-
05 September 2024 | Country Update
Results of First Round of Medicare Prescription Drug Negotiations -
01 May 2023 | Country Update
New Maximums on Insulin Prices
2.7. Regulation
Regulation in the US health care system may be imposed by private or public entities at the federal, state and local county and city levels as a response to “the constant need to balance the objectives of enhancing quality, expanding access, and controlling costs in healthcare” (Field, 2007). All actors in the health care system are subject to regulation, often from multiple government and nongovernment agencies.
As introduced in section 2.1, major federal regulatory organizations include the CMS, the CDC and the FDA, all under the umbrella of the HHS. State regulatory bodies include public health departments, provider licensing boards and insurance commissioners. Local counties and cities also regulate health care through their public health and health services departments. Independent nongovernment and provider organizations such as the AMA and the Joint Commission also have a regulatory role in the US health care system. This section discusses the role of regulation and governance by public and private regulators on third party payers, providers, pharmaceuticals, medical devices and aids, capital investment, patient privacy and human subjects, and public health.
Authors
References
CMS.gov. “Negotiating for Lower Drug Prices Works, Saves Billions.” 15 August 2024. https://www.cms.gov/newsroom/press-releases/negotiating-lower-drug-prices-works-saves-billions
CMS. Gov. “Fact Sheet: Medicare Drug Price Negotiation Program Draft Guidance for 2027 and Manufacturer Effectuation of the Maximum Fair Price in 2026 and 2027.” May 2024. https://www.cms.gov/files/document/fact-sheet-medicare-drug-price-negotiation-program-ipay-2027-and-manufacturer-effectuation-mfp-2026.pdf
Neuman T, Cubanski J, Levitt L. “The First-Ever Government Negotiation Process For Drugs Has Finished, But The Politics Are Ongoing.” Health Affairs Forefront. 19 August 2024. https://www.healthaffairs.org/content/forefront/first-ever-government-negotiation-process-drugs-has-finished-but-politics-ongoing
2.7.1. Regulation of third-party payers
Regulation and governance of private insurers, or third-party payers, in the United States is shared by federal and state agencies. The current regulatory environment facing third-party payers has arisen primarily out of three pieces of legislation: the McCarran-Ferguson Act, ERISA and the ACA.
In reaction to a Supreme Court ruling that the business of insurance was interstate commerce and therefore subject to Congressional regulation and federal antitrust laws, the McCarran-Ferguson Act was passed by Congress in 1945 to counteract the Supreme Court decision and reaffirm the power of states to regulate and tax insurance products of third-party payers (Government Accountability Office, 2005). The Act exempted certain insurance practices from existing federal antitrust laws (i.e., Sherman, Clayton, Federal Trade Commission Acts) to which other interstate businesses were subject (Government Accountability Office, 2005). This exemption applied to activities that: “constitute the ‘business of insurance’; are ‘regulated by State law’; and do not constitute an agreement or act ‘to boycott, coerce, or intimidate’ ”. In essence, this Act reserved authority to regulate third-party payers for state authorities. Many, if not all, states have provisions in their codes to prohibit insurers from engaging in unfair or deceptive acts or practices in their states (Government Accountability Office, 2005). However, in 2011, as part of the ACA, the CMS – a federal agency – took over the review of health insurance rates increasing in excess of 10% annually from some states due to a lack of or inadequate state regulation of health insurance products sold to individuals and small businesses (CMS, 2010).
The other key piece of legislation regarding the regulation of third-party payers is ERISA, enacted by Congress in 1974 (CRS Report for Congress, 2009). ERISA regulations fall under the Department of Labor, in contrast to McCarran-Ferguson’s focus on state-level regulation. They set minimum standards to protect individuals participating in most voluntarily established pension and health insurance private sector employee benefit plans (i.e., self-insured employers). ERISA does not require that private employers offer health insurance but governs the administration of these plans if employers self-insure and defines how disputes are handled. Group health plans established by government or church organizations and plans that only apply to workers’ compensation or disability, or unemployment are not governed by ERISA (US Department of Labor, 2019). Regulations of employer-sponsored health insurance plans imposed by ERISA include the requirement that plans provide enrollees with information about plan features and funding, fiduciary responsibilities for managers of plan assets, and procedures for establishing grievances, appealing denied claims for benefits, and rights to sue for benefits and breach of fiduciary duties (US Department of Labor, 2011).
