-
15 August 2025 | Country Update
Slovakia’s €2 billion ambulance tender sparks political and legal turmoil -
15 August 2025 | Policy Analysis
Out-of-pocket payments in Slovakia reach EUR 1.7 billion with very low transparency and high legal uncertainty -
15 July 2025 | Policy Analysis
Steps to reform emergency medical services in Slovakia -
22 July 2024 | Country Update
Political interference in the Slovak health system -
16 February 2024 | Policy Analysis
Slovakia’s Health Care Surveillance Authority’s lacking institutional stability and independence -
30 June 2023 | Policy Analysis
Financial losses at the state-owned insurer (VšZP) and the corresponding recovery plan -
14 October 2022 | Country Update
Tighter regulation of health insurance companies and supervision of health care -
10 October 2021 | Country Update
Reform to regulate the profits of HICs -
15 October 2020 | Country Update
Changes to redistribution revenue mechanisms for health insurance companies -
12 February 2020 | Country Update
Quality assurance and waiting times in inpatient care reregulated -
14 July 2019 | Policy Analysis
A Revision of the reimbursement decision technicalities -
31 December 2017 | Country Update
General Health Insurance Company (GHIC) and its recovery plan (2016–2017)
2.8. Regulation
In terms of regulation, the main actors in the Slovak health system are the parliament, the central government, and the Ministry of Health and its subsidiary organizations, as well as the SGRs. The parliament as a legislative body passes the acts. The legal environment in health care is significantly influenced by general acts, including the Commercial Code, the Civil Code and the Labour Code. As executive bodies, the government and the Ministry of Health enact secondary legislation (regulations, decrees, rulings, measures, guidelines) with different legal liability and law enforcement. The HCSA is responsible for monitoring health insurance, health care purchasing and health care providers, and also enforces the regulatory framework. The role of the HICs in system regulation results from their competences as purchasers of health care services. This includes maintaining the conditions of selective contracting and flexible pricing.
The Constitutional Court of the Slovak Republic rules on whether or not laws conflict with constitutionally established rights. The Constitution of Slovakia stipulates that every person shall have the right to protect his or her health. Through medical insurance the citizens have the right to free health care and medical equipment under the terms provided by law. The law sets the scope of free health care in general, and subordinate legislation defines specific proceedings (see section 2.2).
Fig2.2 schematically depicts the regulatory framework in Slovakia, which will be elaborated upon in the following sections.
Fig2.2

Slovakia is facing a major public procurement controversy involving the tendering of its emergency medical services. The EUR 2 billion contract, covering both ground and air ambulance operations from 2025 to 2031, has become the largest healthcare tender of the current government – and is now mired in allegations of cronyism, lack of transparency and possible breaches of procurement law. Political tensions, media scrutiny and prosecutorial involvement have converged to make this one Slovakia’s most significant governance crises of 2025.
Tender overview
The Operational Centre of the Emergency Medical Service, on behalf of the Ministry of Health, launched the tender to allocate licences for 344 ground ambulance stations and 7 air ambulance bases nationwide in May 2025. The aim was to ensure the provision of high-quality, continuous emergency services across Slovakia. The winning bidders would secure operational rights for a six-year period, with the contract value estimated at EUR 2 billion (The Slovak Spectator, 2025a).
Transparency concerns
Criticism quickly emerged from opposition parties, the Slovak Medical Chamber and transparency watchdogs. They highlighted opaque selection procedures, including a refusal to disclose the names and qualifications of tender committee members.
In July 2025, preliminary results of the tender and the names of the commission members were leaked to the media, which confirmed concerns about poor transparency and fairness of the tender (The Slovak Spectator, 2025a).
One particularly contentious claim is that the tender process might be structured to favour certain bidders, notably Agel SK, Slovakia’s second-largest private healthcare provider, and a relatively unknown entrant, Emergency Medical Solutions (EMS). Both have reportedly been in positions to gain a disproportionately large share of contracts (The Slovak Spectator, 2025b). EMS was later proven to be linked to the second largest coalition party, HLAS-sociálna demokracia, which also nominated (as of this writing) incumbent Minister of Health, Kamil Šaško.
As a consequence, on 8 August 2025, Penta Hospitals, Slovakia’s largest private healthcare network, withdrew its bid, citing serious concerns over transparency and suggesting possible breaches of EU procurement law (The Slovak Spectator, 2025b).
The Slovak National Party (SNS), another governing coalition partner, demanded not only the cancellation of the tender but also the resignation of Health Minister Šaško. Prime Minister Robert Fico publicly acknowledged that the process could be scrapped or restarted if doubts persisted (TASR, 2025).
The General Prosecutor’s Office, led by Maroš Žilinka, initiated a preliminary review into the tender process. This action signals potential criminal investigations for alleged mismanagement of public funds and violations of procurement rules (The Slovak Spectator, 2025b).
Nevertheless, the management of the Operational Centre of the Emergency Medical Service delivered the results of the tender to the Ministry of Health on 11 August, thereby de facto announcing the successful selection procedure. On the same day, Minister of Health Šaško, announced that he would not sign it and would cancel the tender procedure, and would come up with an alternative for procuring emergency services in Slovakia, pending agreement within the governing coalition. Conclusions of such discussions are expected by the end of August 2025.
The opposition and experts claim that Health Minister Šaško could not terminate the tender and did so in violation of the law, which may cause the bidders to suffer lost profits, and are therefore demanding his resignation (TASR, 2025b).
References
The Slovak Spectator (2025a) News digest: Unqualified officials, secret committees. Ambulance tender raises red flags. SME.sk. Available at: https://spectator.sme.sk/politics-and-society/c/news-digest-unqualified-officials-secret-committees-ambulance-tender-raises-red-flags (Accessed: 15 August 2025).
The Slovak Spectator (2025b) News digest: Ambulance tender turmoil – Penta walks, prosecutor limbers up. SME.sk. Available at: https://spectator.sme.sk/politics-and-society/c/news-digest-ambulance-tender-turmoil-penta-walks-prosecutor-limbers-up (Accessed: 15 August 2025).
TASR (2025) Ambulance tender scandal: Political pressure mounts, PM and SNS weigh in. TASR. Available at: https://www.tasr.sk/tasr-clanok/TASR%3A2025080700000344 (Accessed: 15 August 2025).
TASR (2025b) According to Šaško, the tender for ambulances was cancelled in accordance with the law. “Anyone who questions this is lying”, he said. PRAVDA. Available at: https://spravy.pravda.sk/domace/clanok/763156-sasko-tender-na-zachranky-bol-zruseny-zakonnym-sposobom Accessed: 15 August 2025).
In 2023, total out-of-pocket spending (OOP) in Slovakia reached EUR 1.7 billion EUR, and just over 18% of current heealth expenditure. At the same time, OOP payments are legally inconsistent, economically inequitable and lack transparency (see Table 1). Analysis of OOP spending reveals several key issues:
Low transparency and information asymmetries
Patients often do not know what exactly they are entitled to, do not understand the differences between a fee and a co-payment, or betweenstandard and above-standard service. Patients are often not informed by providers of these differences. Patients are often not issued receipts in practice, further reducing transparency.
There is also a variation in patients‘ readiness to pay, with some unwilling or unable to do so. Some are unwilling based on the principle of free healthcare at the point of service, while others, especially in poor regions, simply cannot afford to pay. There are also those willing to pay OOP, giving them priority and more adequate consultation times, scheduled appointments, and an individual, higher-quality approach.
Gaps in regulation, inconsistent approaches and legal uncertainties
There legal uncertainty surrounding the interpretation regarding providers’ ability to charge fees. After approximately 600 amendments since their adoption, laws 576, 577, and 578 of 2004 (core laws underpinning the major 2004 health system reform) create contradictory motivations for providers.
As stated by providers, a main reason for rising fees is due to insufficient reimbursements from insurers, leading them to seek alternative sources of funding to try to maintain levels of care quality. Other given reasons include rising staff wages (especially in public hospitals), the introduction of a transaction tax, general inflation across the economy and increasing energy costs.
Beginning in 2006, legal restrictions against direct payments were introduced. However, in practice, a chaotic “fee jungle” has emerged, with exploitation of numerous legal loopholes. This is also reflected in the varying levels of patient information (differing communication and price list publication methods), reducing predictability of patient costs.
