-
04 March 2024 | Policy Analysis
Completing the restructuring of the central health administration in Norway -
15 September 2023 | Policy Analysis
Reorganisation of the Central Health Administration -
31 August 2022 | Country Update
Review of the central health administration
2.1. Organization
Historical background
The present structure of the Norwegian health system was established largely in the second half of the twentieth century, seeing emergence of the key actors: the MOHCS, the National Insurance Scheme (NIS), the Directorate of Health and the Board of Health Supervision. The health sector saw rapid expansion between 1950 and 1970, followed by large investments alongside the country’s economic growth after the discovery of petroleum resources in the North Sea in the 1970s. Around that time, the role of hospitals increased, with growing provision of specialist services. Between 1969 and 2002 counties were responsible for planning, building and managing hospitals, and from 2002 this responsibility was transferred to the five (at the time) RHAs. Municipalities became responsible for primary care in 1982, and their role gradually expanded to include environmental health services and providing services for older people and people with disabilities. In 2001 the regular GP scheme was introduced. By the late 2000s reform efforts were focused on coordination between the municipalities and the RHA, and increased attention was given to the aspects of quality of care and patient safety (Ringard et al, 2013).
Organization
The organizational structure of the Norwegian health care system is built on the principle of equal access to services for all inhabitants, regardless of their social or economic status and geographical location. This overarching goal has been a long-standing feature of the Norwegian welfare system and is embedded in national health care legislation and strategic documents (Norwegian Ministry of Health and Care Services, 2019).
At the national level, the parliament serves as the political decision-making body. The Office of the Auditor General is an independent agency that acts as the supreme audit institution and the supervisory body of the parliament. Its main tasks are to monitor public assets and ensure that these are used and administered according to sound financial principles and according to the decisions and intentions of the parliament. Fig2.1 presents an overview of the health system.
Fig2.1

Health care is organized at three main levels: national, RHAs and municipalities. The system is regulated through a large number of Acts and secondary legislation, broadly reflecting the decentralized nature of the health care system (see also Table2.1 and section 2.2).
Table2.1

At the national level, the government decides on general national priorities and proposes legislation and the national budget, which is subsequently discussed by the parliament. The parliament adopts the annual national budget, proposed by the Ministry of Finance. The Standing Committee on Health and Care Services within the parliament is responsible for matters relating to health care and social care services, public health, drug and alcohol policy, and pharmaceuticals.
The MOHCS determines the national health policy, prepares and oversees legislation and implements national health policy with the help of the Directorate of Health and other subordinate institutions (see Table2.1). The Board of Health Supervision (Board of Health hereafter) is responsible for the supervision of health and social services at national and local levels; it receives instructions from the MOHCS and is assisted in its supervisory role by County Medical Officers (fylkeslegen) stationed in the counties. The MOHCS also has administrative responsibility for a number of other subordinate agencies (see Fig2.1 and Table2.1). The MOHCS is the owner of the RHAs, which in turn own the hospital trusts; the MOHCS has direct responsibility for the provision of specialist care. It is also responsible for overseeing the provision of all other types of care and their coordination. Further, the MOHCS owns the Norwegian Health Net trust which is responsible for provision of secure electronic exchange of patient information via a health communication network between all relevant parties within the health and social services sectors (see section 4.1.4). The Directorate of eHealth (NDE) within the Ministry has the overall responsibility for digitalization of the health care sector. The MOHCS is also the owner of the Wine Monopoly, which is the only company in Norway allowed to sell alcoholic beverages with alcohol content of more than 4.75%.
