-
02 June 2025 | Policy Analysis
Restrictions on care worker migration -
07 February 2024 | Country Update
Dentistry recovery plan for England -
25 July 2023 | Country Update
Long term health workforce plan for England -
02 February 2023 | Country Update
National Health Service strikes
4.2. Human Resources
In May 2025, the UK Government published a new Immigration White Paper [1], setting out intended policies to restrict migration. Both specific and general provisions are likely to reduce migration of healthcare and social care workers. Migration has recently been a major or primary source of care staff in several fields.
Social care
The white paper specifically sets out an intention that new visas for social care workers coming from outside the UK are discontinued. “Social care” in the UK refers to all long-term care for disability, illness and old age, and this restriction applies to direct care workers who are not part of a more specialized groups such as nurses. Those who are already in the country working in these roles will be allowed to apply to extend visas or switch to another employer until 2028. This follows changes in 2023 and 2024 with greater enforced requirements for only registered providers directly hiring staff, which had already caused a collapse in visas issued [2].
The previous context was one of very high reliance on international recruitment from outside the UK and EU in a sector which has struggled to remain competitive domestically. In just two years from 2021/22 to 2023/24, the proportion of the total English care workforce from outside the EU had risen from 10% to 20% [3]. Social care in England remains under intense financial pressure, and is chronically failing to meet the level of need for support with daily activities [4].
Healthcare
The white paper commits to lifting the educational requirement for jobs eligible for skilled worker visas to a university degree. This would prevent recruitment into entry level direct care support roles within healthcare, which had previously been increasing.
Other provisions and changes are likely to be significant for clinical professional groups, though less directly. There is a commitment to raise the salary threshold for skilled worker visas. This is already set above certain pay bands for biomedical scientists in the English National Health Service [5]: further increases may affect nursing roles. The number of years required for permanent settlement and therefore citizenship is extended from 5 to 10, reducing attractiveness.
The UK has recently had a very high level of reliance on international migration for both doctors and nurses, with non-EU migrants accounting for half or more of all new joiners to the professional register. In England, two thirds of the significant nursing workforce expansion since 2020 has been accounted for by staff holding non-UK and non-EU nationalities [6].
Implementation
These changes can be implemented without legislation, through statements set before Parliament. This typically takes place quite rapidly following statements of policy change, but as of late May 2025, formal changes had not yet been published.
Authors
4.2.1. Planning and registration of human resources
Overall planning for the health and care workforce across the United Kingdom is the responsibility of its four constituent countries. With a view of improving both recruitment and retention, each United Kingdom constituent country maintains a long-term workforce strategy (Anderson M et al., 2021a). Workforce planning for United Kingdom-trained clinical staff in the NHS begins with recruitment to higher education programmes in medicine, nursing, pharmacy and many other health and care professions. The numbers of publicly funded places on such programmes, apart from a small number associated with private university entry, are determined by bodies including Health Education England, NHS Education for Scotland, Health Education and Improvement Wales and the Northern Ireland Medical & Dental Training Agency. Regulatory standards are shared across constituent countries, with the remit of regulatory bodies such as the GMC, General Dental Council (GDC) and Nursing and Midwifery Council (NMC) being United Kingdom-wide. Furthermore, the scope of the medical royal colleges extends across the United Kingdom, and they play a crucial role in setting educational standards and issuing guidance.
4.2.2. Trends in the health workforce
The NHS in England is the world’s fifth largest employer, with, as of 2020, around 1.5 million employees (Rolewicz & Palmer, 2021). In Scotland, as of 2021, the NHS employs around 178 000 staff (Public Health Scotland, 2021c); in Wales, as of 2020, it employs around 100 000 (StatsWales, 2021b) and in Northern Ireland, as of 2020, it employs around 70 000 (Department of Health Northern Ireland, 2020b). A further 2 million people in the United Kingdom are employed to deliver social care services. In the figures below, note that because of differences in the way data are recorded and physicians are defined, they are not fully comparable across United Kingdom constituent countries.
