-
27 July 2023 | Policy Analysis
Amendments to Slovakia’s pharmaceutical reimbursement legislation to combat growing challenges -
30 June 2023 | Policy Analysis
Financial losses at the state-owned insurer (VšZP) and the corresponding recovery plan -
04 June 2018 | Policy Analysis
Increasing efficiency in the Slovak health system: the Value for money project
7.5. Health system efficiency
In recent years, the Slovak health system has faced several problems with regard to pharmaceuticals, creating a growing list of challenges for policymakers. For example. Slovakia has a high overall consumption level of medicines in comparison to other OECD countries, but research shows low levels of generic and biosimilar medicine usage [1].
There is also a general lack of availability of innovative medicines, and managed entry agreements (MEAs) for new medicines on the Slovak market saw only seven new contracts between 2018 and 2021. In the field of oncology, only 20% of indications with confirmed effectiveness out of 135 were reimbursed in 2021 and only one oncology innovative medicine was categorized (that is, was put on positive medicine lists) that same year [2]. As such, expenditure for the reimbursement of medicines through the exception regime (including orphan drugs and those such as Cisplatina and Dakarbazín that left the market, in addition to innovative medicines that are mainly for oncology patients) is now worth over EUR 50 million annually, as many critical medicines were not categorized, with prescribing physicians resorting to sending reimbursement requests directly to the health insurance companies (HICs) [3]. Overall, these problems have contributed to a lack of transparency and predictability of the environment [3] as well as the decreasing bargaining power of the state, and there has been a gradual departure of multinational companies from the Slovak market [2].
In an effort to address these issues, a new amendment to Act No. 363/2011 Coll. on the scope and conditions of payments for medicines, medical devices, and dietetic foods from public health insurance and on amendments to certain acts was approved in June 2022 [4]. The key changes include the following:
- Changes in the categorization process, including the introduction of consultations before proceeding and simplified MEAs, which alone brought 57 new medicines (69 new indications) onto the market in 2022; the Ministry of Health is now responsible for closing MEAs, which previously was done by the HICs and involved negotiations with all three.
- Transparent rules for decision making under the exception regime and upper limit on the volume of funds (3.9% of the allocated funds for HICs – postponed via legislation to 2024 after HICs nearly hit this upper limit (roughly EUR 60 million) in the first few months of 2023 alone).
- Adjustments to the QALY threshold that is now based on GDP per capita from two years prior. For regular medicines, 3 times GDP per capita (for 0.33–1 QALY gained) or 2 times GDP per capita (for 0–0.33 QALY gained) is applied; medicines for a rare disease or an innovative treatment have higher thresholds of up to 10x GDP per capita.
- Requiring the three HICs to make the list of approved medicines through the exception regime available online.
- New procedures for determining, changing and cancelling reimbursement groups, as well as changes in the revision of reimbursements, referencing or entry of generic and biologically similar drugs.
Authors
References
[1] Tesar T., Golias P, Masarykova L., Kawalec P., Inotai A. (2023) The Impact of Reimbursement Practices on the Pharmaceutical Market for Off-Patent Medicines in Slovakia, In Front Pharmacol. 2021 Dec 13;12:795002. doi: 10.3389/fphar.2021.795002. PMID: 34966285; PMCID: PMC8710743 Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8710743
[2] Babeľa Róbert (2023) Novela zákona 363/2011: kde sme a kam kráčame? Presentation for CEEHPN. Available from: https://static1.squarespace.com/static/63c7dbc6ff4f92106ce2bd6d/t/647f01f44a096110aea9e9d2/1686045191518/6_presentation_oncology_Babela.pdf
[3] Löffler Ľubica, Pažitný Peter, Kandilaki Daniela (2022) Lieková politika v širších rozpočtových súvislostiach. Available from: https://healthcareconsulting.sk/sites/default/files/liekova_politika_v_sirsich_rozpoctovych_suvislostiach.pdf
[4] Ministry of Health (2022) Parlament schválil prelomovú liekovú reformu. Available from: https://www.health.gov.sk/Clanok?parlament-zakon-lieky-prelomova-reforma
The “Value for money” project (VfM) aims to identify areas of inefficient spending and resource allocation through in-depth analysis of all key accounts and processes. Any potential savings should be re-invested within the health system to improve technical efficiency. This initiative has been successfully tested in the UK, Netherlands and other countries and is piloted in three sectors, including healthcare expenditure in Slovakia. The project was led by the MoF, the International Monetary Fund and World Bank and was approved by the Slovak government in autumn 2016. The project set targets for three years, up to 2019.
