-
27 September 2023 | Policy Analysis
General practice access delivery plan
5.3. Primary care
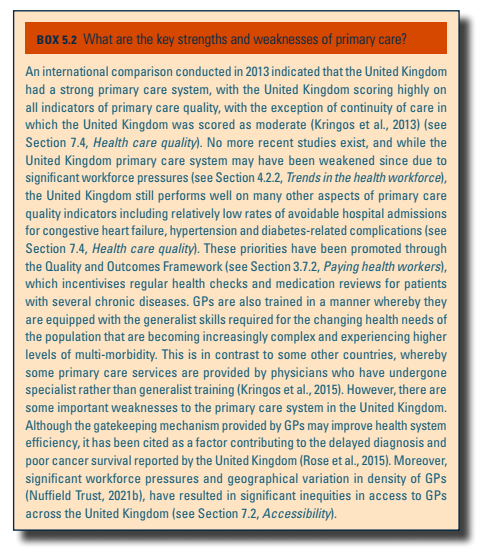
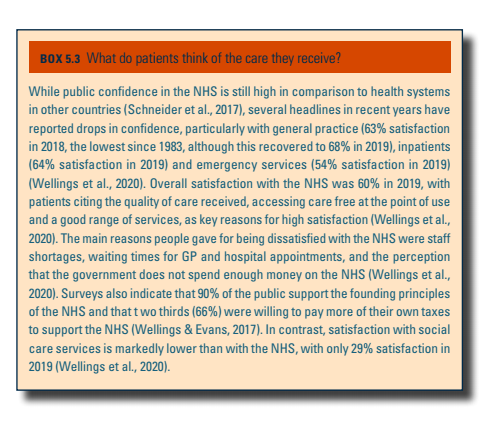
Primary care in the United Kingdom has three main roles (Cylus et al., 2015). It serves as the first point of contact for patients, provides continuing access for common conditions and acts as a gatekeeper to more specialized care. The model in the United Kingdom has remained broadly similar throughout the lifetime of the NHS and in constituent countries following devolution. Although a gatekeeper function is common for primary care, this is more formalized and pronounced in the United Kingdom than other countries (Baird et al., 2018). There is broad consensus that the United Kingdom enjoys a comprehensive and high-quality primary care system (see Box5.2), that contributes to reported high levels of patient satisfaction (Box5.3).
| Box5.2 | Box5.3 |
 |  |
Primary care increasingly means not only a GP but a whole team of doctors, nurses, midwives, health visitors and other health care professionals such as dentists, pharmacists and optometrists in a community setting (Cylus et al., 2015). There is also an increasing use of the voluntary sector in some situations, such as those involving mental health or long-term conditions. Primary care nurses include both practice and district nurses; practice nurses work in GP practices, whereas district nurses work for community health service providers to provide care in patients’ homes.
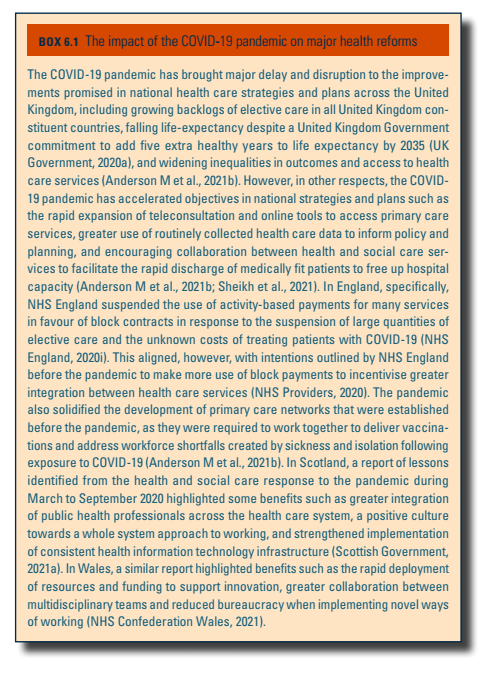
People ordinarily resident in the United Kingdom can register with a GP and consult their GP practice without charge (Cylus et al., 2015). GPs can reject an applicant (unless the applicant has been assigned to them), but they can only do so if it is not discriminatory, or if the patient is out of the practice boundary and the practice has no capacity or feels it would not be clinically appropriate (Practice Index, 2016). GP surgeries provide a range of services, including routine diagnostic services, minor surgery, family planning, ongoing care for patients with chronic conditions, antenatal care, preventive services, health promotion, outpatient pharmaceutical prescriptions, sickness certification and referrals for more specialized care. Not all surgeries provide all of these services. Historically, between 80% and 85% of GP consultations have taken place face-to-face on GP premises, which are called surgeries (NHS Digital, 2021b). However, during the COVID-19 pandemic, approximately 50% of GP consultations were conducted remotely to prevent the transmission of coronavirus (NHS Digital, 2021b). This has increased access for certain working-age adults who previously may have struggled to access appointments, although concerns have been raised that older patients with lower levels of digital literacy have not been served well through this model. Increasingly, GPs are now seeking to adapt the provision of GP services towards a hybrid model involving a combination of face-to-face and remote consultations that best meet patients’ needs (see Box6.1).