Pre-emption of state regulatory laws is an important cornerstone of ERISA. US courts have upheld that ERISA pre-empts certain state health policies, such as employer insurance mandates, financial reserve requirements, premium taxes and managed care standards, placing constraints on states’ abilities to regulate insurance benefits and enact health care reforms (Butler, 2000; Gabel, Jensen & Hawkins, 2003). The pre-emption was included by Congress to “avoid multiplicity of regulation in order to permit nationally uniform administration of employee benefits” for employers with workers in multiple states (CRS Report for Congress, 2009). However, ERISA does not regulate benefits to the extent that the states do. Employer insurance plans that fall under ERISA have different (and often less comprehensive and less expensive) benefit structures than employer-sponsored plans that fall under state insurance regulations.
About 60% of employees covered by employer insurance were enrolled in self-insured plans in 2015, and are therefore affected by ERISA’s pre-emption of state regulation (Fronstin, 2016; Gabel, Jensen & Hawkins, 2003; Pierron & Fronstin, 2008). Although ERISA broadly pre-empts state laws governing the administration of health plans and definition of how grievances are resolved, as noted earlier, states regulate many other components of the third-party payer market. Since its enactment in 1974, there have been several substantial amendments to ERISA. The Consolidated Omnibus Budget Reconciliation Act (COBRA) of 1985 provided some workers and their families the right to continue their health care coverage for a limited time after job loss and other specific events (US Department of Labor, 2011). This is significant because, as mentioned earlier, nearly half of Americans receive their health insurance coverage through their employer. The Health Insurance Portability and Accountability Act (HIPAA) of 1996 amended ERISA to include limitations on exclusions from health insurance coverage based on pre-existing medical conditions events (US Department of Labor, 2011). The Mental Health Parity Act of 1996 was added to ERISA so that health insurance plans offering mental health coverage had annual and lifetime benefits on a par with those for medical and surgical benefits (US Department of Labor, 2011). The final two amendments to ERISA – the Newborns’ and Mothers’ Health Protection Act passed in 1996 and the Women’s Health and Cancer Rights Act passed in 1998 – respectively established minimum maternity lengths of stay and covered reconstructive surgery after mastectomies (US Department of Labor, 2011).
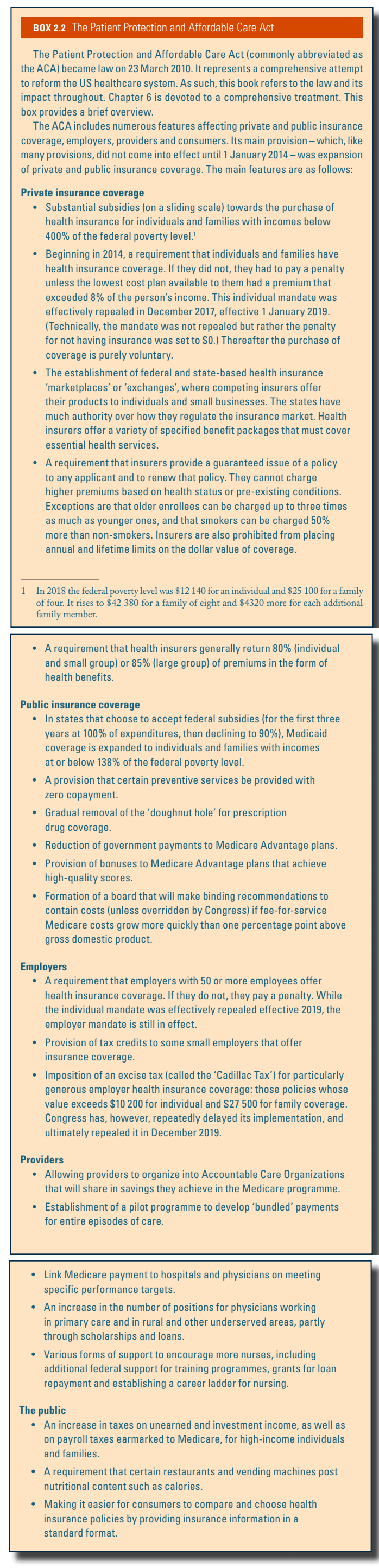
The 2010 ACA included several new regulations governing the third-party payer market. These are discussed in Box2.2 and Chapter 6. Most importantly, health plans are required to offer and renew coverage to everyone and cannot charge more to those who have pre-existing health conditions.