The VfM project set fiscal and qualitative targets for the Slovak MoH that were set as a benchmark for the minister and a condition for receiving capital funds. Fiscal targets were set to achieve savings compared to 2016 of 174 mil. EUR, out of which 143 mil. EUR were from the general health insurance resources (such as through centra procurement of medicines, revision actvities in the GHIC, or implementation of DRGs) and 31 mil. EUR were savings within internal processes of hospitals, as shows table below. Qualitative targets were focused on implementation of a variety of changes in data collection and analysis, e-health, medical consumption and DRGs.
The VfM project is monitored on a quartal basis. According to the final report covering first year, the MoH has been on target in 50% of measures and achieving savings of 79,8 mil. EUR, i.e. 46% of the fiscal target. The greatest improvement was recorded in overconsumption of medicines (18 mil. EUR savings due to an introduction of e-prescription), medical aids (16 mil. EUR savings due to price refencing) and effective procurement of health technologies (14 mil. EUR, due to central procurement and benchmarking).
Authors
References
Implementation unit (2017) Súhrnná implementačná správa [Summary implementation report] [Online] Avalable at: http://www.finance.gov.sk
7.5.1. Allocative efficiency
Allocative efficiency in the health sector is mostly associated with appropriate allocation of resources between the various types of care. Compared to other V4 countries and selected neighbouring countries, the Slovak health care system displays several inefficiencies when allocating resources.
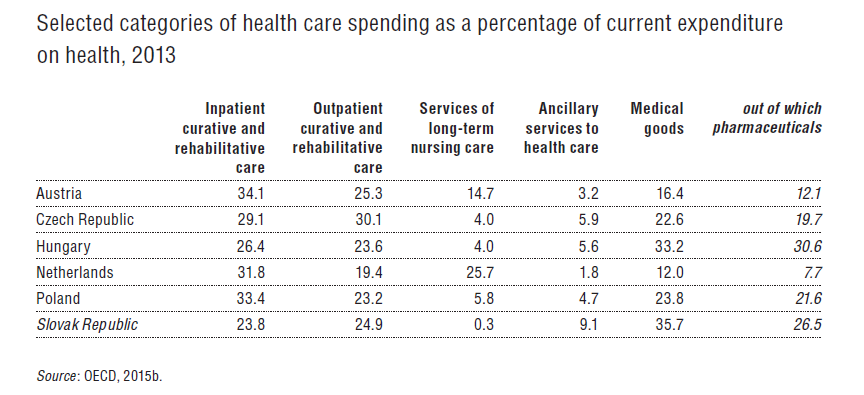
- In 2013 only 23.8% of total resources were spent on inpatient care, which is the lowest in the EU (see Table7.6) and is insufficient for the needs of the Slovak population. There are significant waiting lists for inpatient care (see section 5.4) and capital investments are very low (investment gap) which imply inefficient allocation of resources for inpatient care.
Table7.6
- Slovakia allocated 26.5% for pharmaceutical resources, which is the third highest among the EU28 countries. Recalculating this spending into US$ PPP per capita, Slovakia spent more than half of all the EU28 countries and all other V4 members. Considering Slovakia’s strict referencing system for medicines, over-prescription of medication was the key reason for the inefficiency (Kovalčík & Tunega, 2015) (see section 2.8.4).
- Slovakia has the second highest spending on ancillary services in the EU as a percentage of total health spending. It is driven primarily by laboratory services, transport and emergency services. Duplicate testing caused by the lack of infrastructure to share medical information drives these costs. Spending on transportation services is caused by two factors: (1) the government centrally procures emergency services, and sets and fixes prices for a given period but has never conducted a value-for-money analysis to justify its prices and (2) the rise of secondary transport (see section 5.5).
