-
30 May 2025 | Policy Analysis
Better national anti-drug policies -
18 October 2024 | Country Update
2024–2030 National Strategy to Fight Cardiovascular and Cerebrovascular Diseases -
14 October 2024 | Country Update
Incentives for increasing people’s participation in the screening programmes -
17 January 2024 | Country Update
Measure to reduce antimicrobial resistance -
25 October 2023 | Policy Analysis
National Vaccination Strategy 2023–2030 -
21 September 2023 | Country Update
Development of the National Cancer Registry -
24 April 2023 | Policy Analysis
Approval of the new National Anti-Drug Strategy for 2022–2026 -
08 December 2022 | Country Update
Launch of a programme supporting active case-finding of TB patients -
08 December 2022 | Country Update
Increasing the accessibility of the influenza vaccination -
08 December 2022 | Policy Analysis
The National Plan for Beating Cancer is officially approved -
30 September 2020 | Policy Analysis
A new law seeks to improve prevention and early detection of diabetes -
07 October 2019 | Country Update
Changes to the National Health Programmes -
07 July 2019 | Country Update
Expansion of tuberculosis screening to reach vulnerable populations -
20 November 2018 | Country Update
Improving access to innovative treatment for patients with Hepatitis C -
20 November 2018 | Country Update
Improving access to health care services in underserved areas via the introduction of mobile health units -
15 May 2018 | Policy Analysis
Expanding coverage of palliative care needs -
14 May 2018 | Country Update
Preventive health care interventions among the priorities of the Ministry of Health -
03 July 2017 | Policy Analysis
New strategy to address healthcare-associated infections -
21 May 2017 | Country Update
Innovative treatment for patients with Hepatitis C
5.1. Public health
Public health is defined by Law 95/2006 as “the organized effort of the society towards the protection and promotion of population health” (Title I, Chapter I, Art. 2(1)). Public health services include health promotion, disease prevention and improving quality of life, and comprise the following activities: immunization; control and surveillance of diseases and risk factors; monitoring population health and health determinants; measuring efficiency and effectiveness of health care; assessment of population needs; health promotion and health education campaigns; occupational health; and environmental health, among others. The main strategic document in the area of public health is the National Health Strategy 2014–2020, which includes public health as one of the three main priority areas (see section 2.5 for the general objectives in the field of public health).
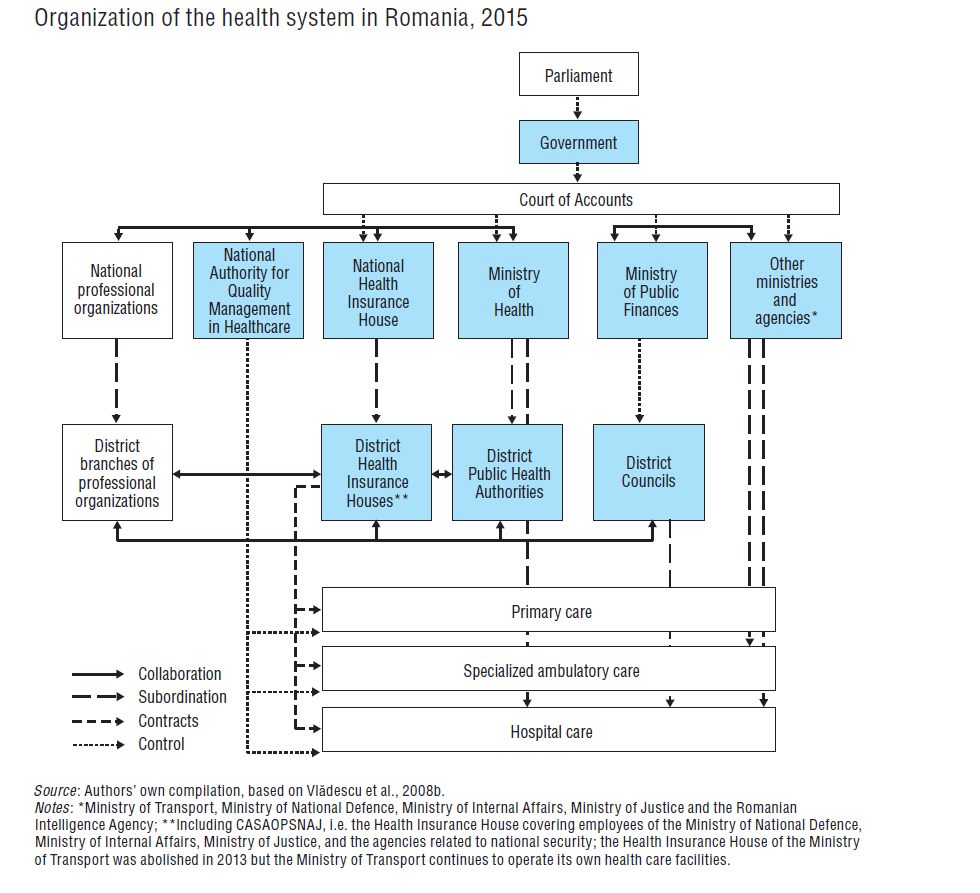
The provision of public health services is coordinated by the Ministry of Health, which is also responsible for the strategic planning and organization of public health services. The NIPH provides technical assistance, including the provision of data, expertise and training, on public health and related matters to the Ministry of Health and other ministries, such as the Ministry of Labour, Family, Social Protection and Elderly, Ministry of Environment, Waters and Forests, and ministries with their own health networks, such as the Ministry of Internal Affairs, Ministry of National Defence (Fig2.1) and other institutions with responsibilities in public health. It comprises four national specialized centres: the National Centre for Environmental Monitoring of Risks in the Community, the National Centre for Communicable Diseases Surveillance and Control (NCCDSC), the National Centre for Methodological Coordination and Information on Occupational Diseases and the National Centre for Health Status Evaluation and Health Promotion, as well as six regional public health centres, which are located in Bucharest, Cluj, Iași, Sibiu, Târgu Mureș and Timișoara, and function as the regional branches of the NIPH. The regional centres have mainly methodological and technical roles.