Box2.2
2.7.2. Regulation of providers
Physicians and hospitals are regulated by public agencies at the federal and state level and by national nongovernmental and provider regulatory organizations. Physicians, as well as nurses and many allied health professionals, are accredited by licensing boards in the state in which they practise. State licensing boards issue new licences to health care professionals with the requisite educational credentials, renew licences and enforce basic standards of practice through their power to suspend or revoke licences to practise (Field, 2007).
In addition to state-level regulation, physicians are also regulated at the federal level by the CMS imposing criteria for reimbursing providers for services rendered. For example, Medicare requires physicians to meet certain requirements, many of which overlap with state-licensing requirements (CMS, 2011a). Since Medicare patients make up a significant portion of many physicians’ payer mix, the requirements for reimbursement serve as a form of provider regulation. Furthermore, the CMS does not reimburse physicians for self-referred services. Also known as the Stark Law, this regulation prohibits payment to physicians for referrals to services in which they or their family members have a financial interest (CMS, 2011b).
Physicians are also regulated by managed care organizations (e.g. HMOs, PPOs) and by the hospitals at which they practise or have admitting privileges. Through various mechanisms for controlling costs (e.g. capitation, gatekeeping and pre-authorization) and improving quality (e.g. disease management), managed care organizations regulate physician behaviour. Managed care organizations also give credentials to physicians in their network, again ensuring providers are able to demonstrate basic requirements to practise similar to those required by state licensing boards and the CMS. Physicians may be disciplined by managed care organizations through exclusion from the network. Hospitals at which physicians practise also regulate physicians through providing credentials and periodically renewing them. Hospitals oversee physician practice through review boards and can discipline physicians for substandard care by requiring additional medical education or supervision by colleagues, or suspension or revocation of clinical privileges (Field, 2007).
Hospital regulation in the United States occurs primarily via certification requirements by the nongovernmental Joint Commission, by federal law on who must be treated at hospitals, and by eligibility for reimbursement criteria imposed by the CMS. Some of the most important hospital oversight results from the self-policing role of accreditation by the Joint Commission. This organization is a nongovernmental regulatory body that includes more than 4000 hospitals (77%) in the United States (Joint Commission, 2017). Auditors from the Joint Commission survey hospitals, unannounced, and evaluate compliance with Joint Commission standards by tracing care delivered to patients, acquiring documentation from the hospital, tracking hospital quality measures and on-site observation. Annual fees for hospitals range from US$ 2000 to US$ 37 000. Re-accreditation surveys occur every three years (Joint Commission, 2017).
The Emergency Treatment and Active Labor Act (EMTALA), passed in 1986, requires that all hospitals participating in Medicare provide “a medical screening examination when a request is made for examination or treatment for an emergency medical condition, including active labor, regardless of an individual’s ability to pay” (CMS, 2011c). After screening, hospitals are required to stabilize patients with emergency medical conditions or, if they are unable to stabilize a patient (e.g. due to capacity constraints), transfer the patient for stabilization. As a result of EMTALA, the emergency department has become an access point commonly used by patients with otherwise limited access to primary care (e.g. the uninsured).
As a result of the Hill-Burton Act, discussed in section 2.1.4, many US hospitals are required to take Medicare and Medicaid patients and are therefore subject to CMS eligibility criteria for reimbursement through conditions of participation (CoPs) and conditions for coverage (CfCs). The CMS is able to regulate hospital care by ensuring facilities receiving CMS reimbursement meet minimum quality and safety standards (CMS, 2011d). In fact, these conditions for participation and coverage also apply to many other health services delivery organizations (e.g. nursing homes, psychiatric hospitals). The conditions laid out by the CMS cover most of the essential components of hospital or other health services facilities, including requirements for staffing, patients’ rights and medical records.