The RHAs are owned by the MOHCS and are responsible for the provision of specialized care, including both somatic and mental health care, special care for persons with drug and alcohol addictions, as well as other specialized medical services, such as laboratory, radiology and ambulatory services. The RHAs also participate in research and medical education. There are four RHAs in Norway: Northern Norway (Helse Nord), Central Norway (Helse Midt Norge), Western Norway (Helse Vest) and South-Eastern Norway (Helse Sør-Øst). The latter is the largest RHA and covers approximately 56% of the population and consumes 54% of the total RHAs budget (Statistics Norway, 2019). The RHAs are owners of the health trusts (see section 4.1); there are currently 28 health trusts, of which 20 are hospital trusts. In addition, the RHAs have joint ownership of the following health trusts: Procurement Services Health Trust, National Air Ambulance Services Health Trust, Patient Travel Health Trust, EmergencyNet Health Trust, and the National IT Health Trust, as well as an Agency for Hospital Construction. The RHAs are also responsible for the “New Methods” system for introducing health technologies (see Box2.1 and section 2.4). The RHAs and the health trusts are independent legal entities with governing bodies at regional and local levels.
Box2.1

In the counties, the county municipality (fylkeskommune) with an elected county council (fylkesting) is responsible mainly for secondary education, public transport, regional road planning, culture, etc. The county governor (fylkesmannen) is an authority acting on behalf of the Norwegian government and is responsible for monitoring the decisions, objectives and guidelines set out by the parliament and government and their implementation by the municipalities. They also serve as an administrative appeal body for the municipal decisions, including those concerning health services. In the area of health care, the responsibilities of counties have increasingly included coordination of care and provision of public health services (see sections 5.2 and 5.1). In addition, counties are also responsible for safeguarding patients’ access to health and care services through the Ombudsman service (POBO). The counties’ role in the provision of curative health care services is limited to dental care.
Municipalities are responsible for the provision and financing of primary care, including rehabilitation, physiotherapy and nursing, and after-hours emergency services (see Chapter 5). They are also responsible for a wide range of public health and preventive measures, as well as the provision of local emergency care beds for patients with a need for pre- or post-hospital services. Some responsibilities over these services have been retained at the central level, mainly to maintain equal access. For example, all decisions regarding GP funding continue to be determined by the central government (see section 3.7.2). The government in power since 2017 has a stated objective for the municipalities to deliver a larger proportion of health care services, with the goal of bringing care closer to the patient, and to strengthen public health efforts and preventive services (Political platform for the Norwegian Government, formed by the Conservative Party, the Progress Party and the Liberal Party (The Jeløya-platform), 2018).
Health care providers are associated in three organizations: Spekter, Virke and the Norwegian Association of Local and Regional Authorities (KS). Within health care, Spekter represents both public and private hospitals. Together with the trade unions, it plays an important role in the national salary negotiations for employees (see section 3.7.2). Spekter also participates in the development of the legal framework regulating general employment conditions. Virke (Enterprise Federation of Norway) represents not-for-profit organizations within health care, as well as pharmacies and several of the private rehabilitation centres. The KS is the only employers’ association for the municipalities and counties. Its main tasks are to advocate the interests of its members to the central government (including collective bargaining), parliament, labour and other organizations; to advise and inform its members about all matters and developments of importance to local government; and to facilitate the exchange of experience between its members. Since 2006 all municipalities and counties, as well as approximately 500 public enterprises, have been members.
The private health care sector is relatively small but well regulated. At the level of primary care the majority of GPs are self-employed, even though they are fully embedded in the public system through contracts with the municipalities (see section 5.3). Private for-profit providers play a smaller role in the provision of specialist care, accounting for about 10% of the total operating cost for somatic services and 13% of mental health care, plus nearly 37% for substance abuse services and about 11% of nursing beds (Statistics Norway, 2019a). Not-for-profit provision also includes private for-profit hospitals and hospitals set up as foundations that are financed from and seen as an integral part of public health services, e.g. the Diaconal hospital foundation in Oslo, which is owned by the Norwegian Church. Private for-profit hospitals receive most of their funding from the state (on average 76% of their total budgets), whereas this share is 96% for private not-for-profit hospitals (Statistics Norway, 2019a).