Fig 2.1
The 42 DPHAs, which represent the Ministry of Health at the local level (see section 2.3), are responsible for the provision of public health services locally, which include: monitoring the health of the population and health determinants; identification of public health needs of communities; performing controls of health institutions; coordinating the implementation of national public health programmes at the local level; carrying out sanitary inspection and health promotion activities, and so on.
Public health activities are also performed as part of medical care services contracted by the DHIHs. They are mainly carried out by family medicine physicians and include: early detection of diseases through check-ups; family planning; antenatal and postnatal care; health education and preventive activities. Family medicine physicians also perform special services under the national public health programmes (e.g. immunizations), which are contracted by the DPHAs. For example, family medicine physicians participate in the screening programme for cervical cancer.
Environmental risks monitoring
The National Centre for Environmental Monitoring of Risks in the Community under the NIPH is responsible for the supervision and monitoring of environmental health. The Centre is divided into specialized departments that are in charge of supervision and monitoring in their respective areas of competence: food and nutrition, occupational health and radiation hygiene. The Centre also coordinates the National Programme of Monitoring Environmental and Occupational Health Determinants implemented by the DPHAs. The NIPH publishes yearly reports on the environmental community risk monitoring.
There are some concerns about the effectiveness of environmental health surveillance and monitoring; for example, in 2014, only about half (48%) of the 50 monitored natural bathing basins were found to be in compliance with the legislative provisions and only 40% of drinking water distribution systems had complied with EC norms; about 5% of drinking water distribution systems were not monitored (NIPH, 2014). There is a comparatively high incidence of diseases that can be attributed to contaminated water in public fountains; for example, in 2010, the incidence of hepatitis A was 16.3 cases per 100 000 population, compared to 2.7 in the EU (WHO Regional Office for Europe, 2016). This can be viewed as a reflection of the low level of preventive measures taken by the DPHAs and family medicine physicians, especially in rural areas, where most communities do not have a sewerage system and people obtain drinking water from public fountains (NIPH, 2014).
Communicable disease surveillance, control and notification
The NCCDSC under the NIPH coordinates surveillance of communicable diseases in the country and is the coordinating competent body that interacts with the ECDC. The legislation on communicable diseases has been harmonized with EU standards. The reporting system covers over 110 communicable diseases, separated into three categories: diseases requiring immediate nominal notification by phone; diseases with nominal notification within five days after detection; and diseases with numerical periodic reporting (weekly, monthly, quarterly and annual). Any doctor who diagnoses a patient with a communicable disease included in the reporting system must report it. In addition, there are networks for the surveillance and control of certain diseases, coordinated by institutions, such as the Institute for Infectious Diseases “Matei Balș” for HIV/AIDS and the Institute of Pneumology “Marius Nasta” for TB, but data collected are also sent to the NCCDSC.
Overall, surveillance of communicable diseases is considered to be well organized and regulated. An assessment by WHO/Europe in 2001 highlighted a number of shortcomings in the epidemiological surveillance system for communicable diseases, identifying a lack of procedures and of microbiology laboratory capacity, as well as some overlapping responsibilities. This was improved in 2003 and 2004 as part of the PHARE programme of financial assistance pre-EU accession, which included enhancing technical capacity, conducting specialized training of epidemiologists and microbiologists, and establishing a coordinating body for the epidemiological surveillance network (Stevens, 2004).
However, there remain challenges in the surveillance of nosocomial infections, which are underreported by hospitals. This is mainly because, in the past, nosocomial infections were included in the individual performance indicators of hospital managers and the latter therefore did not report all cases to avoid being penalized. While the penalties have been abolished, the rate of hospital infections remains included among the indicators against which the performance of hospital managers is evaluated, thus there is an incentive to underreport infection. Efforts are being made to increase awareness of the importance of reporting nosocomial infections, monitoring antimicrobial resistance and reducing their impact. At the time of writing, the Strategic Plan for Prevention and Fighting of Nosocomial Infections 2016–2018 planned that the following measures would be taken in the 2016–2018 period: excluding hospital infection rates from the list of performance indicators; reducing the false reporting of microbiological diagnosis indicators; employing epidemiologists and infectious diseases specialists in all hospitals for antibiotic stewardship; and training hospital managers on the importance of surveillance and reporting.
Occupational health services
Occupational health is regulated mainly by the Law 319/2006 on Occupational Health and Safety. The Ministry of Labour, Family, Social Protection and Elderly, in collaboration with the Ministry of Health, is responsible for elaborating the national policy and strategy on occupational health and safety. The Ministry of Health is responsible for coordinating occupational health services at the national level, surveillance of occupational health through the DPHAs, provision of training and continuing education in occupational health, coordinating research activities, the notification and reporting of occupational diseases, issuing authorizations for occupational health offices and controlling the quality of occupational health services.
According to the legislation, each employer should assure occupational health services such as periodic medical check-ups and prophylactic health care services for their employees, although the extent to which this is being implemented is not regularly monitored. To that end, employers enter into contracts with private occupational health offices or employ an in-house occupational health specialist. The list of prophylactic health care services that employers have to assure for their employees is established by a government decision. If occupational health is perceived to be a public health problem in a given district, occupational health and professional diseases wards must be established within the district hospitals. This is done at the initiative of the DPHAs.
The DPHAs are notified about the incidence of occupational diseases and report on this monthly to the NIPH’s National Centre for Methodological Coordination and Information on Occupational Diseases. The NIPH also provides technical assistance on occupational health to ministries, DHPAs, employers and so on, and carries out research and assessment surveys on occupational risks.
The National Institute for Research and Development in Occupational Health “Alexandru Darabont” conducts scientific research and methodological activities in the area of occupational health and safety. It is also in charge of training and retraining of specialists in health and safety at work and provides technical assistance and consultancy to companies, for example on meeting the provisions of the legislation in force.
