments, a key performance metric, has fallen to 70% or less in each country.
Primary care has also seen an apparent deterioration in access. Mass annual surveys show that in general practice, continuity of care, waits for appointments, satisfaction and ease of contact have all fallen steadily since 2012 before deteriorating more sharply in 2022.
Reflecting this poor performance, opinion polls show a sharp decline in satisfaction with the running of these services, and in confidence that emergency services will be available. The majority of British adults surveyed by Ipsos MORI said that they were not confident “that NHS services in your local area will be able to provide high quality health care to patients during this current winter”.
An important immediate cause of these problems is that admissions and outpatient appointments remain depressed to pre-pandemic levels despite higher spending and staffing levels. Longer term trends which are significant in driving these dynamics include:
- Struggling and underfunded social care systems, and a lack of investment in rehabilitative, step-down and other community care services, leading to lengthening average stays in hospital.
- Increased staff turnover following the height of the pandemic.
- Continued significant numbers of COVID-19 patients, with longer than average length of stay.
- Impaired health system resilience: low numbers of doctors and nurses, low historic capital spending, chronically high bed occupancy, and hospital buildings where a lack of single-occupancy rooms makes infection control difficult.