-
15 August 2025 | Policy Analysis
Out-of-pocket payments in Slovakia reach EUR 1.7 billion with very low transparency and high legal uncertainty -
08 October 2018 | Country Update
Change in methodology for capturing OOP payments in 2017
3.4. Out of pocket payments
Private expenditure comprised approximately
25% of total health expenditure (€1460 million, according to national
accounts) in 2014. It is primarily composed of private households’
cost-sharing (90% of total expenses are OOP payments). OOP payments
in Slovakia mainly consist of (1) co-payments for prescribed
pharmaceuticals and medical durables; (2) user fees for various health
services, stomatology care and spa treatment; (3) direct payments for OTC pharmaceuticals, vision products and dietetic food; (4) above-standard care, preferential treatment and care not covered by SHI;
and (5) a few standard fees – for 24/7 first aid medical services
(€1.99), ambulance transport (€0.07/km), for prescriptions (€0.17), for
accompanying people during a hospital stay (€3.32), as well as for food
and accommodation in spas (€1.66 or more per day). See Table3.8 for a
comprehensive overview.
Table3.8
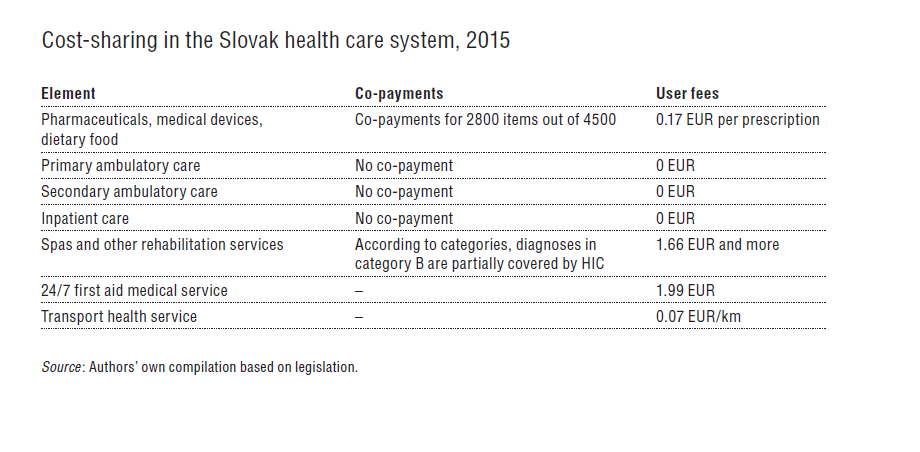
The
Slovak system supports underprivileged residents in the form of maximum
limits for co-payments for prescribed pharmaceuticals, waiving of
ambulance transport fees for chronically ill, and a wide range of
medical devices with individually reduced cost-sharing. Moreover, around
one-third of all reimbursed medicines have no co-payment.
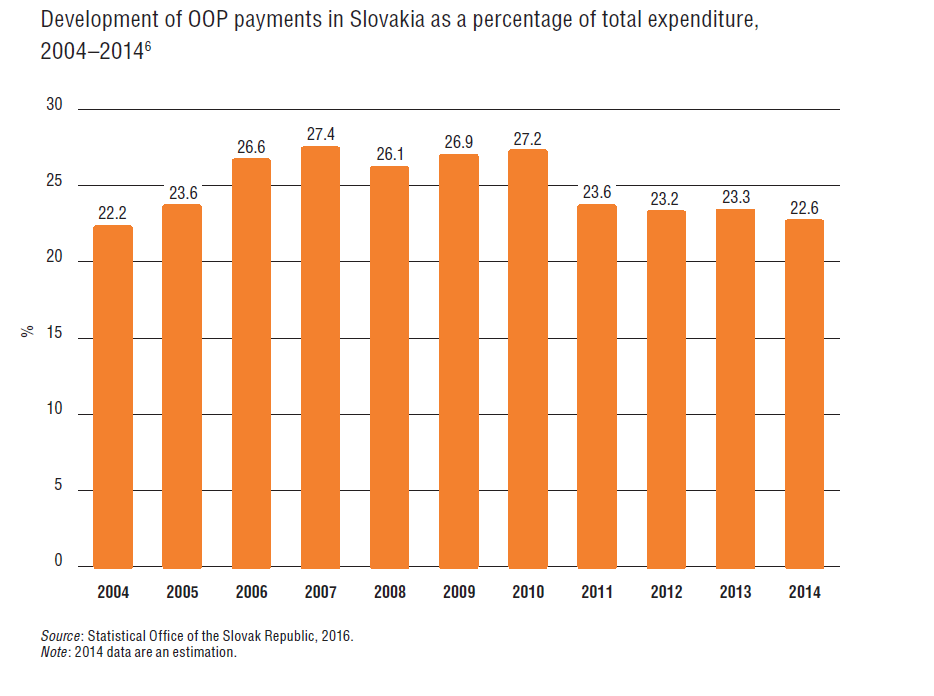
In 2014 Slovakia had a share of 22.6% of total health expenditure paid out of pocket. As illustrated by Fig3.9, the level of OOP payments grew from 2004 to 2007. This was the result of a tax policy change (an increase of VAT on
pharmaceuticals from 10% to 19% over 2003–2005) and the introduction of
a variety of co-payments. Other reasons for increasing OOP expenditure were higher spending on OTC drugs
and new products offered in pharmacies, increased use of private
providers, and an increase of different fees for non-standard health
care services.