Surveillance of population health and well-being
The National Centre for Health Status Evaluation and Health Promotion under the NIPH is responsible for the surveillance of population health and well-being. Population health is evaluated mainly on the basis of general public health statistics published yearly and statistical bulletins on specific aspects of population health published periodically by the National Centre of Public Health Statistics and Informatics. Some aspects of population health are assessed using special surveys, such as surveys of self-perceived population health and health determinants undertaken by the National Institute of Statistics or special projects and initiatives. Examples include the 2012 National Report on Oral Health in Children and Young People and the 2013 Evaluation of the Nutrition Status in 6–9-Year-Old Children within the European Childhood Obesity Surveillance Initiative. Specific organizations, such as the Institute for Infectious Diseases “Matei Balș” for HIV/AIDS and Institute of Pneumology “Marius Nasta” for TB, also undertake assessments. Since 2007, information on cancer patients has been recorded in eight regional registers, coordinated by a National Committee. Through this initiative, the Ministry of Health intended to align Romanian cancer databases with international (WHO, International Agency for Research on Cancer) and European Network of Cancer Registries (ENCR) standards and recommendations.
Health promotion and education and disease prevention
The NIPH is responsible for health promotion and education. Education and information campaigns are also conducted by NGOs as part of specific projects, for example by the Romanian Association for Health Promotion, the Alliance for Fighting Alcoholism and Addictions, the Romanian Association for Education in Diabetes, the Anti AIDS Romanian Association and the Romanian Alliance for Suicide Prevention. There is recognition that the performance of preventive services is “suboptimal” (Ministry of Health, 2014, p. 28) and, in response, the National Health Strategy 2014–2020 (see section 2.5) proposes measures aimed at improving health education for certain vulnerable population groups and particular areas, such as maternal and child health, reproductive health, communicable diseases and healthy lifestyles.
The NIPH also coordinates the development, implementation, monitoring and evaluation of most of the national health programmes financed by the Ministry of Health. The following national health programmes, all renewed on an annual basis, were in place for the 2015–2016 period:
- National Programme for Immunization
- National Programme for Surveillance and Control of Communicable Diseases
- National Programme for Prevention, Surveillance and Control of HIV
- National Programme for Prevention, Surveillance and Control of Tuberculosis
- National Programme for Surveillance and Control of Nosocomial Infections and Monitoring of Antibiotics Use and Antibiotics Resistance
- National Programme of Monitoring Environmental and Occupational Health Determinants
- National Programme for Transfusion Safety
- National Programme for Cancer Screening
- National Programme for Mental Health and Prophylaxis of Psychiatry Pathology
- National Programme for Early Detection of Endocrine Disorders
- National Programme for Mother and Child Health
- National Programme for Health Status Evaluation, Health Promotion and Health Education
- National Programme for Management of National Registries of Chronic Patients
- National Programme for Dietetic Treatment of Rare Diseases
- National Programme for Transplants.
The preventive component of many of these programmes is, however, seen to be weak; for example, the National Programme for Health Status Evaluation, Health Promotion and Health Education includes a subprogramme on the prevention and control of tobacco consumption but it does not include any measures aimed at preventing smoking, instead focusing on the treatment of smoking addictions and supporting smokers who wish to give up smoking.
Some of the national health programmes were specifically established to include screening activities, such as screening for cardiovascular diseases risk factors; cancer (cervical cancer, breast cancer, colorectal cancer, prostate cancer); osteoporosis in women after the menopause; and phenylketonuria, congenital hypothyroidism and hearing screening in newborns. However, there are no publicly available data on the impact of these activities on morbidity and mortality rates (see section 1.4).
Certain preventive services, such as preventive checks-up provided in primary care for people at certain ages, are financed by the NHIF. These check-ups include laboratory tests for the early detection and risk assessment for different diseases (see above).
Access to health promotion and education as well as to disease prevention interventions is considered to be inequitable, with certain vulnerable groups having poorer access, (for example, Roma populations or homeless people) because they are more difficult to reach. The Roma health mediator programme is an example of a measure introduced in order to improve access to health care workers for Roma communities (see section 5.14).
Context
Despite the implementation of the National Anti-Drug Strategy for 2022–2026, illicit drug use, measured in terms of lifetime consumption, increased among adult Romanians aged 15–64, from 10.7% in 2019 to 12.8% in 2024. The consumption is even higher among people aged 15–34, increasing from 16.9% lifetime users in 2019 to 18.2% in 2024.
The strategy is implemented under the coordination and supervision of the National Anti-Drug Agency, subordinated to the Ministry of Internal Affairs, that had been in charge also of the anti-drug policy development, monitoring consumption and assisting consumers through 47 anti-drug prevention, evaluation and counselling centres.
Impetus for the reform (what prompted it)
The existing anti-drug policies, as the previous ones, were highly criticized. Critics argue that they are mainly prone to punishing drug users, who are often declared to be dealers, instead of focusing on prevention and treatment.
In December 2024, the government decided to reorganize the Anti-drug Agency as the National Agency for Policies and Coordination in the Field of Drugs and Addictions, under the subordination and coordination of the Prime Minister. In addition, mental health and addiction prevention centres were developed under the coordination of the National Centre for Mental Health and Drug Control of the Ministry of Health.
Main purpose of the reform
The main purpose of this reform was to attain a better and integrated coordination of the anti-drug policies. Also, the reform will support the Mental Health Action Plan 2024–2029 and in the long run is expected to contribute to the decrease of illicit drug use in Romania.
Content/characteristics
Besides the reorganization of the National Anti-drug Agency that under the direct subordination of the Prime Minister will guarantee better coordination among different sectors and resource pooling, mental health and addiction prevention centres will be created with specific roles in prevention, treatment and rehabilitation of drug users. Further, hospitals will be allowed to establish inpatient wards for the treatment of substance-related addictions.
Implementation steps taken (or scheduled)
The National Agency for Policies and Coordination in the Field of Drugs and Addictions became functional in March 2025 through Government Decision no. 186 that details the roles of the institution, including of the focal point for the European networks and rapid warning system. It also lays out the internal structure, financing and external collaboration.
In May 2025, the MoH published Order no. 1562 on the organization and operating of the mental health and addiction prevention centres, setting their roles, structure and staffing. They are expected to be fully functional in two years.