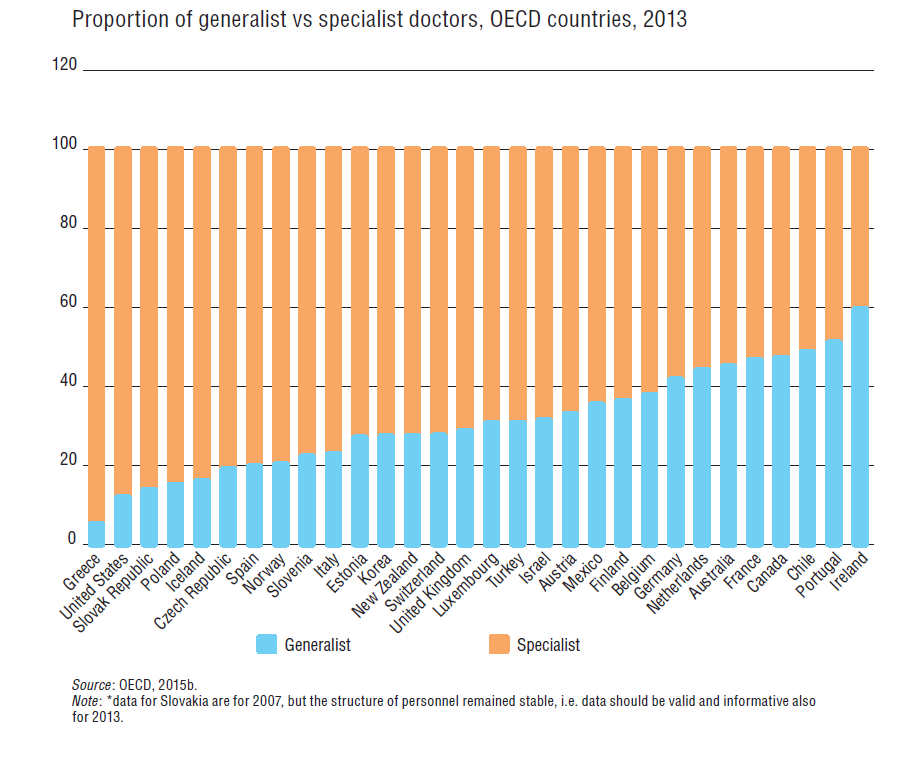
The Slovak health care sector has several other areas that raise questions about its allocative efficiency. Out of 10 doctors, only 1.4 are generalists with the rest being specialists that provide more expensive care. Slovakia has the third lowest proportion of generalist versus specialist doctors among the EU28 countries (see Fig7.9).
Fig 7.9
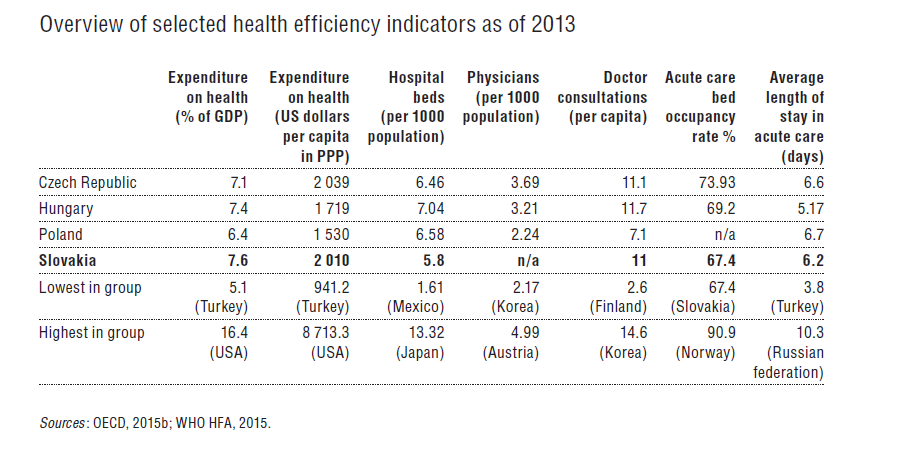
Furthermore, Slovakia, along with the Czech Republic and Hungary, has one of the highest number of doctors’ consultations per capita among OECD members (11 contacts in 2013 versus 7.2 OECD average), which perhaps reflects the inappropriate mix between (supposedly gatekeeping) generalists and specialists.
Allocative efficiency in systems with several insurance funds can suffer from inadequate and unfair resource allocations to individual funds if the risk-adjustment system is not working properly because it has a low predictive ability. Indeed, the Slovak system was long plagued by unfair distributions between the three funds. Therefore, the risk-adjustment scheme, and with that its allocative efficiency, was drastically improved in 2012 after adding PCGs as a risk-adjuster (see section 3.3.2). It has an estimated predictive ability (R2) of 19.65% and redistributes 95% of total SHI contributions.