Fig3.9
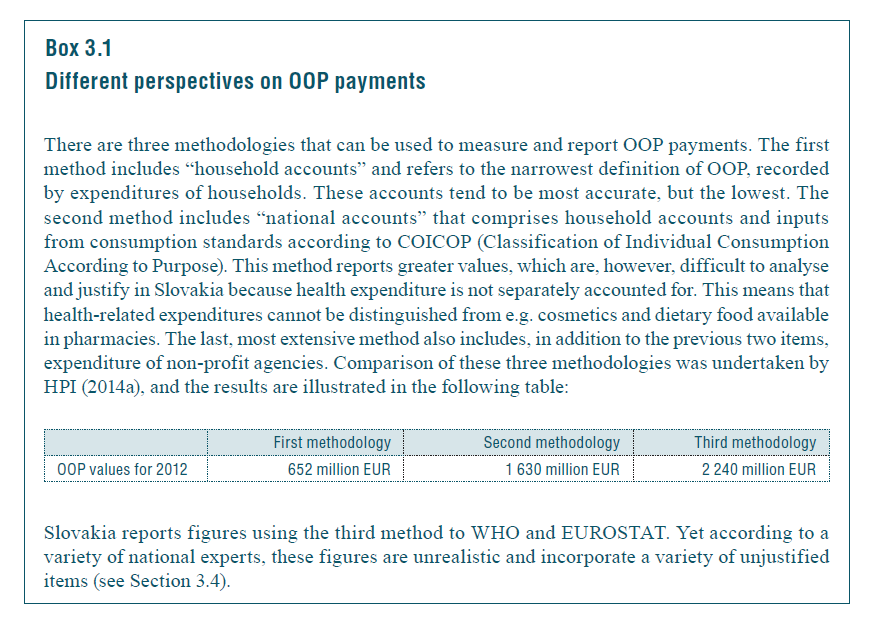
It is important to note that the provided OOP expenditure is based on estimations, as indicated in Box3.1. The methodology of the Statistical Office of the Slovak Republic for calculating OOP expenditure also includes, besides co-payments for prescribed drugs, items that are sold in pharmacies but are only marginally health-related, e.g. decorative cosmetics. However, due to the technical limitations of reporting receipts to the Ministry of Finance, these items cannot be split from medicine expenditure. This may overestimate OOP expenditure in Slovakia (see Box3.1 for more information). On the other hand, OOP expenditure may be underreported given the weak reporting legislation for non-standard services by ambulatory and hospital visits, which include for example different administrative fees, booking of the exact time of appointment, and specialists’ examinations without referral from GPs. However, the providers are not obliged to report the entire sums of these payments.
Box 3.1
Additionally, the Statistical Office overhauled the methodology of reporting private expenditure in 2010. This caused a significant reduction in private expenditure and a consequent decrease in the proportion of private expenditure. However, the office did recalculations only from 2011 onwards.
In 2023, total out-of-pocket spending (OOP) in Slovakia reached EUR 1.7 billion EUR, and just over 18% of current heealth expenditure. At the same time, OOP payments are legally inconsistent, economically inequitable and lack transparency (see Table 1). Analysis of OOP spending reveals several key issues:
Low transparency and information asymmetries
Patients often do not know what exactly they are entitled to, do not understand the differences between a fee and a co-payment, or betweenstandard and above-standard service. Patients are often not informed by providers of these differences. Patients are often not issued receipts in practice, further reducing transparency.
There is also a variation in patients‘ readiness to pay, with some unwilling or unable to do so. Some are unwilling based on the principle of free healthcare at the point of service, while others, especially in poor regions, simply cannot afford to pay. There are also those willing to pay OOP, giving them priority and more adequate consultation times, scheduled appointments, and an individual, higher-quality approach.