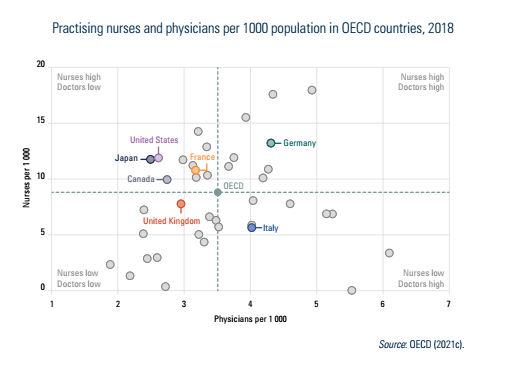
The United Kingdom is exceptional among other high-income countries, in having lower levels of both nurses and doctors per 1000 population (Fig4.3). The degree to which this impacts quality and/or access to health care is unclear. It is possible that this discrepancy is explained by the fact that the United Kingdom makes greater use of nonclinical staff and allied health care professionals, as the United Kingdom compares more favourably to other high-income countries when looking at total numbers of the health and care workforce (Fig4.4).
| Fig4.3 | Fig4.4 |
 |  |
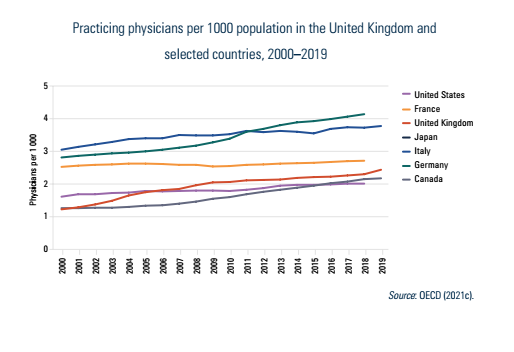
The number of physicians working in the United Kingdom has been steadily increasing for the past 20 years as shown in Fig4.5. In 2000, there were 1.98 physicians per 1000 people and by 2019 that number rose to 2.95. However, the United Kingdom still has lower numbers of physicians than many other high-income countries. Despite an ongoing policy agenda to shift care from hospital closer to home within the community, the majority of this increase in physician numbers has been concentrated in hospital consultants (Fig4.6). This is a trend seen in all United Kingdom constituent countries, which all continue to experience challenges in improving recruitment and retention of the GP workforce. There have been ongoing attempts to increasing training numbers for GPs across the United Kingdom and in England there were 4000 training places filled in 2021 compared with 3157 in 2017 (HEE, 2021); however, it will take several years for this increase in training places to impact the GP workforce.
| Fig4.5 | Fig4.6 |
 |  |
The United Kingdom has lower levels of nurses per 1000 population than most other high-income countries (Fig4.7) and this trend has continued over the last decade. These reductions in nursing numbers are more acute among different types of registered nurses. In England, between 2010 and 2020, adult and children’s registered nursing numbers (full-time equivalent) increased by 14% and 59%, respectively, whereas mental health nurses and learning disability registered nurses fell by 8% and 40% respectively (Fig4.8). However, some mental health nurses and learning disability nurses are employed by independent organizations that are commissioned by the NHS and therefore are not captured by these data. This outcome may have been driven partially by the Francis Inquiry published in 2013 (Francis, 2013), launched in response to concerns about patient safety in an NHS hospital, that recommended an increase in hospital nursing numbers, thus distorting the employment of nurses to the acute sector at the expense of community health services. There are also different nursing staffing levels across the United Kingdom, with lower numbers of nurses per 1000 population in England, compared with Scotland, Wales and Northern Ireland (Fig4.9).