2.7.3. Regulation of pharmaceuticals
Pharmaceuticals in the United States are primarily regulated at the federal level by the FDA. The present-day FDA evolved from legislation adopted in 1906 in response to public health epidemics resulting from unsafe foods and drugs.
The FDA approval process for new drugs or biological products consists of animal testing and then four phases of testing in humans, three of which are completed before the drug can go on the market and the last continues on after the drug has been released. The clinical trials stage often takes several years, with costs largely borne by the sponsor (e.g. the drug manufacturer). However, for biological products the ACA included new statutory provision to expedite the FDA approval process for drugs that are “biosimilar” with an FDA-approved biological product (FDA, 2012). Use of biosimilars is estimated to save the US health care system approximately US$ 44 billion between 2014 and 2024 (Boccia et al., 2017).
Like the European Medicines Agency, the FDA does not require economic analyses of drugs during the approval process. Therefore, drugs need only be effective, not cost-effective or comparably effective, for FDA approval.
With the passage of the ACA in 2010, the federal government is stepping up research on comparative effectiveness (Kaiser Family Foundation, 2011a). The ACA created the Patient-Centered Outcomes Research Institute (PCORI), a public–private organization that funds comparative effectiveness research (Iglehart, 2010). Funds come from Medicare and private insurers. The PCORI has a research agenda based on private stakeholder recommendations rather than government or scientist-initiated recommendations. The ACA charges the private stakeholders to focus on technologies for the most common conditions, especially chronic ones, and those affecting minorities. The research cannot include cost-effectiveness.
The FDA also regulates pharmaceutical advertising through its labelling requirements and its ability to penalize drug companies conducting advertising it deems excessive or misleading. From the 1990s drug companies started advertising directly to consumers. Among the high-income countries, the United States is one of the few to permit direct-to-consumer advertising of prescription-only drugs (Magrini, 2007). While no laws exist in the United States preventing drug companies from advertising prescription drugs to consumers directly, the FDA can prosecute manufacturers for advertising that is false or misleading.
The United States does not have national price regulations on pharmaceuticals, although Medicaid and the VA are exceptions (Adams, Soumerai & Ross-Degnan, 2001). Drug manufacturers in the United States hold de facto monopolies in the pharmaceutical market for a drug, often resulting in much higher prices compared to some other countries. Prior to 1984, generic versions of branded drugs were held to the same standard of the four-phase clinical trial process. This stymied the entry of generics into the market. In 1984 Congress adopted legislation that would allow generics to use some of a branded drug’s FDA safety and efficacy data in exchange for extending patents on branded drugs from 20 to 25 years (Field, 2007). Under the ACA, the FDA can approve generic biological products after 12 years of patent protection to further promote the use of generics (Kaiser Family Foundation, 2011a).
During the 1980s, in an effort to rein in spending on pharmaceuticals, states began repealing anti-substitution laws and enacting substitution laws to facilitate the prescribing and filling of cheaper therapeutic alternatives to branded drugs (Field, 2007). The Medicaid Drug Rebate Program, created in 1990 as part of the Omnibus Budget Reconciliation Act, required pharmaceutical companies to give states and the federal government rebates for drugs sold to Medicaid and VHA patients (CMS, 2011e). Approximately 600 drug companies participate in the rebate programme, a requirement for Medicaid drug coverage, with rebates ranging from 13% to 23% of the average manufacturer price (AMP) for the drug (CMS, 2017).
The United States does not allow the re-importing of drugs previously manufactured in the United States but sold at lower prices in foreign markets or the importing of drugs by individuals directly from foreign producers. The 1987 Prescription Drug Marketing Act made it illegal for drugs to be imported into the United States except by the original US manufacturer. The ACA continued the ban on importation of prescription drugs (see Chapter 6). Legislative solutions to rising drug costs have managed to evade Congress over the past few decades.