Outcomes to date and any evaluation
It is too early to evaluate the outcomes. An up-to-date legal framework has been created for better intersectoral collaboration, strengthening governance in the area and ensuring a more preventive and medical approach to the addictions, rather than a corrective one. It is expected that the new approach, guided by the examples of best practices in other countries, will decrease the use of illicit drugs in Romania and improve the mental health of the population.
Cardiovascular and Cerebrovascular Diseases are the main cause of death in Romania, as in most EU countries, but standardized circulatory disease mortality rate is three times higher than EU average: 1005 deaths in Romania compared to 343 deaths in the EU average per 100 000 population in 2021. This difference is associated with a range of socio-economic factors, but also with differences in both the prevalence of risk factors and quality of care.
On 18 October 2024, the Ministry of Health displayed a 2024–2030 National Strategy to Fight Cardiovascular and Cerebrovascular Diseases for public debate, which includes integrated and comprehensive actions towards prevention, early diagnosis and treatment, and patient rehabilitation.
The project of drafting a national strategy on cardiovascular and cerebrovascular diseases was first announced to the public in September 2022. The first draft was published for public debate in January 2024 and a revised draft to be approved by Government Decision was displayed in October 2024.
References
More information (in Romanian):
Overuse of inpatient care and high amenable mortality rates in Romania are due, among other factors, to insufficient preventive services. Screening rates in Romania are very low compared to EU averages (that is, 9% in Romania compared to 66% in the EU for breast cancer, 25% compared to 60% for cervical cancer, and 4% compared to 33% for colorectal cancer in 2019).
One proposed measure to increase the population participation in screening programmes is to grant two paid leave days per year for employees, two free-from-school days per year for students, and two paid leave days per year for employees of the military, security, intelligence, telecommunication or other similar structures.
This proposal was voted in the senate on 14 October 2024, and it was submitted to the Deputies Chamber on 21 October 2024, and it is currently under the parliamentary specialty commissions’ approval process.
References
Antimicrobial resistance (AMR) has been placed among the official public health priorities in Romania, as one of the 2023–2030 National Health Strategy objectives refers to the control of AMR.
The Ministry of Health has issued an order (Order no. 63/2024) approving the outpatient prescription guideline for antibiotics and antifungals. This guideline holds a provision that pharmacists are required to collect several pieces of information when handing out antibiotics and antifungals, including: specific series and number of the prescription generated by prescriptors, patient data, patient diagnosis, and prescribed drug details. Prescriptions will be retained in the pharmacy and, if necessary, they can be dispensed in fractions only within the same pharmacy, without exceeding the total amount prescribed.
This order does not apply to those outpatient prescriptions that are free of charge or partially compensated.
The order also provides that, in medical emergency situations, pharmacists can release certain antibiotics and antifungals without a medical prescription in the maximum amount related to an emergency dose. The emergency dose can be issued only once during a treatment regime, based on a written and signed statement on the patient’s own responsibility.
More information (in Romanian): https://www.ms.ro/ro/centrul-de-presa/nou%C4%83-metodologie-de-monitorizare-a-prescrierii-%C8%99i-de-raportare-a-eliber%C4%83rii-medicamentelor-antibiotice-%C8%99i-antifungice-de-uz-sistemic-%C3%AEn-contextul-riscurilor-generate-de-utilizarea-excesiv%C4%83-a-acestora
Context
Vaccination coverage is very low in Romania, compared to WHO-set targets, and is decreasing over time. For example, influenza vaccination reached 21.3% of the population in 2022, while the WHO set target is 75%. A law on mandatory vaccination drafted in 2017 (following a significant measles outbreak that occurred in Romania in 2016) was withdrawn from the parliamentary debate after facing strong opposition both at political and public levels. The only measures taken to increase the vaccination rates over the last years were to include the pharmacists among the vaccinators for influenza, and to make certain vaccines available in community pharmacies.
Impetus for the reform
The necessity for a vaccination strategy was acknowledged by the Ministry of Health as a measure to prevent possible outbreaks or re-emergence of certain communicable diseases. Further, the need for defining strategic directions in this area was driven by international requirements and initiatives, such as the Council Recommendation of 7 December 2018 on strengthened cooperation against vaccine-preventable diseases or the WHO Immunization Agenda 2030: A Global Strategy to Leave No One Behind, and by national strategic documents such as the National Health Strategy 2023–2030 and the 2030 National Strategy for the Sustainable Development of Romania.
Main purpose of the reform
The main purpose of the reform is ensuring equitable access to safe and effective vaccination services, contributing to better population health so that everyone, at any time, at any age can benefit from vaccines for their own health and well-being.
Content/characteristics of the reform
The strategy has a holistic approach intending to act on multiple directions, namely:
- ensuring the proper policy and regulatory framework to encourage vaccination uptake,
- ensuring lifelong universal access to vaccination,
- ensuring continuity in the vaccine supply and their efficient use,
- continuously improving the vaccine safety monitoring systems,
- strengthening the monitoring and evaluation of the National Vaccination Programme by analyzing the data from the national vaccination register (RENV) and the surveillance data of vaccine-preventable diseases,
- ensuring sufficient numbers of trained human resources, hence, increasing surveillance capacity for vaccine-preventable diseases,
- improving communication to increase the population's confidence in the benefits of vaccination through sustainable social partnerships, and
- enhancing the implementation of the European region vaccination policies.
Implementation steps taken (or scheduled)
The strategy has an Implementation Action Plan with specific tasks, responsible institutions, monitoring indicators, expected results, deadlines, estimated costs and a source of financing for each specific objective. For most of the tasks, the responsibility is shared among the Ministry of Health, district health authorities, specialized institutions, professional organizations and civil society. Further, institutions from the education and social sectors are involved.
Outcomes to date and any evaluation
The strategy was approved in October 2023. First steps for the implementation to be taken in 2024 would consist of legislative adjustments and additions, vaccines procurement and reserve stocks procedures, updated methodologies for the surveillance of postvaccination adverse reactions and quality assurance of the National Electronic Vaccination Registry data.