All three of Slovakia’s health insurers reported first-quarter losses in 2023, according to the Health Care Surveillance Authority (HCSA, 2023). The problem is expected to worsen, with a cumulative loss of approximately EUR 300 million expected for 2023, representing approximately 4% of the health insurers’ total revenues.
The biggest losses and most problems are faced by the state-owned VšZP, with annual losses estimated to be around EUR 240 million and its equity, that is, the value of its assets, falling into negative values by the end of the year. This would result in its liquidation as an insurance company.
Therefore, VšZP’s Supervisory Board, upon request from the Ministry of Health (MoH), prepared an analysis of the reasons for the losses along with a proposal for recovery measures at the end of May 2023. The Supervisory Board approved the proposal, and the MoH directed VšZP to implement 13 of the measures in June; the Supervisory Board is responsible for the supervision of their implementation.
Approximately 40% of VšZP’s losses (and similarly of other insurance companies) stem from errors on the budgeting side. When the MoH switched to programme-based expenditure budgeting in 2022/2023, it began dictating minimum spending amounts to all insurers by care group. However, the MoH does not budget revenues in this detailed way. As a result, VšZP’s revenues have been underestimated by approximately EUR 93.5 million when compared to the way in which the minimum expenditure was set by Decree 100/2023 in March 2023.
Another approximately 40% is accounting shifts. The programme budget is made so that on a cash basis, the revenues and expenditures are balances. However, insurance companies are public limited companies with double-entry accounting and naturally there is a shift between the cash and accounting view. This became significant in 2023, as several amendments to the law shifted the timing of payments for some items that were not covered by revenue in the budget. On the accounting side, though, these are ledgered as a cost. For VšZP, this represents approximately EUR 90 million of the expected loss.
The remainder (roughly 20% of expected losses), is health care expenditures, which are higher than the MoH budgeted for in Programme Decree No. 100/2023. The primary driver of the increase is pharmaceuticals, whose growth is approximately four times the budgeted plan. This is due to the amendment to the Medicines Act in June 2022 (see related Policy Analysis on pharmaceutical reimbursement legislation and reforming categorization processes). Many more medicines are coming onto the market and entering the categorisation process than in previous years, that is, being added to the positive lists of reimbursed medicines, and the impact of this is approximately EUR 50–60 million higher than budgeted for VšZP. Thus, while medicines were expected to grow by around 2% in 2023, the increase is currently estimated at 8% or more. In addition to medicines, spending on laboratory diagnostics or inpatient care is growing faster, which is, for example, due to the opening of two new hospitals in Slovakia (Bory Hospital and Cardiocentrum Šaca in Košice).
As the Ministry of Finance does not have sufficient resources to cover VšZP’s losses in full and savings have to be found on the VšZP side, the recovery plan for VšZP introduced in June 2023 and its 13 measures aim to save approximately EUR 52 million by the end of the year.
The measures are divided into two parts – administrative savings (EUR 11 million) on operations and savings to eliminate above-standard increases on care (EUR 41 million). The latter is primarily aimed at reducing expenditure on laboratory diagnostics and boosting allocative efficiency of company resources. As a part of the effort of the MoH to realise these savings, the CEO of VšZP, R. Strapko was dismissed and interim management is currently in charge (TASR, 2023).
Even if savings are achieved, VšZP will need a top-up of EUR 165 million (that is, 3.8% of the VšZP’s annual revenue) to avoid receivership status next year and additional liquidity problems as early as December 2023.
The Ministry of Finance has not yet promised whether it will proceed with the refinancing, as they are waiting to see if VšZP can enact savings measures this year before guaranteeing additional funding. In May, VšZP already experienced cash problems in paying its liabilities, which is why the MoH proceeded to advance payments. Thus, cash is not currently an issue for the payment of invoices, but only until December 2023, when this payment will be cleared. The MoH therefore has until the end of the year to resolve the situation, but with national elections on 30 September 2023, there is no guarantee that any top-up funding will be able to materialise in time to prevent VšZP’s dire liquidity issues.