2.7.4. Regulation of medical devices and aids
In addition to regulating pharmaceuticals, the FDA is also the principal regulator of medical devices and radiation-emitting products used in the United States. The FDA’s Center for Devices and Radiological Health (CDRH) regulates firms that manufacture, repackage, relabel and/or import medical devices and radiation-emitting electronic products (medical and nonmedical), such as lasers, X-ray systems, ultrasound equipment, microwave ovens and colour televisions (FDA, 2011a). The CDRH divides medical devices into Classes I, II and III, with the level of regulatory control increasing with the class. Generally, Class I devices are exempt from FDA notification before marketing, most Class II devices require premarket notification and most Class III devices require premarket approval from the FDA. The FDA also monitors reports of adverse events and other problems with medical devices and alerts health professionals and the public when needed to ensure proper use of devices and the health and safety of patients (FDA, 2011b).
The Inflation Reduction Act of 2022 initiated several reforms to Medicare prescription drug coverage. Two notable ones are a $2,000 annual out-of-pocket limit for Medicare-covered prescription drugs (beginning in 2025) and implementation of negotiation of Medicare drug prices (beginning in 2026). One of the earliest changes begins in 2023, when patient cost-sharing requirements for insulin are limited to $35 per month. Millions of seniors are expected to pay less for insulin after the $35 monthly cap as average monthly out-of-pocket spending on insulin was estimated at $58 in 2020, with 37% of beneficiaries paying more than $35, and 24% more than $70.
References
U.S. Department of Health and Human Services. Assistant Secretary for Planning and Evaluation. “Insulin Affordability and the Inflation Reduction Act: Medicare Beneficiary Savings by State and Demographics.” January 24, 2023. https://aspe.hhs.gov/sites/default/files/documents/bd5568fa0e8a59c2225b2e0b93d5ae5b/aspe-insulin-affordibility-datapoint.pdf
2.7.5. Regulation of capital investment
Federal-level regulation on capital investment arose with the Hospital Survey and Construction Act of 1946 – also referred to as the Hill-Burton Act – and also the National Health Planning Law of 1974. The Hill-Burton Act provided construction funds to increase the capacity of health services throughout the country. In exchange for the funds, hospitals, nursing homes and other health facilities were required to provide a certain amount of uncompensated care to individuals living in the area (US Department of Health and Human Services, 2010b). Hill-Burton funds were distributed through local and state health planning boards. These boards in turn regulated the construction of the facilities built within their jurisdiction. The certificate of need (CON) programme is discussed in more detail in section 2.1.4.
From 1972 to 1995 the Office of Technology Assessment (OTA) aided Congress in the identification and consideration of existing and probable impacts of technologies, including medical technologies (Federation of American Scientists, 2011). During its existence, the OTA conducted a number of cost-effectiveness studies related to capital investment so as to inform regulators about policy decisions regarding these investments. The OTA was similar to government offices in other high-income countries in its cost-effectiveness research. In 1995 Congress de-funded the OTA (Princeton University, 2012).
2.7.6. Regulation of patient privacy and human subjects
Regulations regarding the privacy of health information in the United States were initiated in the HIPAA Privacy and Security Rules passed by Congress in 1996. The privacy component of the law provides federal protection for personal health information and gives patients rights with respect to that information (US Department of Health and Human Services, 2011b). The security portion has administrative, physical and technical safeguards to ensure the confidentiality of patient information. HIPAA Privacy and Security Rules are enforced by the Office of Civil Rights under the HHS. The Patient Safety and Quality Improvement Act of 2005 (PSQIA) patient safety rule protects “identifiable information being used to analyse patient safety events and improve patient safety” (US Department of Health and Human Services, 2011b). The PSQIA of 2005 requires disclosure of medical errors to affected patients while protecting those who report the errors by not allowing voluntary admissions by providers to be used against them in a court of law (Howard et al., 2010).
The Office for Human Research Protections (OHRP) within the HHS regulates the protection of human subjects used in clinical and nonclinical research. Its purview “applies to all research involving human subjects conducted, supported or otherwise subject to regulation by any federal department or agency” and includes “research conducted by federal civilian employees or military personnel” and “research conducted, supported, or otherwise subject to regulation by the federal government outside the United States” (OHRP, 2011). Since the vast majority of the research on health in the United States is funded by various government grant mechanisms or regulated by some federal agency, OHRP regulations regarding human subjects research affect much of the research involving people. In addition to the OHRP, many individual research institutions, such as universities, also have departments that verify whether human subjects research is warranted and will be conducted safely, effectively and with dignity.