| Fig4.7 | Fig4.8 |
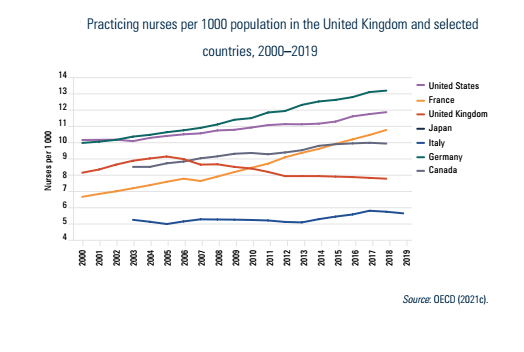 | 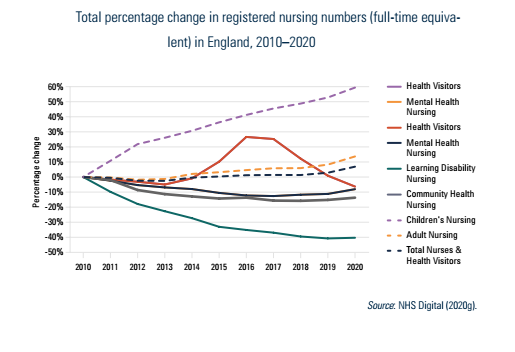 |
Fig4.9
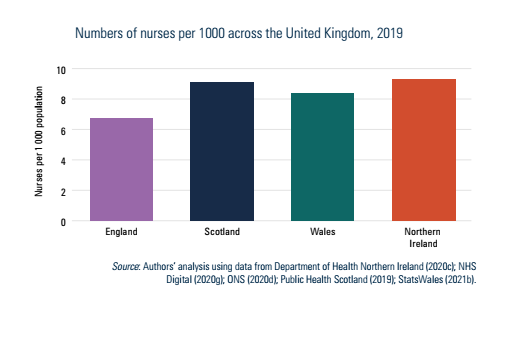
Box4.2 describes the distribution of health workers in the United Kingdom.
Box4.2
NHS England and the Department of Health and Social Care published Faster, simpler and fairer: our plan to recover and reform NHS dentistry [1]. The policy aimed to respond to a long-term trend where a large and growing proportion of the population are unable to access the National Health Service’s primary dental care, due to low participation of dentists in the state-supported system.
This document promised a higher minimum (GBP 28) level for the “Unit of Dental Activity”, the simple base unit at which dental activity is paid. This is a response to a situation where an unreformed contract means some areas of the country pay far less than others, leading to highly uneven access. It also committed to bonus payments for treating patients who had not been seen in the preceding two years, in order to incentivise addressing the problem of people outside the state system, and introduced dental vans as a travelling solution for isolated areas with poor access while more progress could be made.
On workforce, the plan reiterated a commitment to a 40% increase in training of dental therapists and other associate professionals, as well as dentists themselves, by 2031/32. It introduced GBP 20 000 “golden hellos” for 240 posts in priority areas, and announced a consultation on mandatory public sector work requirements for dentistry graduates. Accompanying guidance stated that it was permissible for dental therapists and other professionals to open and close courses of NHS treatment, something previously often understood to require a fully qualified dentist.
The plan also contained oral hygiene outreach activities in nurseries and child support centres, and teams in school to apply preventative fluoride varnish to 160 000 children. There will be consultation on an expansion of water fluoridation, initially to the north-east of England.
The plan confirmed a pledge for longer term reform to the dental contract. It was criticised by experts and key institutions, including the Health and Social Care Committee of the UK Parliament, for delaying these larger reforms [2]. The existing contract has not been changed since 2006 despite being widely perceived as deeply flawed [3]. Its limitations have been associated with a long-term decline in access, a shift of staff and patients to the self-pay private sector, and a lack of incentives for prevention.
Authors
References
In June 2023, NHS England published its Long Term Workforce Plan, produced and agreed with the UK government. This follows a decade without an overall staffing strategy. The plan is intended to respond to unsustainable trends in public health service staffing, including higher rates of resignation and sickness absence after COVID-19, a falling number of general practitioners relative to population, and reliance on international recruitment for over 50% of newly registered doctors and nurses.
The plan uses a projection of demand growth, which predicts a requirement for 50% more staff (around 0.8 million) over a 15-year period to 2036/37. It also aims to address existing shortages. Calculations assume labour productivity increases of 1.5% to 2%, well above what the NHS has historically achieved.