Gaps in regulation, inconsistent approaches and legal uncertainties
There legal uncertainty surrounding the interpretation regarding providers’ ability to charge fees. After approximately 600 amendments since their adoption, laws 576, 577, and 578 of 2004 (core laws underpinning the major 2004 health system reform) create contradictory motivations for providers.
As stated by providers, a main reason for rising fees is due to insufficient reimbursements from insurers, leading them to seek alternative sources of funding to try to maintain levels of care quality. Other given reasons include rising staff wages (especially in public hospitals), the introduction of a transaction tax, general inflation across the economy and increasing energy costs.
Beginning in 2006, legal restrictions against direct payments were introduced. However, in practice, a chaotic “fee jungle” has emerged, with exploitation of numerous legal loopholes. This is also reflected in the varying levels of patient information (differing communication and price list publication methods), reducing predictability of patient costs.
Furthermore, the absence of regulation has led to variability in the fees charged among providers even within the same specialty. Price lists reveal regional differences: the highest charges are in Bratislava (sometimes multiple times higher), while in smaller towns or rural areas, fees tend to be lower or nonexistent.
Finally, an outdated performance catalogue does not reflect technological progress nor current market prices for materials. Notably, the catalogue was originally intended as a tool for introducing innovation (for example, telemedicine, AI, interventional radiology), not solely as a pricing mechanism.
Table 1: Legislative anchoring of direct payments and their relationship to public health insurance
| Occurrence of direct payment | Purpose of direct payment | Legislative basis |
| Before provision | Patient management | Act 576/2004 allows for charging for services beyond standard public coverage. However, annual care program services may be covert payments for services that should be free (Act 577/2004 prohibits fees for appointment scheduling, priority treatment, and administrative tasks). There are often collected by intermediaries (not the providers themselves); the healthcare service itself is reimbursed by an insurer. |
| Reservation portal | Legal loophole: current laws prohibit providers from charging for scheduled appointments.
Exploited by third-party private companies offering booking systems independent from the state and healthcare providers. | |
| During provision | Fees for services related to care provision. | Regulated in §38 of Act 577/2004 in which Slovakia’s Constitutional Court confirmed that such charges are constitutional. |
| Co-payments for medicines, medical aids, durables and materials and dietetic food | Yes, most clearly regulated type.
Defined entitlements and transparent costs for both insurer and patient. | |
| Direct payments to non- contracted providers | Governed by commercial code | |
| Price list fees | Partially regulated: not clearly defined in Act 577/2004 and indirectly referenced in Act 578/2004 requiring a public price list submitted to regional authorities Legally questionable in some cases (e.g., booking fees, prescription printing, spa referral), and often charged due to outdated reimbursement catalogue or lack of coverage in practice. | |
| After provision | Second opinion | While not explicitly defined in law or reimbursement systems, this is usually billed to insurers as a regular consultation or repeat exam. Sometimes charged separately, especially for advisory consultations. |
Source: Pažitný et al. 2025
An examination of the health financing in Slovakia’s specialized outpatient care sector reveals a fragmented landscape of patient cost sharing and direct payments. Legal ambiguity, regulatory inconsistency and increasing financial burdens for patients create significant challenges for fairness, transparency and sustainability. Key areas for reform, not only to simplify rules and protect patients but also to restore trust and ensure long-term sustainability of the health system could include the following:
- Legalizing all types of co-payments – being clearly defined in Act 577/2004 and making any fees and co-payments transparent and understandable.
- Extend informed consent – informing patients of the amount in advance and for what service they are paying.
- Issue receipts for every healthcare service provided – an invoice showing exactly what services were provided, and what is paid by the insurer and what by the patient.
- Health insurers must be involved – informing insurers about any patient charges collected by providers.
- Introduce effective financial protection via co-payment limits – with eligible populations clearly defined.
- Shift the control of patient charges to regional authorities – via legislation to allow them to define scope and amount of allowed fees locally.
- Creation of a reimbursement mechanism to help cover some administrative costs – with the involvement of the Slovak Social Insurance Agency, health insurers and providers
References
Pažitný, Kandilaki, Macko-Forgáčová, Löffler, Zajac: Direct Payments in Specialist Outpatient Care in Slovakia, June 2025
Smatana, M. et al. (2025) in press. Slovakia: health system review 2024. Health Systems in Transition
There has been controversy about the underlying methodology to capture OOPs in Slovakia for years and criticism towards the Statistical Office to overstate OOPs. This has been tackled by two consequent corrections: 1) In 2010, the Statistical Office overhauled its methodology and re-calculated OOPs accordingly for 2011 and onwards; 2) In 2017, the Statistical Office corrected for receipts sent to the Ministry of Finance (therefore switching to the “household account” methodology) for 2015 and onwards.