2.7.7. Regulation of public health
Regulation of public health occurs at multiple levels of government. At the federal level, the CDC (discussed earlier), the EPA, the United States Department of Agriculture (USDA) and the Occupational Safety and Health Administration (OSHA) all regulate various aspects of public health. State and local offices of public health also play important roles in regulating public health.
The United States has 50 state-level public health agencies. In addition, many of the more than 3000 counties and 15 000 municipalities have some type of local health department or have their own public health regulations (Diller, 2007). These governmental agencies regulate a range of public health topics including: air quality, alcohol, animals, cemeteries and burial, communicable diseases, emergency medical services and ambulances, fair and affordable housing, firearms, food, garbage collection and disposal, housing and building codes, mass gatherings, massage establishments, noise, nuisances, pest control, restaurants, sewer systems, smoking, swimming pools and spas, tobacco sales and water wells (McCarty et al., 2009).
The USDA regulates and inspects food services, including production. It also recommends nutritional guidelines and the fortification of certain food staples (e.g. milk, bread, salt), regulates the import and export of animals and plants, and regulates the marketing of foods (US Department of Food and Agriculture, 2011).
The EPA regulates public exposure to harmful environmental contaminants. In 1970 Congress passed the National Environmental Protection Act, the Clean Water Act and the Clean Air Act, giving the newly created EPA the authority to establish and enforce environmental protection standards (US Environmental Protection Agency, 2011). The EPA’s reach expanded in 1980 when Congress, in response to chemical contaminants in groundwater from toxic dumps, passed the Comprehensive Environmental Response, Compensation and Liability Act (CERCLA). This gave the EPA the charge of cleaning up toxic waste at “Superfund” sites, assessing liability and financial responsibility for the contamination, and suing to recover clean-up costs (US Environmental Protection Agency, 2011).
The OSHA also plays a role in public health regulation. Its charge is to mitigate the harm caused from employee exposure to workplace hazards through regulation and training (OHRP, 2011).
Federal, state and local agencies share responsibility for regulating abused substances and other public health threats such as gun violence. The following paragraphs discuss these regulations. At the federal level, the FDA not only regulates food, drugs, vaccines and biological products, and medical devices, but includes regulation of tobacco products in its purview. The FDA’s Center for Tobacco Products (CTP) employs a public health approach to regulate cigarettes, cigars, hookah, electronic vapor products, pipe tobacco and other tobacco products, in accordance with the 2009 Tobacco Control Act. The CTP sets manufacturer requirements, rules regarding the sale and distribution of products, marketing, advertising and product packaging, among others (FDA, 2018). In addition to FDA regulation, states, localities and tribal governments all maintain authority to regulate some aspects of tobacco product use, marketing and distribution. States and local entities have the power to raise tobacco tax rates, enact smoke-free laws in public places, fund tobacco prevention campaigns, place some limits on marketing and advertising, implement counter-marketing and anti-smuggling campaigns, enable access to tobacco cessation programmes and products, and restrict the sale, distribution and possession of tobacco products, including increasing the minimum legal age to purchase these products (Tobacco Control Legal Consortium, 2018).
Alcohol is regulated at the state and local level in the United States, since the 21st Amendment to the Constitution allows individual states to control the sale, distribution, importation and possession of alcohol within the state. States then frequently assign localities the responsibility to regulate alcohol in accordance with state standards. The Federal Uniform Drinking Age Act of 1984 established a federal minimum legal drinking age of 21, and federal law defines an alcoholic beverage as any beverage that contains more than 0.05% alcohol. The maximum level of alcohol (MLA) per drink varies by state, as do laws regarding licensure, penalties for non-compliance, and intoxication (American Addiction Centers, 2018). In addition, many states (14, plus the District of Columbia in 2011) still enforce “blue laws”, originating from Christian religious beliefs, which restrict the sale of alcohol on Sundays (Lovenheim & Steefel, 2011).