It sets out a major expansion in professional training places, increasing medical training places by a third by 2029, and doubling them by 2032 alongside a 92% increase in training places for adult nursing. The UK’s nursing regulator is asked to reduce the required number of clinical placement hours for qualification from 2300 to 1800 to help increase throughput, a step permissible following the UK’s exit from the EU and its Professional Qualifications Directive.
The plan’s projections anticipate especially fast increases in new roles carrying out tasks traditionally undertaken by doctors and nurses. The number of nursing associates, trained assistants taking on some nursing tasks but not fully qualified as nurses, will rise from 4600 to 64 000 by 2032. Numbers of physician associates, anaesthesia associates, and advanced practitioners will also increase. Existing policies to extend the use of non-GPs in primary care practices will expand.
Some stakeholders raised concerns that the plan did not address measures to retain staff in detail, in the context of widespread industrial action over wages in the UK.
Authors
References
https://www.england.nhs.uk/publication/nhs-long-term-workforce-plan
https://www.nuffieldtrust.org.uk/resource/all-is-not-well-sickness-absence-in-the-nhs-in-england
https://www.nuffieldtrust.org.uk/resource/the-nhs-workforce-in-numbers#toc-header-4
https://www.rcn.org.uk/magazines/Advice/2023/July/NHS-workforce-plan
December 2022 and January 2023 saw a series of strikes by NHS staff groups across healthcare in the UK. The Royal College of Nursing (RCN), representing most nurses, held two one-day strikes in December and a further two in January at more than 50 sites in England and Wales, and ambulance staff staged walkouts across three 24-hour periods. Physiotherapists also went on strike in January. Industrial action is rare in the NHS, and strikes across multiple groups have not been seen on a comparable scale since the late 1970s.
Ballots for industrial action were called in response to the pay settlements announced for the 2022/23 financial year. These marked a significant inflation-adjusted decrease in pay for all relevant groups, particularly junior doctors, who were kept to a previously agreed 2%. This latter group is currently also balloting for strike action. The RCN plans further action for February; however, it has paused strikes so far in Scotland where negotiations are ongoing.
In each case, unions demanded that pay keep up with or exceed the heightened inflation seen during 2022. A longer term decline in wages relative to inflation has been seen across all NHS staff groups, though it varies considerably, with ambulance staff pay declining relatively little since 2010 and consultant doctor pay declining by more than 10%.
The UK Government has introduced the Strikes (Minimum Service Levels) Bill as a response to these actions and others in public services. This would empower employers to order striking unions to work to certain standards of delivery set by the Government and enable the dismissal of employees who disobeyed these orders.
Authors
4.2.3. Professional mobility of health workers
The NHS has a long history of a heavy reliance on foreign staff. Data collected from OECD countries show that the United Kingdom is second only to the United States in being the main destination for foreign-trained doctors and nurses (OECD, 2019c). The largest proportion of foreign-trained doctors in the United Kingdom originates from India (Baker, 2021), with whom the United Kingdom Government has a formal arrangement (NHS Employers, 2022). However, a substantial number also originate from Pakistan and Nigeria (Baker, 2021), countries the United Kingdom has committed to not actively recruit from (for example, targeting individuals through actions by recruitment agencies) as part of the DHSC Code of Practice for International Recruitment (Department of Health & Social Care, 2021a). The NHS and social care sectors are also heavily reliant on the supply of EU workers, which before Brexit was facilitated by the free movement directive. In 2019, approximately 6% of the health and care workforce in England were from Europe, compared with 6% in Northern Ireland, 5% in Scotland and 3% in Wales (ONS, 2019). Within England, approximately 12% of the health and care workforce in London are from Europe, compared with 3% in the North East. The impact of Brexit on the United Kingdom health and care workforce is yet to be fully realized and is unclear because of concurrent changes such as the introduction of a compulsory English language test and the emergence of the COVID-19 pandemic, but the United Kingdom has already seen a considerable drop in the number of EU-trained nurses registering to work in the United Kingdom (NMC, 2020). The United Kingdom Government has introduced a new Health and Care Visa so that the NHS can hire non-United Kingdom workers; however, many essential social care roles are not eligible, which has created a significant barrier to addressing social care staffing shortfalls (Portes, Oommen & Johnson, 2020).