References
HSPM update: Increasing the accessibility of the influenza vaccination, 8 December 2022, https://eurohealthobservatory.who.int/monitors/health-systems-monitor/updates/hspm/romania-2016/increasing-the-accessibility-of-the-influenza-vaccination
HSPM update: Increasing influenza vaccination coverage, 16 august 2023, https://eurohealthobservatory.who.int/monitors/health-systems-monitor/updates/hspm/romania-2016/increasing-influenza-vaccination-coverage
Government of Romania (2023), Nota de Fundamentare la Hotărârea Guvernului nr. 1006/2023 privind aprobarea Strategiei naționale de vaccinare în România pentru perioada 2023 – 2030 [Substantiation note for the Government Decision 1006/2023 on the approval of the National Vaccination Strategy 2023-2030] https://gov.ro/ro/guvernul/procesul-legislativ/note-de-fundamentare/nota-de-fundamentare-hg-nr-1006-20-10-2023&page=1
Government of Romania (2023), Proiectele de acte normative care ar putea fi incluse în şedinţa Guvernului României din 20.10.2023/PROIECT DE HOTĂRÂRE DE GUVERN privind aprobarea Strategiei naţionale de vaccinare în România pentru perioada 2023 – 2030 [Legislation proposed to be included on the Romanian Government agenda of 20.10.2023/DRAFT GOVERNMENT DECISION on the approval of the National Vaccination Strategy in Romania 2023 – 2030] https://sgg.gov.ro/1/proiectele-de-acte-normative-care-ar-putea-fi-incluse-in-sedinta-guvernului-romaniei-din-20-10-2023
The National Plan for Beating Cancer, officially launched in November 2022, includes as a specific objective the development of a National Cancer Registry (NCR) linked to the European Network of Cancer Registries (ENCR). In August 2023, the Romanian Government passed the decision of establishing the NCR under the administration of the National Institute of Public Health. The NCR objectives include gathering information on all cancers to support the monitoring of cancer incidence, the evaluation and control of the disease, and substantiating health policies in the field.
In September 2023, an order by the Minister of Health approved the reporting template to be used, the “minimum dataset” (that is, the minimum information to be included in the database), and the organization of the reporting activity (including, for example, the description of activities and responsibilities of each structure and the relationship among them). The data to be reported are in accordance with the recommendations of the Joint Research Centre of the EU and of the ENCR. The order also establishes eight regional coordination centres, their structure, tasks and responsibilities, ranging from data collection to dissemination of information, including provisions related to data protection and confidentiality.
More information (in Romanian):
Context
Illicit drug use among adult Romanians aged15–64 saw an increase between 2013 and 2019, as measured in terms of lifetime consumption (10.7% in 2019 versus 6.6% in 2013), consumption over the last year (6% versus 2.5%), and consumption over the last month (3.9% versus 1.1%). Illicit drug use is higher among people aged 15–34, who in 2019 accounted for 16.9% of lifetime users, 10% of those reporting consumption over the last year and 6.6% of those reporting consumption over the last month (National Anti-Drug Agency, 2022). Although Romanian students report a relatively low perceived availability of illicit drugs (ESPAD, 2019), drug trafficking statistics show an increase in this area (National Anti-Drug Agency, 2022).
Overall, demand for treatment after consuming drugs increased between 2013 and 2020 (Government of Romania, 2022a), and the objectives of the policy documents that were in place in this period – the National Anti-Drug Strategy 2013–2020 and the National Programme for the prevention, and medical, psychological and social care of drug users 2015–2020 – in terms of improving the prevention of drug use and treatment services for drug users were only partially achieved. This was to some extent attributed to the COVID-19 pandemic, during which provision of preventive interventions in schools, counselling services for drug users, and treatments for diseases related to drug use, were limited. Nevertheless, the number of medical emergencies and deaths associated with illicit drug consumption decreased between 2019 and 2021 (National Anti-Drug Agency, 2022).
Content of the reform
The new National Anti-Drug Strategy for 2022–2026 was approved by the Government of Romania in 2022. It ensures the continuity of previous activities in this area and is aligned with the objectives set out in resolution adopted during the 30th Special Session of the United Nations General Assembly on the World Drug Problem in 2016 and the objectives set out in the EU Drugs Strategy 2021–2025. Romania’s new strategy was developed in a collaborative and transparent manner, involving and setting responsibilities for all relevant sectors and stakeholders, including the National Anti-Drug Agency, the police, the Ministry of Health, the Ministry of Education, the Ministry of Family, Youth and Equal Opportunities, local authorities and the civil society (Government of Romania, 2022a).
The Government also approved the new National Programme for the prevention, and medical, psychological and social care of drug users 2023–2026. This programme sets out interventions to be implemented for each specific objective of the National Anti-Drug Strategy (Government of Romania, 2022b). These interventions focus on the prevention of drug use by implementing measures targeted at schools and families (e.g., school counselling sessions with students or parents), communities (e.g., counselling sessions for refugees, or in workplaces), or through Information Education Communication (IEC) campaigns addressed to the population of people aged 15–34; treatment of drug users through provision of integrated services for reducing the risks associated with drug consumption, provision of basic treatment services, case management, substitution treatment, testing for infectious diseases, overdose treatment, etc. The Programme also includes intersectoral coordination measures, monitoring of national drug policy, training and research activities. The total budget allocated for this Programme is 32 300 000 RON (approximately 6 460 000 Euros).