Furthermore, the absence of regulation has led to variability in the fees charged among providers even within the same specialty. Price lists reveal regional differences: the highest charges are in Bratislava (sometimes multiple times higher), while in smaller towns or rural areas, fees tend to be lower or nonexistent.
Finally, an outdated performance catalogue does not reflect technological progress nor current market prices for materials. Notably, the catalogue was originally intended as a tool for introducing innovation (for example, telemedicine, AI, interventional radiology), not solely as a pricing mechanism.
Table 1: Legislative anchoring of direct payments and their relationship to public health insurance
| Occurrence of direct payment | Purpose of direct payment | Legislative basis |
| Before provision | Patient management | Act 576/2004 allows for charging for services beyond standard public coverage. However, annual care program services may be covert payments for services that should be free (Act 577/2004 prohibits fees for appointment scheduling, priority treatment, and administrative tasks). There are often collected by intermediaries (not the providers themselves); the healthcare service itself is reimbursed by an insurer. |
| Reservation portal | Legal loophole: current laws prohibit providers from charging for scheduled appointments.
Exploited by third-party private companies offering booking systems independent from the state and healthcare providers. | |
| During provision | Fees for services related to care provision. | Regulated in §38 of Act 577/2004 in which Slovakia’s Constitutional Court confirmed that such charges are constitutional. |
| Co-payments for medicines, medical aids, durables and materials and dietetic food | Yes, most clearly regulated type.
Defined entitlements and transparent costs for both insurer and patient. | |
| Direct payments to non- contracted providers | Governed by commercial code | |
| Price list fees | Partially regulated: not clearly defined in Act 577/2004 and indirectly referenced in Act 578/2004 requiring a public price list submitted to regional authorities Legally questionable in some cases (e.g., booking fees, prescription printing, spa referral), and often charged due to outdated reimbursement catalogue or lack of coverage in practice. | |
| After provision | Second opinion | While not explicitly defined in law or reimbursement systems, this is usually billed to insurers as a regular consultation or repeat exam. Sometimes charged separately, especially for advisory consultations. |
Source: Pažitný et al. 2025
An examination of the health financing in Slovakia’s specialized outpatient care sector reveals a fragmented landscape of patient cost sharing and direct payments. Legal ambiguity, regulatory inconsistency and increasing financial burdens for patients create significant challenges for fairness, transparency and sustainability. Key areas for reform, not only to simplify rules and protect patients but also to restore trust and ensure long-term sustainability of the health system could include the following:
- Legalizing all types of co-payments – being clearly defined in Act 577/2004 and making any fees and co-payments transparent and understandable.
- Extend informed consent – informing patients of the amount in advance and for what service they are paying.
- Issue receipts for every healthcare service provided – an invoice showing exactly what services were provided, and what is paid by the insurer and what by the patient.
- Health insurers must be involved – informing insurers about any patient charges collected by providers.
- Introduce effective financial protection via co-payment limits – with eligible populations clearly defined.
- Shift the control of patient charges to regional authorities – via legislation to allow them to define scope and amount of allowed fees locally.
- Creation of a reimbursement mechanism to help cover some administrative costs – with the involvement of the Slovak Social Insurance Agency, health insurers and providers
References
Pažitný, Kandilaki, Macko-Forgáčová, Löffler, Zajac: Direct Payments in Specialist Outpatient Care in Slovakia, June 2025
Smatana, M. et al. (2025) in press. Slovakia: health system review 2024. Health Systems in Transition
As explained in a previous policy analysis (https://eurohealthobservatory.who.int/monitors/health-systems-monitor/analyses/hspm/slovakia-2016/slovakia-s-health-care-surveillance-authority-s-lacking-institutional-stability-and-independence), the Health Care Surveillance Authority (Úrad pre dohľad nad zdravotnou starostlivosťou in Slovak) plays an important regulatory role in the Slovak health system and is responsible for supervising health insurance, purchasing and healthcare markets. As with previous governments (no chair of the Health Care Surveillance Authority has served a full term since its establishment in 2004), the current government led by Prime Minister Robert Fico with Minister of Heath Zuzana Dolinková have politicized the role of the Authority’s chair. In February 2024, they used legislative amendments to §22 of Act 581/2004 to remove the then-incumbent Renáta Blahová.1, 2
More recently, the Fico government has adopted legislation to take effect on 1 August 2024 to change the criteria of who can serve as director of the National Institute for Value and Technologies in Healthcare (NIHO or Národný inštitút pre hodnotu a technológie v zdravotníctve), which was established in 2022 and is responsible for Health Technology Assessment in Slovakia. The new criteria specify that only a doctor or pharmacist could serve as head of the HTA agency (leading to the dismissal of the current head, Michal Staňák); the legislation also enables the Minister of Heath to dismiss the agency’s director at any time and without cause.
Besides the political sphere pushing itself into the decision-making levels of these two seemingly independent organizations within the health system, the current government has also used their existing authority to make the following changes in healthcare institutions and providers around the country since coming into office in October 2023 (the dates refer to when the officials were dismissed or replaced):
- Tomáš Janík, director of Faculty Hospital Trenčín, 14 November 2023.3
- Vladislav Šrojta, director of Faculty Hospital Trnava, 30 November 2023.4
- Pavol Bartošík, general director of Central Slovak Institute of Heart and Vascular Diseases (Stredoslovenský ústav srdcových a cievnych chorôb), 5 December 2023.5
- Ľubomír Šarník, director of Faculty Hospital Prešov, 6 December 2023.6
- Jozef Tekáč, director of Faculty Hospital Poprad, December 2023.7
- Eduard Dorčík, director of the hospital in Žilina, December 2023.8
- Peter Potůček, director of State Institute for Drug Control (Štátny ústav pre kontrolu liečiv), 31 December 2023.9
- Ľubica Hlinková, general director of VšZP (Všeobecná zdravotná poisťovňa), the state-owned Health Insurance Company, 10 January 2024.10
- Peter Lukáč, director of National Centre for Health Information (Národné centrum zdravotníckych informácií), 10 January 2024.11
- Ivan Kocan, director of University Hospital Martin, 10 January 2024.12
- Július Pavčo, director of Emergency Medical Service Operations Centre (Operačné stredisko záchrannej zdravotnej služby), 31 January 2024.13
- Renáta Blahová, Chair of Health Care Surveillance Authority, 6 February 2024.14
- Michal Fajin, director of Faculty Hospital Nitra, 14 February 2024.15
- Matej Mišík, chief of the Institute for Healthcare Analyses (Inštitút zdravotných analýz) at the Ministry of Health was revoked on 20.6.2024 without any reason. The Institute focuses on: epidemiological studies and data analysis, sector analysis and health policies, implementation of optimization of the hospital network and the development of the DRG reimbursement mechanism.16
- Michal Staňák, director of NIHO, according to legislation set to take effect on 1 August 2024, enabling the Minister of Health to dismiss the NIHO at any time and without giving a reason. The Ministry of Health has already published the announcement for the selection procedure for the position of the new director.17
Authors
References
1. https://spectator.sme.sk/c/23346445/slovak-health-minister-direct-power-independent-body.html
5. https://www.health.gov.sk/Clanok?mz-suscch-vedenie-nove
6. https://domov.sme.sk/c/23281567/fajin-nemocnica-nitra-dolinkova-pellegrini-hlas-rozhovor.html
7. https://domov.sme.sk/c/23272033/zuzana-dolinkova-zdravotnictvo-nemocnice-cistky.html
8. https://dennikn.sk/minuta/3744432
11. https://zive.aktuality.sk/clanok/SdYXsqi/odvolali-riaditela-nczi-kto-bude-na-cele
13. https://www.health.gov.sk/Clanok?operacne-zachranka-riaditel
14. https://www.tyzden.sk/zdravotnictvo/106251/vlada-odvolala-sefku-udzs-na-jej-miesto-zasadne-palkovic
15. https://domov.sme.sk/c/23281567/fajin-nemocnica-nitra-dolinkova-pellegrini-hlas-rozhovor.html
The Health Care Surveillance Authority (HCSA) plays an important regulatory role in the Slovak health system. Responsible for supervising health insurance, purchasing and healthcare markets, HCSA chairs are elected for five-year terms and are theoretically independent, given an irrevocable mandate as chair. This independence was written in the original legislation from 2004 that specified that a chair’s mandate could only end due to their own resignation, by power of the government (only after the chair committed an intentional crime) or the chair died.