Cannabis is another product regulated at the federal and state level. While it remains illegal to possess or use cannabis under federal law, some states have chosen to legalize medical and/or recreational use of cannabis in recent years. As of 2018, 33 states and the District of Columbia have approved comprehensive medical cannabis/marijuana programmes protecting some consumers of cannabis for approved medical reasons from criminal liability, and offering access to cannabis at approved dispensaries. Thirteen additional states had limited access medical programmes, and 10 states and the District of Columbia have legalized marijuana for adult recreational use. While cannabis distribution remains illegal at the federal level, the US Department of Justice allows federal prosecutors broad latitude to decide how they will prioritize enforcement of federal law, offering them the opportunity to defer to state-based enforcement efforts if appropriate (NCSL, 2018b).
Gun violence has been named a public health issue in the United States by leading organizations such as the AMA, and more than 100 medical organizations signed a letter to Congress in 2016, asking members to lift the Dickey Amendment. The Dickey Amendment, passed in 1996, forbids the CDC from using any federal funding to “advocate or promote gun control”, though its mission includes investigation into accidental death and injuries, as well as suicide, to which gun violence contributes (Zhang, 2018). In addition, the Bureau of Alcohol, Tobacco, Firearms and Explosives is prohibited from sharing data with either the NIH or the CDC. Lack of funding and lack of available data have been some of the factors hindering regulation of guns to reduce the public health burden of gun violence in the United States (Evans & Anthony, 2018).
2.7.8. Health technology assessment
Health technology assessment (HTA) is the evaluation of the effectiveness, safety, costs and patient-reported outcomes of health care technology with the aim of informing health policy-making (Sullivan et al., 2009). HTA is conducted in the United States by public and private payers, universities, hospitals, research institutes and manufacturers. HTA has a long history in the United States. However, several earlier organizations which conducted HTAs, such as the OTA, no longer exist due to lack of funding as well as political pressures (Sullivan et al., 2009). Since the de-funding of the OTA, the US Government Accountability Office (GAO) has performed technology assessments, but these are not specifically HTAs.
Currently, on the federal side, Medicare conducts HTA through the Medicare Evidence Development and Coverage Advisory Committee (MedCAC), an appointed body of national experts on medical technology that holds public meetings to examine the evidence regarding health technologies. Cost-effectiveness cannot be part of the consideration. CMS places the evidence presented at the committee meetings and final coverage policies on the CMS website. Assessment of pharmaceuticals covered by Medicare is separate from this process. Medicare coverage of pharmaceuticals – the Part D programme – is a privately administered benefit, so all pharmaceutical coverage decisions are made by Part D private contractors, with the exception of coverage restrictions placed by Medicare.
The AHRQ is the largest federal funder of HTA research (Sullivan et al., 2009). It conducts systematic reviews to assess the effectiveness, comparative effectiveness and safety of medical technologies and interventions. The AHRQ’s Technology Assessment programme provides technology assessments for the CMS.
Both the federally run VHA and the Military Health System (MHS) conduct HTAs on pharmaceuticals to help with decision-making regarding medications to use within these systems. The VHA does this through the Pharmacy Benefits Management Strategic Healthcare Group (PBMSHG), whereas the MHS does this through the Department of Defense Pharmacoeconomic Center (PEC).
The FDA does not conduct formal technology assessments of pharmaceuticals but instead evaluates the safety and efficacy of drugs by providing research guidelines and reviewing the studies conducted by external researchers. The FDA focuses on controlled trials of the effectiveness and safety of each drug rather than studies of the comparative effectiveness of drugs (see section 2.7.3).
At the state government level, many Medicaid programmes support HTA for pharmaceuticals and medical technologies (Sullivan et al., 2009). Although these HTA programmes are usually administered by state Medicaid staff with support from clinical experts, state administrators often purchase HTAs from private organizations. Budgets for HTAs usually come from the state alone (no federal support). Medicaid agencies in 14 states have relied on pharmaceutical evaluations conducted by the Drug Effectiveness Review Project (DERP), created in 2001 by the Oregon Health and Sciences University. The publicly available reports from DERP have a description of the HTA issues, a description and synthesis of the relevant literature, and a judgement on the quality of the evidence. Cost-effectiveness is not considered, and the reports do not provide recommendations about coverage.
Many of the larger private insurers and pharmacy benefit management companies have HTA programmes with their own researchers, financial analysts and data systems (Sullivan et al., 2009). Smaller health plans have more limited abilities to conduct the research internally, and often depend on HTAs from external private or public agencies. Most private organizations consider their HTA programmes to be proprietary.