In terms of professional mobility between United Kingdom constituent countries, most professional groups can move freely as United Kingdom-wide regulatory and professional standards ensure that United Kingdom-trained and accredited staff can move from one United Kingdom constituent country to another.
4.2.4. Training of health personnel
There are minor variations between England, Scotland, Wales and Northern Ireland, but generally the training and career paths of health workers are as below.
Physicians
To train in medicine, students spend four–six years, dependent upon whether they have already completed an undergraduate degree or choose to do an optional intercalated degree (a further undergraduate degree undertaken in one year instead of three years) on an undergraduate degree course, which takes place under the supervision of the United Kingdom GMC. Continuing professional development is required of all doctors. Doctors show their proficiency in continuing professional development by two methods: the annual appraisal process (one for GPs and one for hospital consultants), and the five-yearly revalidation process, which is more detailed than the annual appraisal, requiring more in-depth evidence, introduced in 2012.
Dentists
To train as dentists, students attend five years of undergraduate dental school. After undergraduate school, they register with the United Kingdom GDC to practise as a dentist. More training is required for dental specialists, such as orthodontists. Specialists usually work in hospitals. Dentists are revalidated through the GDC, a process that began in 2011.
Nurses and midwives
To train as nurses or midwives, students attend a three- or four-year pre-registration degree course. Midwives must have a midwifery degree, or, if they are already a nurse, they can do a short additional training programme. After training, nurses and midwives register with the United Kingdom NMC to practise. Nurses and midwives have to re-register annually, and every three years revalidate with the NMC to illustrate that they have met the standards required for safe practice in their chosen area of work. In 2018, a new nursing associate role has been introduced with the intention to support registered nurses and free them up to focus on more complex care. A nursing associate completes a two-year training programme and, although not implemented yet, there is an expectation that nursing associates will at some point be allowed to progress to graduate level nursing.
Pharmacists
To train as pharmacists, students must obtain a four-year Master of Pharmacy postgraduate degree. After that, they spend a year training in a community or hospital pharmacy, and then register with the Great Britain General Pharmaceutical Council in order to practise.
4.2.5. Physicians’ career paths
Once graduated, physicians enter a two-year foundation programme, including placements in several specialty and health care settings. Specialist training begins after F1 and F2 rotations. Applications to specialty training are coordinated on a United Kingdom-wide basis, with candidates scored according to interviews and predefined criteria that reflect previous experience and academic achievements. Medical royal colleges create curricula and assessments for specialist training. The GMC approves curricula, assessments and the distribution of training posts (specialty registrar posts).
Specialists train in hospitals for another five–eight years, and then join the GMC Specialist Register and can be appointed to a consultant post. GPs train for at least another three years – one year in hospitals and two years in a GP practice. They then join the GMC’s GP Register and can work as a GP. Employers offer a range of other contracts to meet service needs and the choices of doctors. These contracts are recruited through competitive entry and require various levels of experience and training. Once qualified, doctors can also choose to develop managerial roles such as becoming a clinical director, or within local CCGs (see section 2.2 Organization for an overview of the role of CCGs).
4.2.6. Other health workers’ career paths
There are many different career paths for nurses. They can take roles as specialist nurses in most branches of medicines and surgery, and have increasingly been granted more autonomy in their practice, developing competences in undertaking procedures and prescribing (Imison, Castle-Clarke & Watson, 2016). Nurses can also undergo additional training to become advance nurse practitioners who are increasingly used as independent clinicians in their own right to provide primary care services and out-of-hour cover in hospitals. Similarly, there have been efforts to expand the role of pharmacists, paramedics, physician associates and a range of other clinicians, particularly in primary care, as part of a broader initiative to maximize the use of multidisciplinary teams to meet changing demand for health care services.