Successive governments over the past two decades, however, have worked to install chairs corresponding to their particular (political) needs, given the prominent role the HCSA plays in regulation. Thus, through the years, changes of chair have become common after legislative amendments to §22 of Act 581/2004, the law that defines the conditions of a chair’s appointment and the revocation process (for example, clauses permitting the removal of the chair were added regarding subjective evaluations of the chair’s performance, or general (subjective) views of the Government that the chair cannot complete the mandate due to personal, moral or professional reasons). Since the establishment of the HCSA 20 years ago, not one of the seven chairs have served a full term (see Table 1): their mandates were either revoked (3x) or they resigned on their own (4x).
As no chair has served a full term, the record of longest term was Monika Pažinková, who served 75% of her term (2012–2016), while the shortest was under the first chair, Alexandra Novotná (2004–2005). Additionally, and crucially, the HCSA had no chair from the end of 2019 through the first year of the COVID-19 pandemic, a total of 553 days. Chairs are typically changed following parliamentary elections, so there is little overlap of incumbent chairs continuing to serve in a new government, even if their term is ongoing. There have also been four instances of new HCSA chairs coming into office within the first five months after parliamentary elections.
The four cases of chairs withdrawing from leading the HCSA include:
- Alexandra Novotná served for 150 days in 2005 (8% of the planned mandate duration). After establishing and stabilizing the institution, she relinquished her position to the State Secretary of the Ministry of Health, Ján Gajdoš, who decided to assume the role he had originally planned to take. As a result of her resignation, a position exchange occurred with the then-State Secretary, Ján Gajdoš [1].
- Ján Gajdoš after 703 days in 2012 (39% of planned term). His resignation came in reaction to an amendment of law 581/2004 that once again enabled the Minister of Health to remove the chair of the HCSA. Gajdoš cited disagreements with the politicization of the office of HCSA Chair and a de facto subordination to the Ministry of Health [2].
- Monika Pažinková after 1368 days in 2016. Pažinková became a symbol of patronage in office, being closely connected to businessmen from the city of Košice and the Smer political party [3].
- Tomáš Haško after 1269 days in 2019 because of irregularities in tender process for emergency vehicles that he oversaw [4].
The three cases of governments revoking mandates for HCSA chairs include:
- Ján Gajdoš after 663 days in 2007. While the Health Minister at the time (Valentovič) stated Gajdoš’ dismissal was the result of the office's performance given the state of healthcare in Slovakia at the time, Gajdoš himself considered it to be political, not professional [5].
- Richard Demovič after 1310 in 2010. He was dismissed by Health Minister Uhliarik using the same reasoning (poor performance) [6].
- Renáta
Bláhová after 1013 days in 2024. The Health Minister’s (Dolinková)
dismissal justified this by saying that Bláhová does not meet the
qualifications to be chair as required by law and that she is a
political nominee, appointed to the position of chair without a
selection process [7].
Increasing the institutional stability and independence of the regulatory frameworks (see for example, Balík (2012 [8])) and environment in Slovakia requires
- reestablishing the HCSA Chair’s independence by abolishing the legislative clause on their removal by the government without formal reason,
- strengthening the competences of the HCSA’s Board by transferring the decision-making powers from the chair, making the HCSA a collective decision-making body and not a single “one-person show”, and
- transferring the HCSA’s supervisory role over health insurance companies (HICs) to the National Bank of Slovakia and thus fulfilling an initial plan from 2004 when the HCSA was established.
The National Bank of Slovakia is an independent financial institution that could effectively supervise the financial situation of HICs. This would achieve the diversification of authority and preserve independence and resistance to political power, which is characteristic of regulators in other countries with competition-based systems (that is, multiple health insurers), like Germany (Federal Office for Social Security [9] and Federal Financial Supervisory Authority [10]), Switzerland (the Federal Office of Public Health [11] and the Financial Market Supervisory Authority (FINMA) [12]) and the Netherlands (The Dutch Healthcare Authority [13] and the Netherlands National Bank [14]).
Table 1

Authors
References
[1] https://hsr.rokovania.sk/329/125-schodze-vlady-slovenskej-republiky/?csrt=10869901077926702124
[2] https://www.trend.sk/spravy/sef-uradu-pre-dohlad-vzdal-funkcie
[4] https://domov.sme.sk/c/22242684/vlada-sr-odvolala-tomasa-haska-z-funkcie-predsedu-udzs.html
[5] https://domov.sme.sk/c/3108072/gajdos-povazuje-dovody-na-svoje-odvolanie-za-politicke.html
[6] https://domov.sme.sk/c/5521713/demovic-odchadza-z-uradu-nerad.html
[8] http://www.hpi.sk/cdata/Publications/regulacny_ramec_a_udzs.pdf
[9] https://www.bundesamtsozialesicherung.de/de
[10] https://www.bafin.de/EN/DieBaFin/diebafin_node_en.html
[12] https://www.finma.ch/en/authorisation/insurers/getting-licensed/health-insurance
[13] https://www.nza.nl/english
[15] https://www.udzs-sk.sk/urad/zakladne-informacie/predstavitelia-uradu
Given increasing budget constraints at the Ministry of Health, there was a need to raise extra revenues and at the same time reduce the number of fraudulent reinsurance among Slovakia’s health insurance companies (HICs). As such, the Ministry of Health has rolled out plans for a mixture of changes governing HICs, as well as clearer guidelines for the relationships between insurees and HICs. Among these changes was the introduction of minimum monthly contribution rates for all employees. More complex procedures for reinsurance were introduced to minimise reinsurance fraud, as well as a simpler and more transparent process for switching insurers.
Authors
Currently, health insurance companies (HICs) in Slovakia have the ability to turn a profit and pay shareholders dividends. The aim of this reform is to set a maximum amount of profit that the HICs can generate and take in. This reform has come about due to one of the private health insurance companies in Slovakia using creative accounting to pay out upwards of EUR 400 million to its shareholders over the past 15 years. The Ministries of Health and Finance were tasked with amending legislation and thereby setting a formula that determines what is the maximum profit that can be accumulated each year. The amendment to define a maximum level of profit was approved by the government in September 2022 and is set to be approved by the parliament (as of October 2022).
Authors
In 2020, with an Amendment to the Act on Health Insurance, the Ministry of Health began a second round of updates to the redistribution revenue mechanisms among Slovakia’s Health Insurance Companies (HICs). The main aim was to include ex-post redistributions to improve revenue streams to the state-owned General Health Insurance Company (VšZP). The Ministry of Health acted on the evidence that, despite having risk indices in place to redistribute costs, there remains a significant group of insured persons whose health care costs significantly exceed compensation. Thus, the “over-limit amount” element is being introduced into the redistribution process, which was initially part of the redistribution process in 2018, only to be subsequently removed. The measure is meant to bring roughly EUR 9.5 million into the VšZP’s annual budget at the expense of (private) Health Insurance Companies Dôvera and Union. The impact analysis was done on the basis of the previous year's data on the insured.
Changes in redistribution mechanisms
continued in 2020, with the introduction of an impact assessment on
devices and DCG groups, to be put in effect as of 1 January 2023.
Authors
Elective care will be one of the foundations to improve the
quality of in-patient services. By introducing a minimum number of
procedures per hospital (so called EBHR; see update from 31/1/2020 on
stratification) during the contracting process by HICs quality of these
services are assured. The MoH prepared the EBHR for a majority of
elective surgical cases in cooperation with professional medical
associations and chief experts of the ministry. As of February 2020, the
MoH had 258 procedures with a set limit defined. The EBHR limits were
supposed to be a part of the stratification reform, however they are to
be published separately by HICs in February 2020 in order to begin data
collection and the preparatory phase of centralisation of care.
All
EBHR regulated procedures have a set maximum waiting time to ensure
that concentration will not have a negative impact on accessibility of
services. There are several “categories” of waiting times, depending on
acuteness of a procedure i.e. procedures that have to be done within 1,
3, 6 and 12 months from indication.
