-
08 October 2024 | Policy Analysis
Independent investigation of NHS performance and long-term plan in England
7.5. Health system outcomes
The previous iteration of the Health System in Transition United Kingdom report showed how life expectancy had improved for the United Kingdom over the previous decade (Cylus et al., 2015). This success was in part driven by a national cross-governmental strategy to improve population health and reduce health inequalities (see section 2.5 Intersectorality). However, since this report, increases in life expectancy have stalled in the United Kingdom and now the health of the population is lagging behind that of many other comparable high-income countries (McKee et al., 2021). These trends in life expectancy are similar across the United Kingdom’s constituent countries, although there remain significant differences in life expectancy between each United Kingdom constituent country, with life expectancy consistently reported as higher in England than in the other three nations, with Scotland lagging far behind (McKee et al., 2021). The latest available data, which are for the period 2018–2020, reveal that life expectancy for men was 79.3 years in England, 76.8 years in Scotland, 78.3 years in Wales and 78.7 years in Northern Ireland (ONS, 2021e). For the same period, life expectancy for women was 83.1 years in England, 81.0 years in Scotland, 82.1 years in Wales and 82.4 years in Northern Ireland (ONS, 2021e) (see section 1.4 Health status). Analyses have indicated that this disparity is driven by a variety of factors including level of deprivation, obesity rates and smoking rates (McCartney et al., 2015; Minton et al., 2017).
Several factors have been suggested as contributing to the United Kingdom’s stalling increases in life expectancy. The United Kingdom experienced significant excess deaths in 2015, attributed in part to a particularly virulent strain of influenza circulating that year, although this did also coincide with widespread capacity issues for acute beds across the United Kingdom in NHS hospitals (Hiam et al., 2017). Some of the decline may also reflect historical trends, specifically the timing of the smoking epidemic peaking in the early 1970s (Leon, Jdanov & Shkolnikov, 2019), but there is also increasing evidence that links stalling increases in life expectancy with austerity measures introduced since 2010. For example, analyses have indicated that funding cuts for local authorities and subsequent reductions in social care service provision have been associated with increased mortality rates, particularly affecting older people and those living in poverty ( Loopstra et al., 2016; Hiam et al., 2018). There have also been considerable cuts to public health services in England over the last decade, as public health has struggled to compete for resources with front-line health services (see section 5.1 Public Health). There have been growing inequalities in life expectancy, with differences between the richest and poorest people in the United Kingdom widening since 2011 (Marshall et al., 2019). The impact of the COVID-19 pandemic on life expectancy is yet to be determined, but as the United Kingdom has experienced one of the highest death rates attributable to the COVID-19 pandemic, the gap in life expectancy between the United Kingdom and other developed nations may grow in the coming years (McKee et al., 2021). The latest data on life expectancy in the United Kingdom reveal that life expectancy at birth in the United Kingdom in the three-year period between 2018 and 2020 was 79.0 years for men and 82.9 years for women, which is a fall of 7.0 weeks for men and a slight increase of 0.5 weeks for women from the latest non-overlapping period of 2015–2017 (ONS, 2021e).
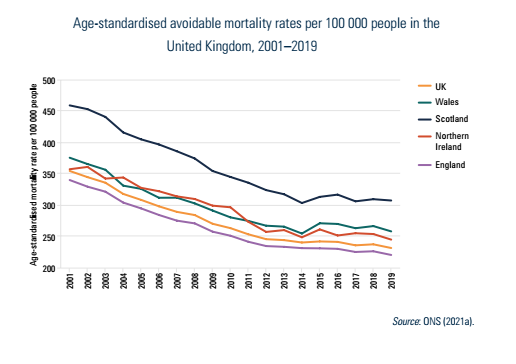
Avoidable mortality, a measure of deaths under 75 years, which are either considered to be amenable (deaths which should not occur if people have access to timely and effective health care) or preventable (deaths which could have been avoided through effective public health and primary prevention interventions), has been developed as an indicator of population health more attributable to the health system than other measures such as life expectancy. In 2019, 22.5% of all deaths in the United Kingdom were considered avoidable and this is broadly in line with rates reported over the previous five years, which followed a significant reduction in avoidable mortality between 2001 and 2014 (Fig7.6). However, similar to life expectancy, Scotland is an outlier and reported much higher rates of avoidable mortality than the other United Kingdom constituent countries. Reductions in avoidable mortality have been driven by decreases in deaths associated with diseases of the circulatory and respiratory system, and from cancer. The notable exception is deaths that are alcohol-related or drug-related that have been increasing in all United Kingdom constituent countries over the last decade, particularly in Scotland, where they have increased from a low of 31.9 per 100 000 people in 2012 to 48.1 per 100 000 in 2019 (ONS, 2021a).
Fig7.6
When focusing on international comparisons, the United Kingdom reports an age-standardized amenable mortality rate of 84.4 per 100 000 in 2016, which is above many other comparable high-income countries such as France and Germany (Fig7.7).