Among other state actors, the Ministry of Labour is involved in the health care system, mainly through the Labour and Welfare Administration (NAV), which administers different benefit schemes within the NIS, such as sick leave and disability benefits. It is also responsible for implementation of the Working Environment Act (2008), which ensures safe working conditions and equal treatment among workers, and creates a health-promoting environment at workplaces. A number of other ministries are also involved in issues of relevance to the health care system. For example, the Ministry of Education is involved through planning of the health workforce and provision of health education (see section 2.3); the Ministry of Finance is involved through taxation and budgeting. The overall responsibility for the information and communication technology (ICT) strategy for the public sector lies with the Ministry of Local Government and Modernisation.
Health registries
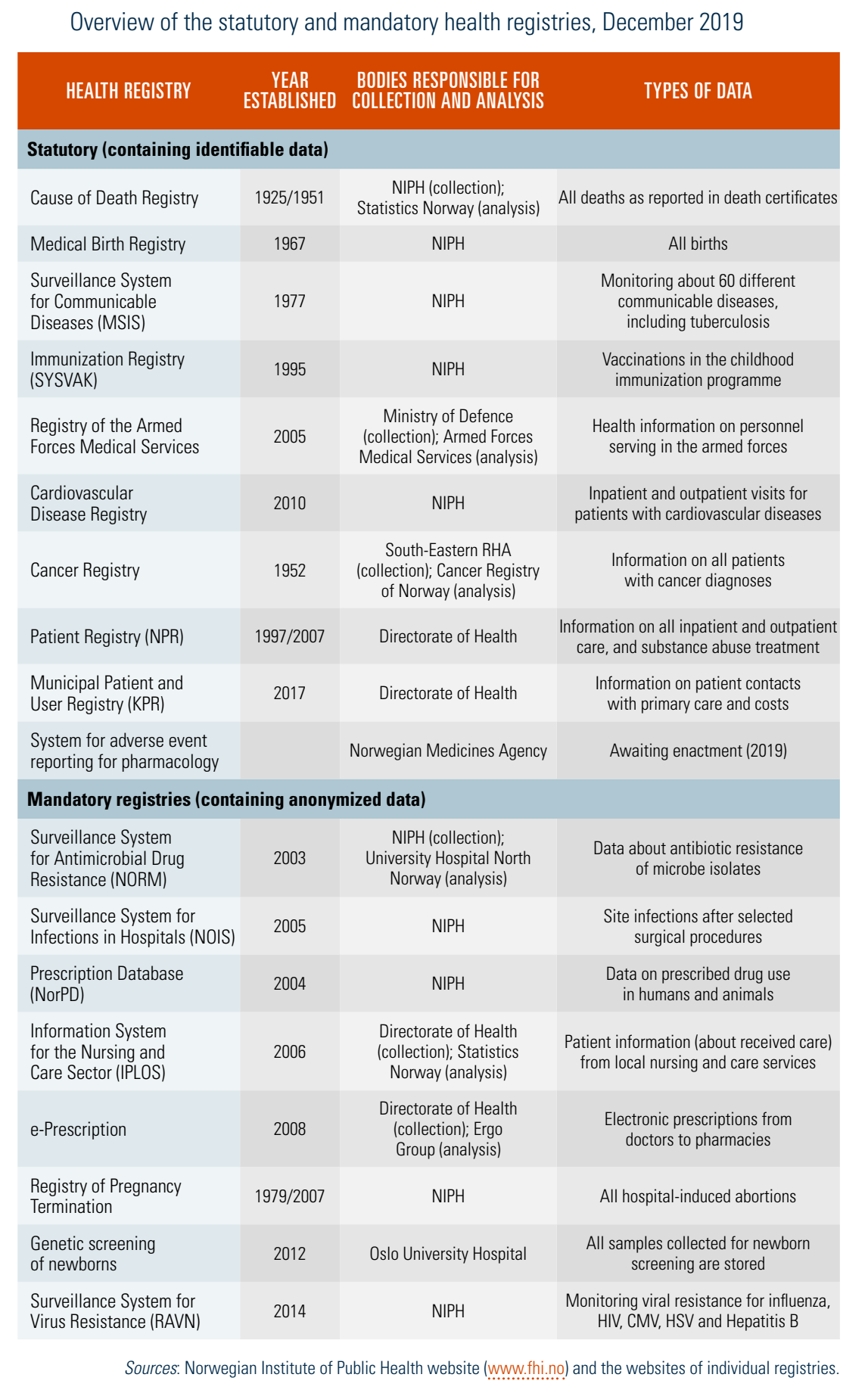
Norwegian health registries contain various types of health data for various purposes. The increasing amount of data availability has led to a reform of the legal framework and organization of health registries. The 2014 Act on the Personal Health Data Registries distinguishes between consent-based registries, mandatory registries where patients can opt out, and statutory registries which do not require consent. The purpose of these registries is to provide current, reliable and secure information about the population’s health and the quality of health care. Information from these registers is analysed and published as part of public statistics. Tabl2.2 provides an overview of the registries and bodies responsible for data collection and analysis. In general, data in these registers are considered to be of high quality (Norwegian Institute of Public Health, 2016; Office of the Auditor General of Norway, 2018). In 2019 there were 10 statutory registries and eight mandatory registries with anonymized patient data.