Authors
Legislation in 2011 set standards to the price referencing system, that should be revised on a quarterly basis. A key rule was to ensure that the remuneration for a standard dose of drug in comparable groups is the same. These comparable groups were set according to a variety of traits, such as dosage, strength, ATC and the form of application. A lowered reimbursement could be partially or fully compensated by the manufacturer, or compensated by a higher patient co-payment.
Nonetheless, the Revision was not done properly since 2011. As a result, the reimbursement rates were not standardised, leading to higher level of prices for HICs paying for medicines and patients less on co-payments. A study conducted by the Institute for Health Policies and the Value for money unit (2018) estimated that a proper Revision could result in public savings to 64 mil. EUR and at least 50 mil. EUR, if social aspect e.g. the exclusion of vulnerable groups from OOP of co-payments would be taken into consideration.
This study initiated a Revision in autumn 2018 by the MoH, however, manufacturers refused to compensate for the decline in the level of reimbursements. Consequently, very high co-payments in a variety of drugs were expected. Patient organisations publicly demanded that the revision is not signed into law and the minister concurred (Folentová, 2018).
Additionally, the Revision had technical and practical problems as it was done for the first time. In February 2019, a Revision was passed and enabled a lot of technical changes (mainly in the higher number of reference groups and a possibility to set reimbursement rate for each group manually). The Revision is expected to save 39 mil. EUR from public funds and was put into effect as of 1st of July 2019.
Authors
References
Folentová (2018) Kalavská nedodrží zákon. Nepodpísala zníženie ziskov farmafiriem o 50 miliónov [Kalavska will not abide the law and will not sign the reduction of farma profits by 50 mil. EUR]. [Online] Available at: https://dennikn.sk/1296575/kalavska-nedodrzi-zakon-nepodpisala-znizenie-ziskov-farmafiriem-o-50-milionov/(accessed 28 July 2019).
Value for money unit (2018) Na prvom mieste pacient. Alebo farmafirmy? [Patient first. Or pharma lobby?] [Online] Available at: https://www.finance.gov.sk/sk/financie/hodnota-za-peniaze/blogy-uhp/na-prvom-mieste-pacient-alebo-farmafirmy/(accessed 28 July 2019).
In 2016, the GHIC (as the biggest out of three health insurance
companies) reported an accounting loss of 112 million EUR. Consequently,
the surveillance authority HCSA enforced a recovery regime during 2017
and pledged to balance its budget by 2018. The recovery regime comprised
a set of measures that aimed to curb expenses and internally
rationalise operations of the GHICs. The target was to contain a growth
in expenses and cut unnecessary expenses through renegotiations of
contracts with providers of MR, CT, inpatient services, dialysis units,
laboratories, and other auxiliary providers. As of the end of 2017, the
GHIC had achieved most of these targets and reported an accounting
profit of 35 million EUR, also as a result of a greater social insurance
income to the growing Slovak economy.
Authors
References
GHIC (2018) Rok 2017 skončila VšZP so ziskom 35 miliónov eur [GHIC
closed financal year of 2017 with a profit of 35 million EUR] [Online]
Available: https://www.vszp.sk/novinky/rok-2017-skoncila-vszp-so-ziskom-35-milionov-eur.html
2.8.1. Regulation and governance of third-party payers
HICs providing SHI have the role of third-party payers in the Slovak health system. They operate under private law and must be established as joint-stock companies. HICs are responsible for collecting contributions and purchasing health care. All HICs must operate nationwide, although their market shares show significant regional variation. This results in regional differences between HICs in negotiating positions vis-à-vis health care providers.
The HCSA issues licences for HICs. Legal conditions for issuing a licence include an issued share capital in a minimum of €16.6 million and transparent staff relations. Their owners appoint the members of the board of directors and the board of trustees. Regulations apply to the shareholders’ structure, staffing, and purchasing policy, as well as to the financial management of the HIC itself. The HCSA enforces these regulations and may impose sanctions. This may happen, for example, in cases of poor economic performance, if the HIC becomes seriously indebted or insolvent, or in cases of failure to comply with the public interest. Examples of these sanctions include imposing penalties, placing the company under forced management and revoking the operating licence.
HICs, like all other joint-stock companies, are obliged to undergo an audit of their accounting records. The HIC can propose an auditor but the HCSA may refuse this and assign another one. The HCSA submits biannual reports on the financial administration of HICs, as well as an annual budget proposal to the Ministry of Finance and the Ministry of Health. All HICs must submit their business plans to the HCSA and must publish annual reports via the Commercial Register. The HICs must publish all contracts with health care providers on their websites and also on the central register of contracts.
The (central) government plays an important role in regulating HICs. The government can dismiss the chair of the HCSA if the performance of the health insurance sector does not meet expectations. Furthermore, during the preparatory process of the state budget, the government also decides on additional financial sources for the system through changing the contribution rate for the state insured. Through the Ministry of Health, it defines the (minimum) benefits package, the minimum provider network, reimbursement policies for drugs, medical devices and dietetic food, whether user fees apply and maximum waiting lists. Lastly, the Ministry of Health is the only shareholder in the largest HIC, the GHIC. This enables the Ministry of Health to influence the company’s operating and purchasing policies. Moreover, due to its size the GHIC has strong influence over the entire health insurance market.
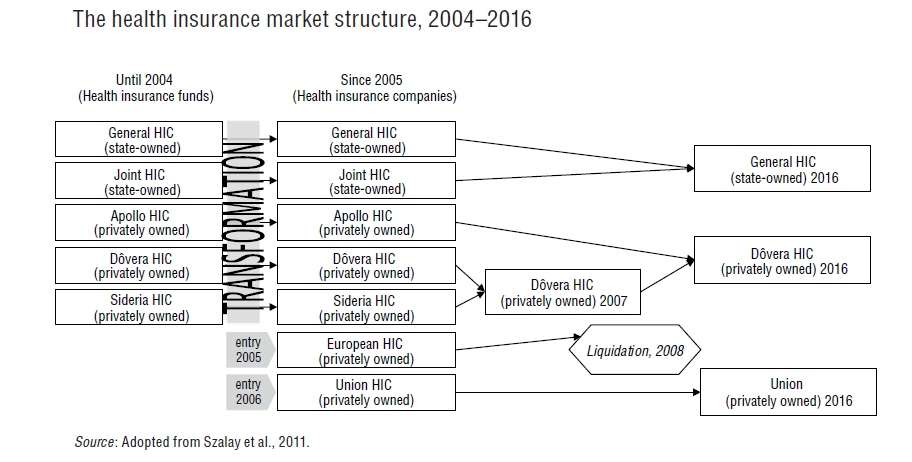
In the 2004 health reforms the hitherto existing public health insurance funds (operated by the state or industrial sector) were transformed into joint-stock companies, allowed to make profits and pay dividends to shareholders. The HICs must meet all the health care needs of their insured before being allowed to pay out profits to shareholders. During the three years after the reform two profit-oriented HICs entered the market, two companies merged to consolidate their portfolios, and one ceased operations as a reaction to the changed regulatory framework from 2008. From the beginning of that year HICs have been obliged to use all profits for purchasing health care in the following year (ban on profit). The possibility of making a profit from public health insurance was reintroduced in 2011 after a ruling of the Constitutional Court. In 2012 the Dutch HIC Achmea, owner of Union Health Insurance Company, won an international arbitration against Slovakia. According to this, Slovakia must pay €25.5 million in damages to Achmea as a result of the profit ban between 2008 and 2011 (see section 6.2).
After two more mergers, the market (as of 2015) consists of one state-owned HIC and two privately owned HICs (see Fig2.3). The total market share of the state-owned company GHIC dropped from 76% in 2005 to 64% in 2015.
Fig2.3
Despite this, in 2015 the health insurance market is very
concentrated, with a Herfindahl-Hirschmann index of 0.49. This indicator
measures the amount of competition among firms in an existing market in
relation to their sizes. As such, it can range from 0 to 1.0, moving
from a huge number of very small firms to a single monopolistic producer
(see Table2.2). Above 0.25 a market is seen as highly concentrated.
Table2.2

Timely
access to health care is regulated by the law. In general, waiting
lists should not exceed 12 months. Empirical findings indicate
considerable differences in the length of waiting lists between
different HICs.