This resulted in a sharp decline of reported OOP payments to international databases like WHO and Eurostat. For instance, according to the old methodology OOP amounted to 1345,5 mil EUR in 2015, whereas the corrected value was by more than 500 mil EUR lower. In 2016, the old methodology resulted in a total of 1607 mil EUR for OOP, whereas the new methodology is capturing only 849 mil EUR as OOP.
Authors
3.4.1. Cost-sharing (user charges)
A variety of policies were adopted to contain the increase in cost-sharing, such as the de facto abolishment[5]
of co-payments for outpatient care and hospital stay or lowering
co-payments for prescribed medicines. Nonetheless, the proportion
remains high, since most OTC
drugs are not regulated and a small number of services (e.g. dental
care or ophthalmology care) remain cost-shared, along with some anchored
fees for emergency services, receipt processing, ambulance
transportation and spa treatment. Table3.8 gives an overview on current
cost-sharing in Slovakia.
Table3.8
- 5. Co-payments have never been abolished in practice, but their value was set in legislation to zero. ↰
3.4.2. Direct payments
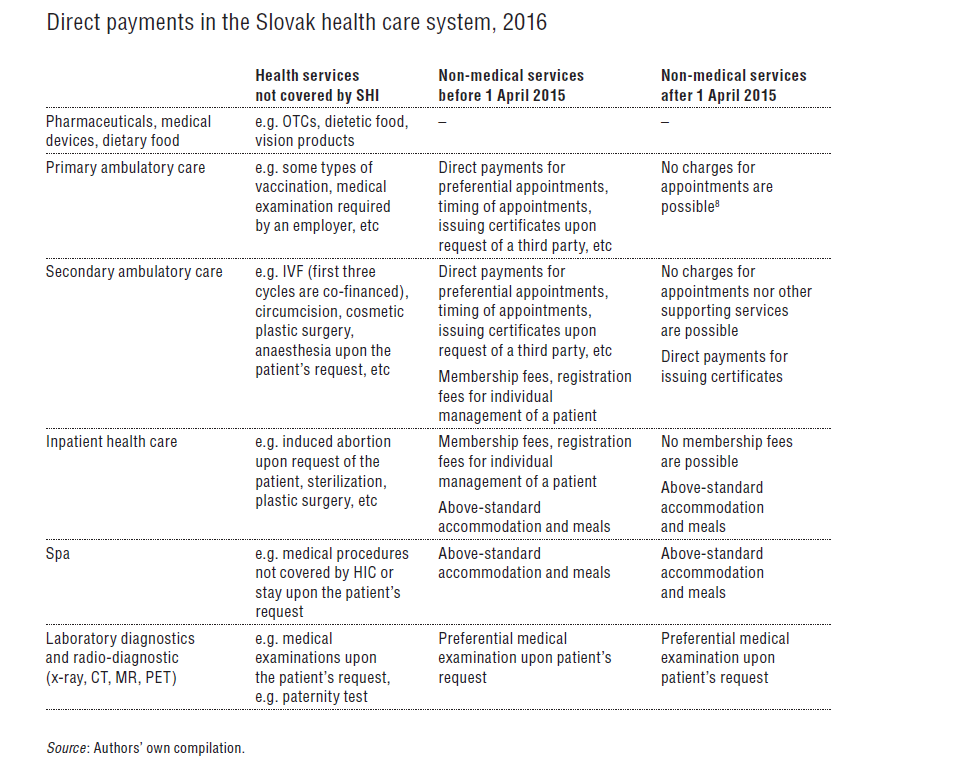
Direct payments in the Slovak health sector comprise mainly payments for OTC pharmaceuticals and dietetic food and care not covered by SHI.
In 2015 the Ministry of Health introduced new legislation restraining possibilities for providers to charge for health care and health-related services. This was a response to the fact that although cost-sharing for medical services was regulated gradually, the providers were free to charge fees related to care (e.g. a payment for air conditioning in the waiting room, a payment for administrative tasks, payment for printed documents, etc.). These payments were identified as one of the key drivers of increasing OOP expenditure but were virtually outside legislative control. The new legislation since 2015 defined which nonmedical services can be charged for and enforced greater control by the SGRs. A brief overview of some of these direct payments is given in Table3.9. However, the legislation has been heavily criticized by health professionals and the public, as well as the media, and an amendment is planned during 2016.
Table3.9
3.4.3. Informal payments
According to a survey by Mužík & Szalayová (2013b), 71.4% of respondents (843 out of 1181 respondents) reported making an informal payment in the form of cash or presents. More up-to-date research by Transparency International did not confirm this high percentage, but concluded that almost 27% of respondents made informal payments. The total value of such payments is virtually impossible to estimate (Transparency International Slovakia, 2015).