References
National Anti-Drug Agency (2022), Raport național privind situația drogurilor [National Report on Drugs] http://ana.gov.ro/rapoarte-si-studii/ (accessed 14 March 2023)
ESPAD (2019), Report 2019. Results from the European School Survey Project on Alcohol and Other Drugs, The ESPAD Group http://www.espad.org/espad-report-2019 (accessed 14 March 2023)
Government of Romania (2022a), Strategia Națională în domeniul drogurilor 2022–2026 [National Strategy on Drugs 2022-2026] http://ana.gov.ro/despre-institutie/programe-si-strategii-proprii/ (accessed 14 March 2023)
Government of Romania (2022b), Programul naţional de prevenire şi asistenţă medicală, psihologică şi socială a consumatorilor de droguri, pentru perioada 2023-2026, [National Programme for prevention, and medical, psychological and social care of drug users 2023-2026] https://lege5.ro/Gratuit/geztcnbshazdq/programul-national-de-prevenire-si-asistenta-medicala-psihologica-si-sociala-a-consumatorilor-de-droguri-pentru-perioada-2023-2026-din-28122022?d=2023-03-14 (accessed 14 March 2023)
In early November 2022, a campaign supporting active case-finding of tuberculosis (TB) patients was launched in 11 districts in Romania. The project is part of a programme titled “Approaching challenges for health system on control of TB in Romania”, which runs between 2018 and 2023 and is financed by the Global Fund. The aim is to enhance health system’s capacity to prevent, diagnose and treat TB.
As part of the campaign, mobile caravans, provided and coordinated by the District Public Health Authorities are sent to deprived areas and communities with a high TB prevalence within their territories and test all persons over 18 years old who are at risk of TB, irrespective of their insurance status, including refugees from Ukraine.
The methodology, testing procedures, the roles and responsibilities of different actors and the financial arrangements are outlined in the Ministry of Health’s Order no. 3326 issued on 28 October 2022.
More information (in Romanian):
https://www.ms.ro/2022/11/03/program-de-depistare-activa-a-tuberculozei-in-11-judete/
According to the Ministry of Health’s Order no. 3262 from 19 October 2022, community pharmacists have been permitted to administrate the influenza vaccine. This Order is meant to facilitate access to vaccination and includes a guide of good practice and lists conditions that pharmacies must meet in order to be authorized to provide the vaccination.
Previously, only family doctors were authorized to administrate the vaccine. According to the National Immunization Programme, influenza vaccine is provided and administered for free by family physician to the population at risk as defined by the WHO, that is, including older people, chronic patients, pregnant women, etc.
The rest of the population can buy the vaccine from a pharmacy. Allowing pharmacies to also administer the vaccine is hoped to increase the vaccination rate, which at 8% of the general population (2021/22 season) is very low in Romania.
More information (in Romanian):
Context
Historically, cancer has been the second cause of death in Romania, except for 2021 when it was surpassed by respiratory diseases due to COVID-19 pandemic (INSP-CNSISP, 2022). Lung cancer is the most frequent cause of cancer death (3.9% of all deaths in 2020), followed by colorectal cancer (2.5%) and breast cancer (1.4%). Mortality rates for all cancers have seen an increasing trend in recent years (OECD, 2021). While cancer incidence is lower in Romania compared to the EU average, cancer mortality is higher, reflecting weaknesses in cancer diagnosis and treatment (OECD, 2021). The situation is expected to worsen, in part due to the COVID-19 pandemic, which affected both the diagnosis and treatment of cancer patients, and in part due to the high impact of risk factors, such as unhealthy diet, tobacco and alcohol consumption, and air pollution. These factors contribute to Romania’s poor performance among the EU countries in terms of both amenable mortality (the highest rate in the EU at 250 per 100,000 population vs. the EU27 average of 111), and preventable mortality (second highest, after Hungary, at 95 per 100,000 population vs. the EU27 average of 55) in 2019 (as calculated by the European Observatory for Health Systems and Policies based on WHO data).
Impetus for the reform
A few months after the release of the Europe’s Beating Cancer Plan in February 2021, the Romanian Parliament appointed a working group charged with the development of a National Plan for Beating Cancer (Camera Deputaților, 2022). To support these efforts, a dedicated online platform “Împreună învingem cancerul” [Together beat the cancer] (https://cancer-plan.ro) was created by the Romanian Association of International Medicines Producers (ARPIM) as a dialogue and public debate forum for professionals, patients’ associations and the media.
The National Plan for Beating Cancer was finalized in January 2022, voted through by the Senate (September 2022) and the Deputies Chamber (October 2022) and on 2 November 2022 the President of Romania promulgated the Law thereby officially approving this Plan (Raportul de Garda.ro, 2022).
Content of the reform
The National Plan for Beating Cancer will be implemented during 2023–2026. Its main objective is to define the patient pathway in order to ensure an integrated, multidisciplinary approach. Specific objectives include the establishment of a health innovation fund to offer early access to the best therapies; developing supporting services for cancer patients such as nutrition advice, psychological support and palliative services; developing a prevention strategy and monitoring risk factors; developing a National Cancer Registry linked to the European Network of Cancer Registries; periodical updating of the clinical guidelines and treatment protocols; and introducing a tumor board in cancer care (to review patient’s condition and discuss treatment options) and personalized medicine.
The National Plan for Beating Cancer is financed by the Ministry of Health. The Plan has a dedicated annual budget that amounts to 20% of the total budget for national health programmes. The health innovation fund will be set up and financed by the Ministry of Finance (Parlamentul României, 2022).