Subordinate legislation issued by the Ministry of Health regulates only
three types of waiting list (implantations of artificial joints,
implantations of artificial lenses and heart interventions). This
prevents the HCSA from monitoring overall waiting times.
All three of Slovakia’s health insurers reported first-quarter losses in 2023, according to the Health Care Surveillance Authority (HCSA, 2023). The problem is expected to worsen, with a cumulative loss of approximately EUR 300 million expected for 2023, representing approximately 4% of the health insurers’ total revenues.
The biggest losses and most problems are faced by the state-owned VšZP, with annual losses estimated to be around EUR 240 million and its equity, that is, the value of its assets, falling into negative values by the end of the year. This would result in its liquidation as an insurance company.
Therefore, VšZP’s Supervisory Board, upon request from the Ministry of Health (MoH), prepared an analysis of the reasons for the losses along with a proposal for recovery measures at the end of May 2023. The Supervisory Board approved the proposal, and the MoH directed VšZP to implement 13 of the measures in June; the Supervisory Board is responsible for the supervision of their implementation.
Approximately 40% of VšZP’s losses (and similarly of other insurance companies) stem from errors on the budgeting side. When the MoH switched to programme-based expenditure budgeting in 2022/2023, it began dictating minimum spending amounts to all insurers by care group. However, the MoH does not budget revenues in this detailed way. As a result, VšZP’s revenues have been underestimated by approximately EUR 93.5 million when compared to the way in which the minimum expenditure was set by Decree 100/2023 in March 2023.
Another approximately 40% is accounting shifts. The programme budget is made so that on a cash basis, the revenues and expenditures are balances. However, insurance companies are public limited companies with double-entry accounting and naturally there is a shift between the cash and accounting view. This became significant in 2023, as several amendments to the law shifted the timing of payments for some items that were not covered by revenue in the budget. On the accounting side, though, these are ledgered as a cost. For VšZP, this represents approximately EUR 90 million of the expected loss.
The remainder (roughly 20% of expected losses), is health care expenditures, which are higher than the MoH budgeted for in Programme Decree No. 100/2023. The primary driver of the increase is pharmaceuticals, whose growth is approximately four times the budgeted plan. This is due to the amendment to the Medicines Act in June 2022 (see related Policy Analysis on pharmaceutical reimbursement legislation and reforming categorization processes). Many more medicines are coming onto the market and entering the categorisation process than in previous years, that is, being added to the positive lists of reimbursed medicines, and the impact of this is approximately EUR 50–60 million higher than budgeted for VšZP. Thus, while medicines were expected to grow by around 2% in 2023, the increase is currently estimated at 8% or more. In addition to medicines, spending on laboratory diagnostics or inpatient care is growing faster, which is, for example, due to the opening of two new hospitals in Slovakia (Bory Hospital and Cardiocentrum Šaca in Košice).
As the Ministry of Finance does not have sufficient resources to cover VšZP’s losses in full and savings have to be found on the VšZP side, the recovery plan for VšZP introduced in June 2023 and its 13 measures aim to save approximately EUR 52 million by the end of the year.
The measures are divided into two parts – administrative savings (EUR 11 million) on operations and savings to eliminate above-standard increases on care (EUR 41 million). The latter is primarily aimed at reducing expenditure on laboratory diagnostics and boosting allocative efficiency of company resources. As a part of the effort of the MoH to realise these savings, the CEO of VšZP, R. Strapko was dismissed and interim management is currently in charge (TASR, 2023).
Even if savings are achieved, VšZP will need a top-up of EUR 165 million (that is, 3.8% of the VšZP’s annual revenue) to avoid receivership status next year and additional liquidity problems as early as December 2023.
The Ministry of Finance has not yet promised whether it will proceed with the refinancing, as they are waiting to see if VšZP can enact savings measures this year before guaranteeing additional funding. In May, VšZP already experienced cash problems in paying its liabilities, which is why the MoH proceeded to advance payments. Thus, cash is not currently an issue for the payment of invoices, but only until December 2023, when this payment will be cleared. The MoH therefore has until the end of the year to resolve the situation, but with national elections on 30 September 2023, there is no guarantee that any top-up funding will be able to materialise in time to prevent VšZP’s dire liquidity issues.
References
HCSA (2023). Straty zdravotných poisťovní nemajú rovnakú príčinu (Health insurers’ losses do not have the same cause). Úrad pre dohlad nad zdravotnou starostlivosťou (Healthcare surveillance authority). Available from: https://www.udzs-sk.sk/blog/2023/05/09/straty-zdravotnych-poistovni-nemaju-rovnaku-pricinu
TASR (2023) Minister Palkovič odvolal z funkcie šéfa Všeobecnej zdravotnej poisťovne (Minister Palkovič dismissed the head of the General Health Insurance Company). SME. Available from: https://domov.sme.sk/c/23192316/strapko-vseobecna-zdravotna-poistovna-vszp-odvolanie.html
2.8.2. Regulation and governance of providers
Regulating provided care (also for quality aspects) focuses on three components: structure, processes and results. The first component, regulation of structure, is most clearly defined. The Ministry of Health sets minimum criteria for material and technical equipment as well as qualifications and personal criteria. The following conditions need to be met by a health care facility to provide health care in Slovakia: (1) a permit to operate the facility and (2) a licence from the relevant professional chamber for the various professionals working in the facility. Both can be requested if material, technical, staff and qualification requirements are met.
The permits for almost all in- and outpatient facilities are issued by the relevant SGR. Disputes are settled by the Ministry of Health. The Ministry of Health also issues permits for providers of emergency medical services, specialized hospitals, facilities for biomedical research, tissue units, biological banks and reference laboratories. Providers willing to act in several SGRs also fall under the competences of the Ministry of Health.
Permits are granted for an indefinite period of time, during which the provider is obliged to observe the legal conditions of their entry to the market. The facilities of emergency medical services are an exception; they can only obtain a permit from the Ministry of Health for a period of six years based on a tender. After winning a tender, financing from HICs and an identified operating territory are secured.
Independent health care professionals who do not operate in any health care facility but function as entrepreneurs may provide health care services based only on their licence to perform in an independent medical practice.
Almost all GPs and the vast majority of specialized physicians provide health care services in private medical practices. The state is the owner of the largest (mostly university and teaching) hospitals, almost all of which are contributory organizations. Five state-owned health care facilities were transformed into joint stock-companies by the 2004 health reform.
Irrespective of their legal form, all providers need to compete for contracts with HICs based on quality criteria and prices. By delegating the competences to establish a network of providers from the Ministry of Health to HICs, selective contracting was enabled in the Slovak health system. To guarantee accessibility of providers, a minimum network requirement is set by the government to influence capacity planning. This network is based on calculations of the minimum number of physicians’ posts in outpatient care and a minimum number of hospital beds for each of the eight SGRs. Minimum capacities are calculated per capita, but they do not consider the specific health care needs of the population and the effective use of resources.
HICs are responsible for maintaining the minimum network. Both selective contracting and market demands motivate health care providers to adapt to changes in demand. The government can adapt the minimum network requirement and by doing so direct the planning of the health sector. In 2016 a total of 36 state hospitals, specialized institutions and medical institutions are part of this legally set minimum network.
The Ministry of Health also regulates natural healing spas, natural healing resources and natural mineral waters through the State Balneal Committee.
The second quality component, regulation of processes, is very general. The Ministry of Health requires providers to have written documentation concerning their quality system, in order to reduce shortcomings in health care provision. However, the Ministry of Health has so far not enforced this requirement. It only issues guidelines, which are neither legally binding nor enforceable. Therefore, health care providers are not required to undergo external monitoring, or to publish their financial results or quality indicators publicly, thus reducing quality systems in health care to a mere formality.
The third quality component, regulation of results, is limited to issuing quality indicators on health care providers, which serve as criteria for selective contracting. Quality indicators are published yearly and are developed by the Ministry of Health in cooperation with professional organizations, HICs and the HCSA. According to the HCSA’s own statement, the data collected by health care providers have low validity, which results in the low credibility of the providers’ ranking.