Fig7.7
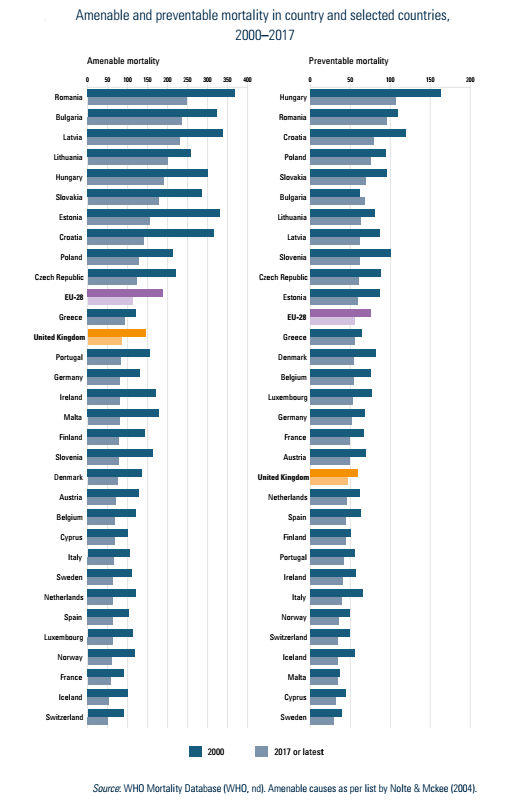
The United Kingdom performs better in relation to preventable mortality, reporting an age-standardized mortality rate of 47.3 per 100 000 in 2016, lower than France at 49.0 per 100 000 and Germany at 51.3 per 100 000 in the same year (Fig7.7). This may reflect a range of factors. Screening rates in the United Kingdom are among the highest in OECD countries, with 74.4% of women aged 20–69 years and 75.1% of women aged 50–69 years undergoing screening in 2019 for cervical and breast cancer, respectively, compared with 58.2% and 48.8% in France, and 55.9% and 50.1% in Germany (OECD, 2019b). However, it should be noted that cervical screening rates have reduced from a peak of 83.7% in 2000. The United Kingdom also reports relatively low smoking rates, with 15.8% of the population aged above 15 years reported as daily smokers in 2019, below 24.0% in France and 18.8% in Germany (OECD, 2019b). The United Kingdom does have relatively high rates of obesity, with 64.2% of the population aged above 15 years self-reporting as being overweight or obese in 2019, compared with 45.3% in France and 52.7% in Germany (OECD, 2019b). As discussed in Box5.1, the United Kingdom and devolved governments have also been committed to influencing healthy behaviour change through fiscal and pricing policies. For example, in 2018, the United Kingdom Government introduced a tax on manufacturers of soft drinks related to sugar content, which one year after implementation resulted in a 10% reduction in sugar content in soft drinks, without impacting sales (Pell et al., 2021). Scotland introduced minimum unit pricing for alcohol purchases in 2018 and Wales followed suit in 2020 (Anderson P et al., 2021), with subsequent analysis demonstrating an 8% reduction in alcohol sales in both of these countries (Anderson P et al., 2021).
Box5.1
On 25 September, the UK Department of Health published a review of National Health Service performance in England by the prominent surgeon Lord Ara Darzi [1]. This was commissioned by the Secretary of State for Health in July, following the electoral victory of the Labour party, presented as a stock-take of their inheritance from the previous Conservative party government [2].
The report warned that the English National Health Service (NHS) is “in serious trouble”, with a crisis marked by unprecedented public dissatisfaction, poor access to care, and declining health outcomes. It also made recommendations for a forthcoming 10-year plan for the service, expected in 2025 following a public engagement process.
Waiting times for GP appointments, community services, and mental health care have surged, with millions waiting for treatment, particularly among vulnerable populations like children. The NHS has not met key performance targets since 2015, leading to further erosion of public confidence. Cancer survival rates remain below those of comparable countries, and the rate of inclusion has slowed over the last 15 years. Despite recent increases in staffing, productivity appears lower than before the COVID-19 pandemic, which has left a difficult legacy of higher need, staff stress, and delayed treatment.
Lord Darzi noted that deteriorating population health, associated with worsening of the social determinants of health, such as housing and income, had exacerbated the situation. The report also pointed to diminished and limited managerial capacity, praising management generally for attempting to “keep the show on the road”, and to a lack of capital investment. It concluded that the move to “Integrated Care Boards” bringing together purchasers and providers “has the makings of a sensible management structure” and applauded the shift towards collaboration over competition. However, it noted that despite attempts to shift care from hospitals to community and primary care, spending and staffing had become even more concentrated in hospitals.
Specific policy recommendations were outside the report’s scope, but it provided a set of themes for a comprehensive 10-year health plan to address systemic issues and strengthen the NHS. These were:
- Re-engage staff and re-empower patients.
- Lock in the shift of care closer to home by hardwiring financial flows, reflecting a government commitment to expanding the share of the budget spent outside hospital.
- “Simplify and innovate care delivery for a neighbourhood NHS”, with multidisciplinary care across primary, community and mental health care.
- Drive productivity in hospitals through better management and capital investment.
- Improve the use of technology, particularly by expanding electronic records and digital data to services outside hospital, and by adopting AI.
- Contribute to the nation’s prosperity by reducing the number of people economically inactive due to health needs.
- Clarify roles and accountabilities, rebalance management capacity, and improve capital approvals so that the health service is better able to deliver on policies.