Box6.1
Historically, GPs were responsible for out-of-hours care, but following a new contract agreed with GPs in 2004, responsibility for commissioning out-of-hours care shifted to commissioning (that is, purchasing) bodies, with services provided by GP cooperatives or private sector providers. Out-of-hours care consists of call handling, phone assessment and triage, and in-person consultations. Patients in England, Scotland, Wales and Northern Ireland can dial 111 to access information and advice 24 hours a day and to access out-of-hours primary care services, or they can consult the FAQs and symptom checkers online. NHS walk-in centres were introduced in 2000 as an alternative means of accessing primary care without the need to book an appointment. They are heavily reliant on advance nurse practitioners, who are nurses that can independently diagnose and treat patients, and typically are open for extended hours during the day, rather than being open 24 hours a day. Many walk-in centres are located either within or close to emergency care departments, and patients are often signposted to use walk-in centres for minor complaints rather than using emergency care inappropriately.
There is significant variation in the number of GPs to patients across the United Kingdom, as of 2020, ranging from 2826 patients per GP in North East Essex CCG to 1768 patients per GP in Vale of York CCG (Nuffield Trust, 2021b). However, there are challenges in ascertaining reliable estimates of the GP workforce across the United Kingdom, as England is the only country that routinely records data on a full-time equivalent basis. Efforts have been made to have an equitable distribution of GPs, with England, Wales and Scotland all having Targeted Enhanced Recruitment Schemes for GP trainees offering a one-off salary supplement of £20 000 (€23 589) to physicians willing to make a commitment to train and work in underserved regions (NHS England, 2021o). The number of GPs across all United Kingdom constituent countries has remained relatively stagnant over the last decade, during a period when the number of hospital consultants has increased by approximately 40% (Anderson M et al., 2021a). In response, the government has now pledged to recruit an additional 6000 GPs by 2024/2025 by expanding training places, increasing international recruitment and improving retention (Department of Health & Social Care, 2020a). Increasing efforts across all United Kingdom constituent countries are focused on addressing workforce pressures in primary care through the introduction of a broader multidisciplinary team, including advance nurse practitioners, physician associates, paramedics, pharmacists and social prescribers. In England and Wales as part of their national strategies (see section 6.1 Analysis of recent reforms), these efforts are consolidated around primary care networks or clusters, that share a common pool of some staff and work together to provide care for populations of around 50 000.
Context
Over several years before and following the most challenging phases of the COVID-19 pandemic, access and continuity in primary medical care in England and public satisfaction have steadily declined. While the proportion of appointments taken up the same day remained constant [1], the large-scale GP patient survey showed people found it harder to make contact, get an appointment, and see the doctor of their choice [2]. An important point of context is the steadily declining numbers of general practitioners relative to the size of the population in England.
Impetus for the reform
The delivery plan was motivated by a political and policy drive to improve access to general practice. The British Social Attitudes Survey showed public satisfaction, previously high, declining to an all time low in 2022 [3].
Main purpose of the reform
The delivery plan, published in May 2023, emphasized improving access to appointments as its overarching goal. It sought to do this by removing and rerouting some activity to free up clinician time and capacity; by improving the technology used for contact and triage; and by increasing total workforce capacity. Its targets and actions focused on achieving these intermediate goals, rather than setting an explicit commitment or ambition for improving access.
Content and characteristics
Measures to reduce demands on general practice staff included new provisions for community pharmacists to prescribe medicines including antivirals and antibiotics for seven self-limiting conditions, including sore throat and uncomplicated urinary tract infection. This is described as the “Pharmacy First” initiative and is to be permitted through directives expanding the scope of pharmacist practice for specific patient groups – an established mechanism. There was also a commitment to expand existing initiatives for pharmacists to manage blood pressure consultations and ongoing oral contraception.
A funding increase of £645 million over two years has been allocated for these pharmacy initiatives, and other group directions will enable pharmacy technicians to dispense medicines, aiming to free the time of fully qualified pharmacists.
There are also measures and processes to reduce administrative work relating to patients referred to secondary care. This includes requiring secondary care providers to issue their own referrals for related or immediate needs, and their own recalls to patients after treatment, rather than sending patients back to general practice.
A programme of supporting practices to adopt cloud-based telephony services described as “Modern General Practice Access” is included within the plan, with £240 million in existing funds reallocated as funding. Practices signing up within two months were to receive support with procurement, contracts, training and transition funding. Fully funded online consultation tools will also be provided.
On workforce capacity, an existing programme reimbursing 50% of payroll and other costs for employing non-medical staff including pharmacists, mental health workers and paramedics was extended with additional funding. The plan set out the introduction of more streamlined review and approval processes tailored to individuals seeking to return to work having left general medical practice. The plan also emphasizes the earlier extension of tax allowances for pensions among higher earners, seen as relevant to many doctors, and the gestures to the Long Term Workforce Plan published the following month, which expanded GP training.
Implementation steps taken
NHS England has implemented the process of practices bidding for and receiving support for adopting digital telephony [4]. A consultation has been opened on group directions to enable pharmacy technicians to dispense medicines.
Outcomes to date
Assessing the impact on patient experience of access relies primarily on England’s large annual patient surveys, not yet available for this period. Activity data is likely to be analyzed in future for further changes, but any changes would be expected to be at an early stage. No specific evaluation has been commissioned of the delivery plan as a whole. The Department of Health and Social Care has commissioned an evaluation of the new “Pharmacy First” provisions [5].