Suspicions of malpractice are investigated by the HCSA. If malpractice is confirmed, the HCSA can impose sanctions on the health care provider in cooperation with the SGR and the Ministry of Health. In case of a suspected crime, the HCSA files a motion to bring a contested issue before a court for decision. Such incidents are published by the HCSA in case report summaries.
General overview
In March 2025, the Slovak Government approved the most significant reforms to the emergency medical services (EMS) system in over two decades. Although the initial implementation date was set for 1 January 2025, the new legislation will be introduced in phases, and commenced on 15 April 2025. It includes structural changes to ambulance services, the development of a new ambulance network and the introduction of a new professional role.
Structural changes to ambulance services
Several new types of ambulance crews will be deployed. One of the most notable is the hybrid rapid medical assistance (RLP)/rapid medical aid (RZP) model, whereby a physician-staffed RLP unit will operate during daytime hours, and an RZP crew without a physician at night. This measure is designed to optimize the use of physicians, whose availability in the Slovak health system is limited.
Another innovation is the RZP crew with extended-scope specialist paramedics. These paramedics will be authorized to perform advanced medical interventions previously reserved for physicians, with the intention of accelerating care delivery, particularly in remote or underserved areas.
The reform also introduces specialized ambulance types, including:
- Planned transport ambulances for non-emergency inter-hospital transfers and selected low-acuity primary calls, freeing doctors and paramedics for acute cases.
- Mobile paediatric intensive care unit ambulances, operated by tertiary paediatric healthcare facilities, to ensure critically ill children are transported by personnel trained in paediatric emergency medicine.
- Emergency medical assistance ambulances for repatriation (if a patient is abroad and needs transport back to Slovakia) and other non-insurance-covered transport needs, such as medical coverage at social, cultural and sporting events.
Development of a new ambulance network
The EMS network will be redesigned based on a mathematical optimization model that uses historical data on response times, call volumes, call types and geographic distribution of incidents. This model will propose optimal crew deployment to minimise response times and maximize coverage.
As a result, the number of ground ambulance service stations in Slovakia will increase from 321 to 344 from the next tendering period, beginning in Autumn 2025. Additionally, the reform specifies more precise regulations for the location of EMS stations in regional capitals to improve equitable access across urban areas and surrounding municipalities.
A commission within the Ministry of Health will monitor compliance with newly established quality indicators for both EMS providers and emergency dispatch centres. The first set of indicators was published in the Official Gazette in mid-2025, with systematic measurement scheduled to commence in 2026.
Introduction of a New Healthcare Professional Role
The legislation also creates a new category of healthcare worker: the transport assistant. Transport assistants, similar in status to nurses within the EMS system, will be formally registered with the Slovak Chamber of Emergency Medical Technicians. This ensures both professional representation and access to continuous professional development opportunities.
Another key feature of the reform is the planned introduction of a new emergency telephone number, 116117, in January 2026. This number will handle non-urgent medical inquiries, thereby alleviating the workload on the existing emergency number 155, which will continue to be reserved for urgent, life-threatening cases. The aim is to enable EMS teams to concentrate their resources on critical incidents requiring immediate intervention.
References
Fekete, B. (2025) Vláda schválila najväčšiu reformu záchraniek za posledné roky. Čo nás čaká? (The government has approved the biggest reform of the emergency services in recent years. What can we expect?). MEDICINA Trend. Available online from: https://medicina.trend.sk/2025/03/12/vlada-schvalila-najvacsiu-reformu-zachraniek-za-posledne-roky-co-nas-caka
Jeseňák, Š., Gaston, I. and Majerský, F. (2025) František Majerský & Gaston Ivanov: Najväčšia reforma záchrannej zdravotnej služby za 20 rokov s cenovkou 1,2 miliardy € (František Majerský & Gaston Ivanov: The biggest reform of the emergency medical services in 20 years, with a price tag of €1.2 billion). Ozdravme.sk Available online from: https://www.ozdravme.sk/Dokument/101831/frantisek-majersky-gaston-ivanov-najvacsia-reforma-zachrannej-zdravotnej-sluzby-za-20-rokov.aspx
2.8.3. Registration and planning of human resources
Each health professional is obliged to register in the relevant professional chamber and regularly update their occupational and educational activities. Upon completion of a university education and having been issued a licence, graduated physicians are authorized to practise as physicians. Health care professionals can be providers themselves (as entrepreneurs) or employees of a provider. As providers they need both a permit and a licence, but as employees they need only a registration from the professional chamber. A licence is also issued by the professional chamber and provides proof of qualification (education and years of practice).
In order to operate an outpatient practice, a physician must submit their licence to the chief physician of the relevant SGR, together with an application for a permit to operate an outpatient practice. Upon fulfilling certain requirements for qualification and medical equipment (technical and personnel criteria established by law), a physician is authorized to run their own practice. There is no system of recertification of licences in the Slovak health system. Furthermore, there is no mechanism for regulating the number of health workers in each category and specialization according to the population’s needs.
A lack of regulation is evident in long-term human resource planning. Decisions concerning the numbers of students and graduates at medical faculties are made by the university, funded by the educational sector, and are not linked to health sector needs. The EU accession has strengthened the mobility of health professionals and has resulted in shortages in specialists in certain areas. Expanding emergency medical services by requiring them to employ anaesthesiologists has led to a decrease in the number of hospital-based anaesthesiologists. The rigid territorial planning of GPs until 2004, which made the profession unattractive for new entrants, combined with the ageing of the workforce, has led to significant shortages in the sector (see section 4.2).
Residency programme
The Strategic Framework for Health 2014–2030 tackles the planning of human resources in Slovakia. Firstly, it addresses the ageing workforce, and should reduce the average age of GPs from current 54 to 40 years by 2030. Key to achieving this goal is a newly established residency programme, which aims to (1) reduce the average age of GPs and paediatricians, (2) improve education in general medicine for adults, children and adolescents, and (3) improve the quality and accessibility of health care in primary care.
The pilot project began in the school year 2014/2015, and graduates of medical schools can apply immediately after graduation. Other graduates of medical faculties must meet these conditions: age up to 36 years and the non-inclusion of any specialized study, or already enrolled for the specialized study, which is scheduled to terminate at the earliest at the end of October 2015. The programme should also raise general awareness of quality and gatekeeping in primary care and improve accessibility of health care.
Hand in hand with decreasing the age of the workforce, performance indicators are also to be improved. Firstly, the gatekeeping role of GPs is to be strengthened, so that the number of patients sent to specialists or hospitals decreases from the current 80% to 30% in 2030. Secondly, consultations per capita are to decrease from 11.3 in 2014 to 6.4 in 2030 (Strategic Framework for Health 2014–2030) (see section 6.2).
2.8.4. Regulation and governance of pharmaceuticals
Before entering the market in Slovakia, pharmaceuticals must have an authorization from the European Medicines Agency (EMA), or the national-level State Institute for Drug Control (SIDC). The SIDC closely monitors the safety of drugs in Slovakia and is the national competent body responsible for pharmacovigilance. Monitoring includes reporting of adverse reactions, requiring reports from pharmaceutical companies as well as pharmaceutical quality. Reports on adverse effects are submitted to the Centre of Adverse Effects Follow Up in the SIDC. The prescribing physician is obliged to report any adverse effects. The number of reports peaked in the 1980s and the 1990s with over 2000 reports annually. In the late 1990s the number of reports fell below 500 per year but has been well above that number in the early 2000s. In 2015 there were 1171 reports (SIDC, 2016).
Market authorization holders are also obliged to report adverse effects of drugs. Each market authorization holder appoints a person responsible for pharmacovigilance. In addition to physicians, the reporting of adverse effects applies to pharmacists and nurses as well as patients. The SIDC has the right to suspend distribution of a pharmaceutical or withdraw a pharmaceutical from the market, and in more serious cases can suspend the registration for 90 days or terminate the registration.
General public advertisement is permitted for drugs free of dazing and psychotropic effects, and OTC drugs not covered by health insurance. Advertisements aimed at physicians and pharmacists have no such limitations. Vaccination campaigns, with the permission of the Ministry of Health, are another exception. The content of general public advertisement may not give the impression that medical examination is not necessary or that pharmaceutical effects are guaranteed. The description of a diagnosis should not mislead patients, and result in self-diagnostics; it should avoid exuberant, ugly and misleading expressions. The advertisement should not compare a drug to food, cosmetic products or consumer goods. It must be clear that the information is an advertisement, containing clear information on proper use. The SIDC is in charge of advertising standards.