Table2.2
In addition to the above-mentioned health registries, there are 54 national medical quality registries. The Centre for Clinical Documentation and Evaluation in Tromsø has been a national support centre for the medical quality registries since 2009. These registries can be initiated by individuals, hospitals or educational institutions, and contain comprehensive information for assessing the effects of different treatments and for benchmarking efficiency at the level of hospital wards. They may also be used for quality assurance, research and service improvement. With support from the RHAs, a medical quality registry may be turned into a national quality registry. The RHAs are responsible for funding and managing national quality registries, and the four RHAs have the final say on which registries may be implemented at the national level.
In 2014 the infrastructure project “Health registries for research” (2014–2019) was implemented to support health care research. The project is funded by the Research Council of Norway and includes the establishment of a research documentation service that provides methodology and metadata from the health registries, as well as a statistical support service. The project enhances data security by facilitating the use of secure servers for storage and analysis of research data (HRR metadatabase for Nasjonale Helseregistre, 2019). In 2017 the NDE established the National Health Data Programme, which aims to improve availability of health data for quality improvement, health monitoring, management and research. Users include government agencies, researchers, and health care professionals, as well as residents. The Health Registries for Research project and the National Health Data Programme may be seen as national initiatives aimed at facilitating the use of existing data for health care improvement, monitoring, management and research purposes.
An audit of the existing health and quality registries, undertaken by the Office of the Auditor General in 2017, revealed severe shortcomings in how some of the quality registries are managed, including incompleteness of data, and lacking and/or unpublished information. Of the 54 national medical quality registries, less than a third had countrywide coverage. Fifteen years after the initial mapping of medical quality registries there are still medical areas that are not covered, such as epilepsy, mental health and substance abuse (Office of the Auditor General of Norway, 2018; Saunes & Danielsen, 2005). The recommendations from the audit called for the establishment of performance management and monitoring mechanisms and for strengthening of the registers’ frameworks to promote their effective functioning. In addition, the RHAs need to ensure cross-regional cooperation in the area of medical quality registries.
Another challenge is posed by the lack of linkages between Statistics Norway and the health registries for purposes such as quality improvement, management or planning. According to the legislation in place (Statistics Act, 1989), it is only possible to link data for research purposes. So, for example, information about social inequalities can be linked with health data from the registries for research purposes but not for planning purposes. However, the Statistics Act has been under public consultation in 2019 and its amended version may address data linkage problems.
After the Parliament amended the health legislation on 12 December 2023, to restructure the central health administration, the resulting organizational changes came into force on 1 January 2024 (see Figure 2.1).
Figure 2.1. Overview of the health system following the 2023 amendments

Source: Authors
As the reform aimed at clarifying the roles and responsibilities of the state agencies subordinate to the Ministry of Health and Care Services, it also intended to make the threefold division of roles (that is, governmental tasks, supervisory activities, and knowledge production) clearer and more consistent.