References
INSP-CNSISP (2022) [National Institute of Public Health-National Center for Statistics and Informatics in Public Health]. Cauze de deces în Romania. Anul 2021 comparativ cu 2020 [Death causes in Romania 2021 compared with 2020] https://insp.gov.ro/centrul-national-de-statistica-in-sanatate-publica-cnssp/date-statistice-pagina-de-descarcare (accessed 6 December 2022)
OECD (2021) State of Health in the EU Romania Country Health Profile 2021 https://read.oecd-ilibrary.org/social-issues-migration-health/romania-country-health-profile-2021_74ad9999-en#page1 (accessed 6 December 2022)
Camera Deputaților (2022) [Deputies’ Chamber] > Structuri parlamentare 2020-prezent > Parlamentul României > Comisii > Combaterea cancerului [> Parliamentary Structures 2020-present > Romanian Parliament > Commissions > Cancer Fight] https://www.cdep.ro/pls/parlam/structura.co?cam=0&idc=231 (accessed 6 December 2022)
Raportul de Garda.ro (2022), https://raportuldegarda.ro/lege-plan-national-prevenire-combatere-cancer-presedinte-romania/ (accessed 6 December 2022)
Parlamentul României (2022) [Romanian Parliament] Lege nr. 293 din 08 noiembrie 2022 pentru prevenirea şi combaterea cancerului [Law on prevention and fighting cancer] Monitorul Oficial nr. 1077 din 03 noiembrie 2022 [Official gazette no. 1077 from 08 November 2022] https://lege5.ro/Gratuit/gezdsmzzguyte/legea-nr-293-2022-pentru-prevenirea-si-combaterea-cancerului (accessed 6 December 2022)
Context
Diabetes is one of the public health priorities in Romania, with increasing incidence, from 321.2 cases per 100 000 population in 2011 to 397.2 cases per 100 000 in 2019 (INSP, 2020), and prevalence, from 3% in 2011 to 3.9% in 2019 (WHO – HFA, 2020). However, prevalence data reported to the WHO are based on family medicine physicians’ records, which seem to underestimate the real number of cases. The National Institute of Public Health (NIPH) reported prevalence of 6.0% in 2019, based on the cases reported by diabetes and metabolic diseases specialty offices (INSP, 2020). This higher prevalence figure could also indicate that diabetes is discovered in an advanced stage of the disease when patients report to hospitals to treat complications. According to the estimates from the Romanian Diabetes Forum (https://www.forumdiabet.ro), about 70% of diabetes cases are diagnosed in later stages of the disease and 40% of the cases do not comply with the treatment (Forumul Român de Diabet, 2019). Mortality from diabetes is also a matter of concern, having increased from 9.9 cases per 100 000 population in 2011 to 12.9 cases per 100 000 population in 2019 (INSP, 2020).
Impetus for the reform
The Romanian Diabetes Forum (which is a dialogue platform gathering several professional and patients’ associations that was initiated in 2019 by the Romanian Society of Diabetes, Nutrition and Metabolic Diseases with the support of the Romanian Association of International Medicine Manufacturers) has organized several consultations on prevention and early detection of diabetes with the medical community, patients’ associations, authorities, experts, and the pharmaceutical industry. At the beginning of 2020, the Law on prevention and early detection of diabetes was submitted to the Parliament, and on 13 November 2020, it was promulgated by the Romanian President (Forumul Român de Diabet, 2019).
Since the implementation of the reform is conditioned on the issuance of the secondary legislation, the Romanian Diabetes Forum remains committed to further action.
Content of the reform
The main purpose of this law is to improve prevention and early detection of diabetes, but also to raise awareness and to encourage a healthy and responsible lifestyle in the population. The main tool provided by the law is the National Programme for Diabetes Prevention, which will be approved by a Government Decision every four years. This will include measures for primary prevention and reduction of risk factors, measures for early detection of persons at risk, and measures to avoid progression of the disease. The Programme will be financed by the Ministry of Health. The Law also establishes the National Diabetes and Pre-diabetes Registry as a component of the Electronic Information Health Insurance Platform.
The Law offers the prerequisites for an interagency and intersectoral collaboration, setting tasks for health providers, district health insurance houses, integrated community centres, local authorities, and the Ministry of Education (Parlamentul României, 2020).
At the time of writing (September 2020) the secondary legislation has not been issued yet.
References
WHO – HFA database (2020) https://gateway.euro.who.int/en/hfa-explorer (accessed 26 September 2020)
INSP (2020) [National Institute of Public Health]. Raportul Național al Stării de Sănătate a Populației 2020 [National report on population health status 2019]
Ministerul Sănătății (2011), [Ministry of Health] Ordinul nr. 1014/2011 privind înființarea și funcționarea Registrului național de diabet zaharat [Order no. 1014/2011 on the establishment and functioning of the National Diabetes Registry] https://legislatie.just.ro/Public/DetaliiDocumentAfis/129291 (accessed 26 September 2020)
Forumul Român de Diabet (2019) [Romanian Diabetes Forum]. Diabetul în România [Diabetes in Romania] https://www.forumdiabet.ro (accessed 26 September 2020)
Parlamentul României (2020) [Romanian Parliament] Lege nr. 249 din 13 noiembrie 2020 privind prevenţia şi depistarea precoce a diabetului [Law on prevention and early detection of diabetes] Monitorul Oficial nr. 1079 din 13 noiembrie 2020 [Official gazette no. 1079 from 13 November 2020] https://legislatie.just.ro/Public/DetaliiDocument/233148 (accessed 26 September 2020)
Existing national health programmes are typically renewed
annually through a Government Decision, and incorporate changes put
forward by the Ministry of Health. In June 2019, the following changes
have been approved:
(1) The National Programme for the evaluation
of vitamin D deficiency in the population at risk has been introduced
in response to increased incidence of rickets and other diseases related
to vitamin D deficiency.
(2) The National Programme for Cancer
Screening was supplemented with a sub-programme dedicated to the early
detection of tumour markers in the population at risk. This is hoped to
ensure earlier treatment, decrease cancer mortality rates and lead to
cost savings.
(3) The National Programme for Mental Health and
Prophylaxis of Psychiatry Pathology was supplemented with training in
approaching patients with autism spectrum disorders. Training will be
available to health professionals and patient’s family and is expected
to increase service quality.
The National Programme for Prevention, Surveillance and
Control of Tuberculosis covers passive case finding, diagnostics,
epidemiological surveys and preventive treatment of persons who have
been in contact with diagnosed cases as well as information, education
and communication campaigns. Despite a decreasing trend, Romania has the
highest TB incidence among the EU countries, with 9 818 new cases
reported in 2018.
Since 2018, an active TB screening programme
has been introduced among the more vulnerable populations. The new
screening programme was introduced within the project ”Organization of
early detection (screening), diagnostic and treatment programmes for TB,
including latent TB infection” co-financed from the EU structural
funds. The project will end in 2023 and has a total cost of 64 million
lei (approx. 13.6 million euros). It will covers over 75 010 thousand
vulnerable individuals, including people from rural communities,
homeless people, alcohol and substance addicts and prisoners.