Based on European legislation, as well as the recommendation of the EMA to improve the knowledge of patients, the SIDC has created a patient portal on the website www.sukl.sk. This portal publishes a list of patient organizations. However, it has not been updated since 2007, which may reflect a rather formal approach to the patients’ agenda.
Additionally, the Dôvera HIC started its own e-health project, “Safe drugs”, for its 1.4 million insured individuals. This is an online service which links doctors, patients, pharmacists and the company itself more directly. The main goal of the project is to increase patient safety and decrease the risk of polypharmacy for complex patients.
Reimbursement decision
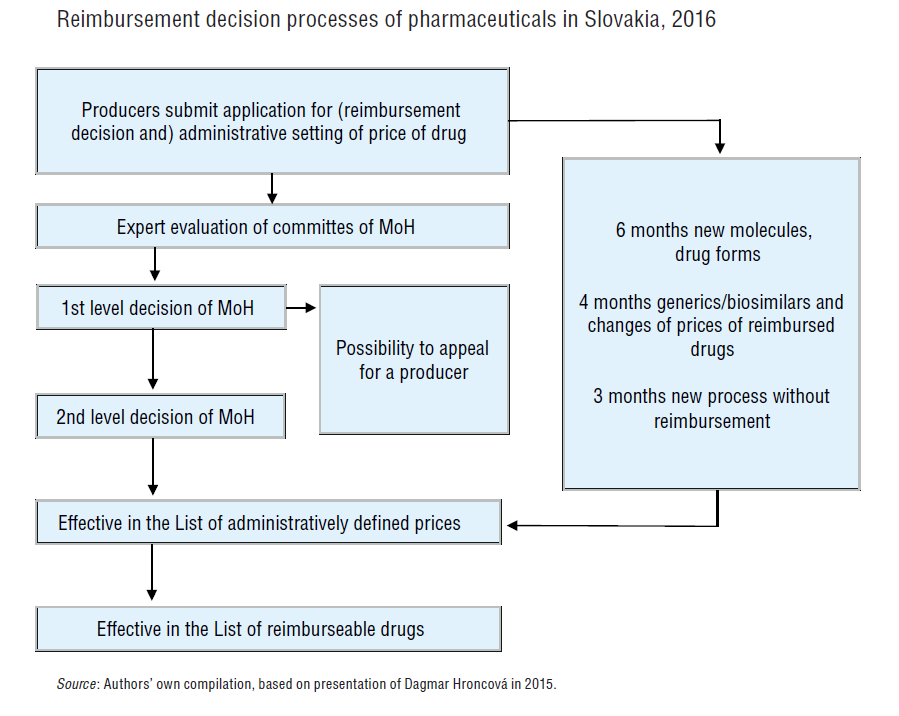
The decision as to whether a pharmaceutical will be covered by SHI
is the competence of the Ministry of Health and its reimbursement
committee. The decision is made after an assessment of the
pharmaceutical (see Fig2.4). A similar process is used for medical
devices and dietary products. The Ministry of Health centrally regulates
the scope of health care services provided by health insurance by
defining the list of fully, partially or non-reimbursed drugs, medical
devices and dietary products, and also by defining the list of priority
and non-priority diseases, as well as by definition of co-payments and
user fees.
Fig2.4
First, the marketing authorization holder must submit comparative
data on the pharmaceutical, including effectiveness, safety and
pharmacoeconomic data. In line with recommendations from the Ministry of
Health, the pharmaceutical is assessed using cost-minimization,
cost-effectiveness and cost–utility analysis. The discount rate for
benefits and costs was set at 5%. The recommended threshold of a
cost-effective new technology was set at 24x the average monthly wage
from two previous years per unit of health state improvement (€20 592 in
2016), and thus pharmaceuticals with lower costs per QALY
are considered cost-effective. In contrast, pharmaceuticals that exceed
35x of the average monthly wage from two previous years per unit of
health state improvement (€30 030/QALY in 2016) are not considered cost-effective. Pharmaceuticals whose QALY range lies between €20 591 and €30 030 per QALY in 2016 will undergo further evaluation.
Second, each pharmaceutical is evaluated according to its anatomic and therapeutic classification by one of the 22 specialist working groups. The working groups evaluate the effectiveness, safety and importance of each pharmaceutical. One working group evaluates the pharmacoeconomic properties of the pharmaceutical. The results produced by the specialist working groups serve as the context for the decisions of the Reimbursement Committee for Medicinal Products. The Committee has 11 members, of whom three are representatives of the Ministry of Health, five are representatives of the HICs and three are representatives of the professional public.
Lastly, the Reimbursement Committee puts forward proposals for inclusion, non-inclusion, exclusion or change in the status in the benefits package, along with proposals for reimbursement level, co-payment and conditions for reimbursement. The results of their decisions are published on the webpage of the Ministry of Health after every meeting of the Reimbursement Committee. The applicant receives written information on the results of the reimbursement decision, and may appeal the decision.
The process of reimbursement decision-making for drugs is updated and published once a month. Requests for inclusion in the official price list may be submitted at any time. Price changes and the inclusion of medicinal products shall be published each month, according to the actual timetable of the entire assessment process.
The frequency of revising the reimbursements is four times a year. These revisions become enforceable always on the first day of the calendar quarter (1 January, 1 April, 1 July and 1 October).
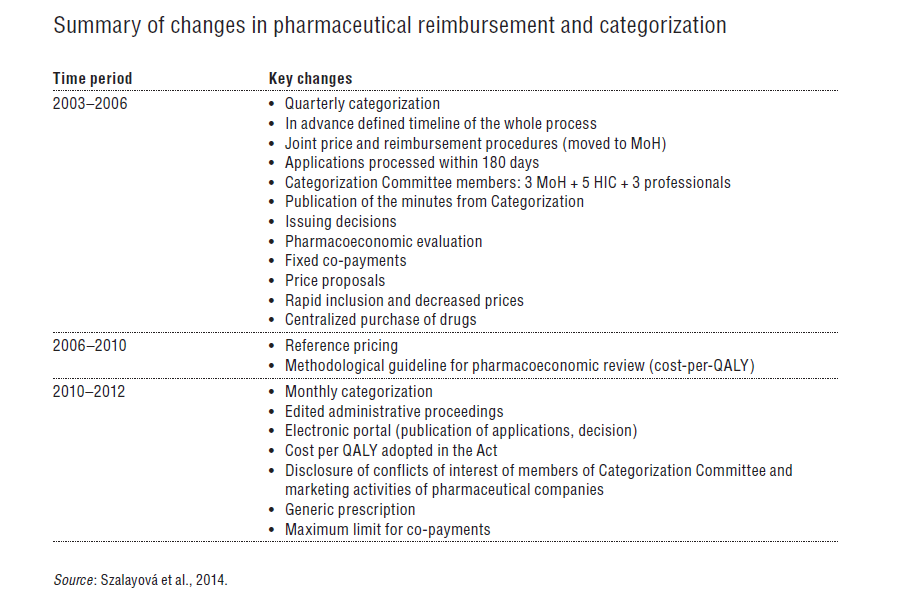
For the summary of changes in pharmaceutical reimbursement and categorization, see Table2.4.
Table 2.4
Pricing decision
Slovakia operates a reference pricing system for pharmaceuticals. SHI
reimbursement is set as the maximum price for a standard daily dose in
the reference group of the pharmaceuticals. The definition of a given
reference group is very narrow. All pharmaceuticals included in the
reference group contain the same active substance and are administered
uniformly. In certain cases the Reimbursement Committee may decide to
form a separate reference group for pharmaceuticals with different
administering form and a different amount of active substance per dose.