References
HCSA (2023). Straty zdravotných poisťovní nemajú rovnakú príčinu (Health insurers’ losses do not have the same cause). Úrad pre dohlad nad zdravotnou starostlivosťou (Healthcare surveillance authority). Available from: https://www.udzs-sk.sk/blog/2023/05/09/straty-zdravotnych-poistovni-nemaju-rovnaku-pricinu
TASR (2023) Minister Palkovič odvolal z funkcie šéfa Všeobecnej zdravotnej poisťovne (Minister Palkovič dismissed the head of the General Health Insurance Company). SME. Available from: https://domov.sme.sk/c/23192316/strapko-vseobecna-zdravotna-poistovna-vszp-odvolanie.html
7.5.2. Technical efficiency
Comparing HLY and health expenditure per capita in US$ PPP among the EU28 countries suggests that the Slovak health system achieves sub-par efficiency (Fig7.10) and that there is room to improve.
Fig7.10

A study by the IMF (Grigoli, 2012) looked into the technical efficiency of 37 OECD country health care systems in 2000–2004 and 2005–2008 using DEA methodology as a tool for comparison. According to this study, the Slovak health care system underperformed heavily during 2000–2004 and achieved an efficiency score of 0.4 (i.e. far below the calculated production frontier). This finding implied that Slovakia could have saved up to 60% of its financial resources if it operated at the same level of efficiency as the most efficient countries in the sample (i.e. Israel, Japan or Malta). The study concluded that in 2005–2008 performance worsened and room for improvement grew to 64% of the total health expenditure per capita. This translated into savings worth 3.4% of the Slovak GDP.
The technical efficiency of the system was further analysed by the Institute for Financial Policy (Filko, Mach & Zajíček, 2012). In December 2012 the Institute conducted an in-depth analysis of the effectiveness of the Slovak health care system by running an OLS model. The study modelled theoretical life expectancy of countries and compared it to actual results while considering the impact of wealth inequalities, alcohol consumption and the post-socialist history of countries on their respective life expectancies. These determinants were identified as having strong impacts on the life expectancy of OECD countries (see Fig7.11). From 2004 to 2007 its performance strongly deteriorated and stabilized at a lower level. Since 2011 the efficiency of Slovak health care is behind the Czech health care system by three years and the OECD average by two years. Slovakia had the largest recorded decline over this period.
Fig7.11
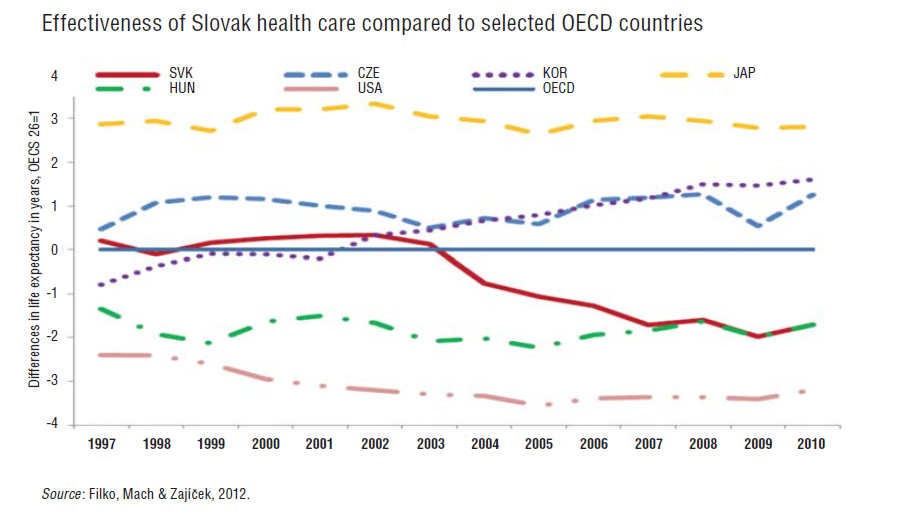
Study authors identified dividend payouts of private insurance companies, poor management of hospitals and pharmaceutical spending as key factors contributing to poor efficiency levels in Slovakia.
In 2013 the last study conducted on the technical efficiency of the Slovak health care system was undertaken by INEKO (Zachar, 2013). Their study included another parameter that influences performance of health care systems: the poverty rate (represented by, for example, the proportion of Roma population). It found that poverty had a significant impact on overall results.
The most recent 2016 Country Report on Slovakia by the EC reconfirmed that despite improvements, weak management of hospitals, a high number of unused acute beds, over-consumption of medicines and poor gatekeeping of the system were still key reasons for overutilization of services and insufficient system efficiency (European Commission, 2016) (see sections 4.1.2 and 5.6, and Table7.7).
Table7.7