Hence, the role of the Directorate of Health as an authority agency is reinforced, while the role of the Institute of Public Health (NIPH) as a knowledge agency is enhanced. Furthermore, the Directorate of eHealth (NDE) was partially merged with both the Directorate of Health and the NIPH. Finally, the Medical Agency has been transformed into a directorate, now known as the Norwegian Medical Products Agency (NOMA).
The new Directorate of Health was remodelled with a reinforced governmental authority, including an expanded role in analyzing and advising on public health within care services. Its activities encompass interpreting regulations, formal authority tasks within infection control and environmental medicine, government and implementation functions, and responsibility over registers’ analysis and statistics within both the field of health and care services and broader field of public health. As it merged with some functions of the NDE, the Directorate of Health gained responsibility for the digitalization of the health and care services sector.
NIPH’s role as a knowledge centre was strengthened in several areas, including the transfer of the Health Data Department and Health Data Service from the former NDE; and the transfer of the management of the Norwegian Patient Registry (NPR), the Municipal Patient and User Registry (KPR), and the Egg and Sperm Donor Registry (including the Mother and Donor Code Registry) from the Directorate of Health and of the Cancer Registry from the Oslo University Hospital (OUS).
NOMA, the new directorate for Medical Products, was assigned additional responsibilities, notably in the areas of supply chain security, emergency preparedness, procurement, and public financing of medical products. The new agency will now play a more active role in managing emergency stockpiles. These changes will require closer dialogue with stakeholders and strengthened international cooperation, particularly with the European Medicines Agency (EMA) and the European Commission’s Health Emergency Preparedness and Response Authority Directorate-General (DG HERA). Additionally, NOMA became responsible for cost-benefit assessments of all medical products, including vaccines and medical devices, a function transferred from NIPH. Furthermore, the medical products agency gained expanded responsibility on market insight and vaccine procurement, which involves establishing a specialist group within procurement processes for medicines and vaccines that are financed by the Norwegian National Insurance Scheme (Folketrygden), vaccines for vaccination programs, and medicines for the emergency stockpile in Norway.
Authors
References
The Ministry of Health and Care Services proposes changing the central health administration’s organization, roles, and responsibilities. The last reorganization of the central administration took place in 2016. The upcoming changes will directly impact various institutions, including the Directorate of Health, the Norwegian Institute of Public Health (NIPH), the Directorate of eHealth (NDE), the Cancer Registry and the Norwegian Medicines Agency. More specifically, the Ministry is putting forward the following changes [1]:
- Concentrating all heath registers in the NIPH: The responsibility for governing the Patient Registry (NPR) and the Municipal Patient and User Registry (KPR) will be transferred from the Directorate of Health to the NIPH. The NIPH will also take on the responsibility of overseeing the Cancer Registry at Oslo University Hospital.
- Merging the NDE with the Directorate of Health: As a result, the Directorate of Health will be responsible for the digitalization of the health care sector. However, one task from the NDE, administering e-Health methodology and managing health registers, will now be transferred to the NIPH.
- The Norwegian Medicines Agency will become the Directorate for Medical Products: The responsibility for medicines and medical equipment (medical products) is continued, but the agency is given greater responsibility for purchasing medicines and medical equipment. Further, the responsibility for the preparedness and security of supply in the vaccine field is transferred from the NIPH to the Directorate for Medical Products. The overall responsibility for the methodological assessment of medical products is also transferred from the NIPH to the Directorate.
- Distribution of tasks between the Directorate of Health and NIPH: All regulatory functions, implementation functions and registry analyses will be consolidated in the Directorate of Health. The NIPH will retain its monitoring responsibility in infection control and environmental medicine. However, formal regulatory functions will be moved to the Directorate of Health.
Authors
References
In August 2022, the government decided to undertake a review of the central health administration – its organization, and the roles and responsibilities within it. The review concerns the Directorate of Health, the Institute of Public Health, the Norwegian Medicines Agency, the Directorate for e-Health and the Directorate for Radiation Protection and Nuclear Safety.
The main goal is to ensure an efficient use of resources and clarify roles and responsibilities of the different the agencies, as well as the distribution of work between the agencies and the Ministry of Health and Care. This mapping must be completed by 15 February 2023.