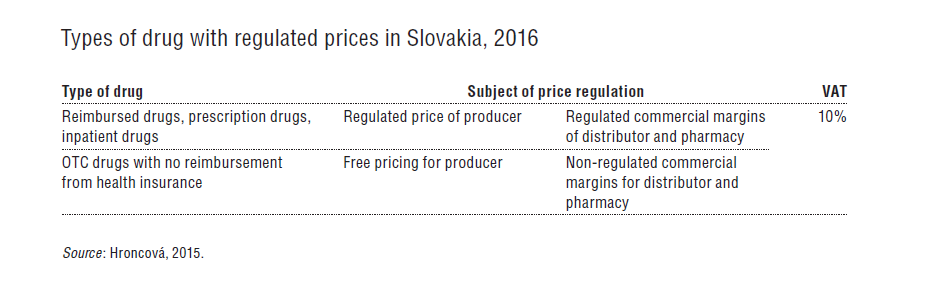
The prices of pharmaceuticals covered by SHI
are regulated, both in the ambulatory and inpatient sectors. After
obtaining an authorization to enter the market, the ex-factory price of
the pharmaceutical is determined by the Ministry of Health through
external reference pricing. The ex-factory price may not exceed the
average of the three lowest prices of the same pharmaceutical sold in
all 28 EU countries. The prices of OTC pharmaceuticals and prescription pharmaceuticals not covered by health insurance have been deregulated (Table2.3).
Table2.3
A
degressive margin for pharmaceuticals and dietary foods was first
introduced in Slovakia in 2004. Initially, the margins were set as a
fixed percentage from the pharmaceutical price (11% for the distributor
and 21% for the pharmacy). In 2004 a lower margin (10%) was established
(4% for the distributor and 6% for the pharmacy) for so-called
financially demanding pharmaceuticals, i.e. certain high-priced
pharmaceuticals that put pressure on the budget. However, exactly what
constituted a financially demanding pharmaceutical was never precisely
defined. The decision to include a pharmaceutical in this category was
made by the Reimbursement Committee during the reimbursement decision.
Since 2008, however, a more elaborate degressive system has been in
place, which sets margins separately for distributors and pharmacies
based on the ex-factory price (Table2.5).
Table2.5

VAT on pharmaceuticals has changed several times since 1999. Until 1999 it was 6%, after which it rose to 10% in the period 2000–2002. In 2003 VAT increased to 14% and a flat rate of 19% VAT was introduced in 2004. On 1 January 2007 the new government reduced the VAT on pharmaceuticals to 10%. VAT on the pharmacy margin was introduced on 1 January 2004.
Generic substitution
Regulation in 2011 (Act no. 362/2011) amended the legal framework of 2005 on generic substitution. The change obliged doctors to prescribe the effective substance of a medicine. Furthermore, pharmacists were obliged to inform patients about cheaper alternatives (generics) when filling a prescription. If the physician did not provide any reason not to use the generic substitute, the patient may choose the less expensive option under the supervision and advice of a pharmacist.
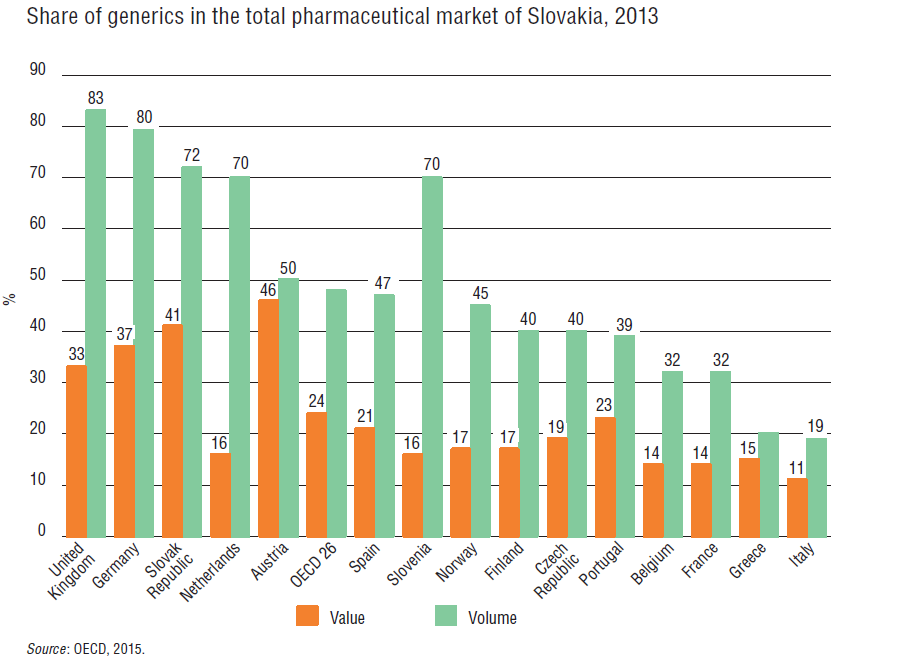
Out of 4415 medicines reimbursed under health insurance during the first half of 2016, 2573 (i.e. 58%) were registered as generics. According to the OECD (2015), 72% of all medicines that were partially or fully reimbursed in 2013 were generics, which accounted for roughly 41% of total pharmaceutical sales in the country. These values are some of the highest among OECD member countries (see Fig2.5).
Fig2.5
2.8.5. Regulation of medical devices and aids
Medical devices and aids are assessed through a similar categorization process as described for pharmaceuticals. This includes the application by the marketing authorization holder of the medical device, evaluations by working groups and a reimbursement proposal prepared by the Reimbursement Committee.
The Ministry of Health acts as regulator, and defines the administratively defined price at which the medical device manufacturer or the importer is allowed to enter the Slovak market. This price is based on the reference pricing principle and is the average of three lowest prices across the 28 EU countries. The Ministry of Health started the process of price referencing for 586 medical devices in January 2016 and implementation was expected in July 2016. According to preliminary reports, a 23.5% reduction in the prices of the 586 medical devices is expected (Černěnko & Haluš, 2015).
The Ministry of Health also sets the maximum margin for the distributor (8.5%) and the retailer (11.5%), which together should not exceed 20%. On average, HICs pay 92% of the price, and the rest is paid by the patient in the form of a co-payment (Černěnko & Haluš, 2015).
2.8.6. Regulation of capital investment
The centrally organized capital budget of the Ministry of Health was largely abolished in 2003 to secure greater transparency in hospital capital modernization. Investment planning was not based on transparent relevant economic or health indicators resulting in unpredictable allocation of funds. Funds are now redistributed to HICs to be included in their payments to providers and cover fully for capital investments. Thus, in theory capital renovation of hospital infrastructure has been financed by the health insurance funds through reimbursement of hospital services.
Providers, however, do not see these revenues as sufficient and often invest additional money into their health facilities and usually bear the investment costs in these hospitals and outpatient centres. The Ministry of Health provides only occasional capital grants, the average value of which is up to €10 million per year. Planning and coordination of resource utilization from the EU structural funds to this day suffer from the same problem. From 2004 onwards, the vast majority of funds for capital investment were allocated to HICs so that they could include amortization in their payments to providers. A programme called “Operation Programme Healthcare (“Operačný Program Zdravotníctvo”) was launched for the period of 2007–2015 to tackle investment gaps in health service provision. The programme, worth €193 million for updating hospital infrastructure and €34 million co-financing from other national sources, only marginally contributed to urgently needed capital (KPMG, 2013). A new Operation Programme for 2014–2020, called the Integrated Regional Operation Programme, which has a budget of €300 million for the capital demands of in- and outpatient providers of care, may have a similarly small impact.
The technical infrastructure of hospitals in Slovakia is often outdated. According to a comprehensive Ministry of Health investigation from 2004, Slovak state hospitals had an average age of 34.5 years. Since then, only one new hospital has been built (St Michael’s Hospital, built by the Ministry of Interior for €50 million). An update by the Ministry of Health had seen a further increase of the average age to 42 years in 2013 (MoH, 2013a). A study by HPI confirmed an insufficient capital formation in Slovak health care (Pažitný et al., 2014). Slovak capital formation in health care was found to be only 59.3% of that of the Czech Republic and 30.8% of that of Austria. Estimates of investments needed to converge with EU15 averages range from €3.9 billion by the Ministry of Health (MoH, 2013a) up to €8.3 billion, in the worst case scenario, by HPI (Pažitný et al., 2014).
It was also discovered that hospitals in Slovakia do not reach international standards in terms of their built-up areas. The majority of hospitals occupy large areas of land with numerous buildings scattered around the area. General hospitals have an average of 30 buildings per hospital; some hospitals have up to 81 buildings.