At the end of September 2018, the National Health Insurance
House (NHIH) announced that Hepatitis C treatment will be made
available to 13000 patients in all stages of fibrosis. The number of
contracted providers was also increased. Access to innovative treatment
for Hepatitis C has been extended since 2016, when an innovative
interferon free treatment was made available to 5860 patients with
advanced stage of fibrosis (F4). In 2017 treatment was offered to almost
10000 patients, including those in stages F3 and F2 (see Reform Log
dated 22.05.2017).
Prevalence of Hepatitis C virus infection
stands at 3.3% of the Romanian population (over 660 thousand people),
which is the highest rate in the European Union. The measures described
above are meant to contribute to the WHO and EU efforts to eliminate
Hepatitis C by 2030.
More information (in Romanian): http://www.cnas.ro
Authors
Mobile health units were introduced by the Law 95 on Health
Care Reform in 2006. They were meant to improve access to health
services in rural or remote areas and in areas where access to health
services is limited by lack of human resources or economic factors.
However, their organization and functioning was not regulated and their
availability was limited to a few private initiatives.
In order
to remedy this situation, in May 2018 the Ministry of Health issued an
order regulating the establishment, organization and operation of mobile
medical units. Eight mobile units for provision of screening services
for cervix cancer were procured within an ongoing project financed by
the World Bank.
For more information (in Romanian) see: https://www.caravanacumedici.ro
Authors
Context
Population aging and the increasing incidence of cancers and chronic illnesses have resulted in an increase of people with life-limiting illnesses and with specific care needs such as relief from pain and other symptoms of a terminal illness. Palliative care was developed in Romania after 1990, through initiatives organized by various NGOs and with international financial support. However, the lack of supporting legislation and appropriate training has resulted in poor availability of palliative care in Romania.
A study conducted within the EU-financed pre-accession programme to assist applicant countries from Central and Eastern Europe (PHARE) in 2010 showed that 76.5% of terminally ill persons were cared for only by family members, with 20.7% of the Romanian population (approximately 4.3 million people) having to provide such care to their relatives (Hospice Casa Speranței, 2013).
Impetus for the reform
Improving palliative care is included as one of the goals in the main policy frameworks that guides the ongoing development of health services to ensure the health and wellbeing of Romanian citizens: the National Sustainable Development Strategy 2013–2020–2030 aims to expand coverage of palliative care needs to 60% by 2020 (Government of Romania, 2008), and the National Health Strategy 2014–2020 includes measures for the development of these services (Ministry of Health, 2014).
Content of the reform
Measures to develop palliative care are supported by the 2014 Improving Health System Quality and Efficiency project financed by the World Bank which aims to establish, by 2020, 29 palliative care units in hospitals (by allocating some of the existing acute care beds to palliative care), 90 home care teams and 90 outpatient clinics. The project also includes funding to develop training of GPs and community nurses to deliver basic palliative care (Moșoiu et al., 2918).
Further developments of palliative care services are also supported by two recently passed regulations. In 2017, an order of the Ministry of Health included palliative care among the specialties available to nurses after finishing their basic nursing training. Another order, from March 2018, set out the framework for the organization and functioning of palliative care services: it classifies palliative care services into three complexity levels; defines the beneficiaries of palliative care; establishes standards for palliative care professionals (e.g. the type and number of professionals needed for each level of care and their qualifications; patient pathways and ways of communication among different health personnel involved in order to ensure coordination and integration of services provided).
Besides the goal of reaching 60% coverage of palliative care needs by 2020, as set by the National Sustainable Development Strategy 2013–2020–2030, some outcome indicators to evaluate the implementation of this policy are set by the National Health Strategy 2014-2020. In particular, the number of newly established palliative care providers and the number of palliative care providers contracted by the National Health Insurance House (NHIH) are used to assess the development of palliative care in Romania. At the time of writing, the number of palliative care providers contracted by the NHIH is the only indicator available, which has increased from 56 to 69 in the period 2013 - 2015 (Ministry of Health, 2016). In 2016, less than 10% of the estimated palliative care needs in the country were covered (Ministry of Health, 2017).
References
Hospice Casa Speranței (2013). Studii paliative [Hospice Casa Speranței. Palliative studies] / Programul național de îngrijiri paliative [National programme for palliative care] HOSPICE Casa Speranței © 2013-2018 (http://www.studiipaliative.ro/programul-national-de-ingrijiri-paliative/,accessed 27 March 2018)
Ministry of Health (2017). Referat de aprobare a Regulamentului de organizare, funcționare și autorizare a serviciilor de îngrijiri paliative [Request for approval of the Regulation for the organization, functioning and authorization of palliative care services]
Government of Romania (2008). National Sustainable Development Strategy Romania 2013–2020–2030. Bucharest, Government of Romania (http://www.un.org/esa/dsd/dsd_aofw_ni/ni_pdfs/NationalReports/romania/Romania.pdf, accessed 27 March 2018)
Ministry of Health (2014). Strategia Națională de Sănătate 2014–2020. Sănătate pentru prosperitate [National Health Strategy 2014–2020. Health for wealth]. Bucharest, Ministry of Health
Moșoiu, D., Mitrea, N., Dumitrescu, M. (2018). Palliative Care in Romania, Journal of Pain and Symptom Management, S67, Vol. 55, No. 2S, February 2018 (http://www.jpsmjournal.com/article/S0885-3924(17)30384-6/pdf, accessed 27 March 2018)
Ministry of Health (2016). Strategia Națională de Sănătate 2014–2020. Sănătate pentru prosperitate. Raport anual privind stadiul implementării. 2015. [National Health Strategy 2014–2020. Health for wealth. Annual report on implementing stage. 2015]. Bucharest, Ministry of Health
In April 2018, the Minister of Health announced the
introduction, by the end of the year, of screening programmes for breast
and cervical cancers and for risk factors for cardio-vascular diseases.
Funding will come from the EU structural funds and from the World Bank,
with a certain percentage of the programmes costs covered from national
sources.
Breast cancer screening and cervical cancer screening
are estimated to cost 21 and 45 million euros, respectively. Programmes
will be implemented through eight regional cancer screening centres,
which will be established within district hospitals. Five such centres
are already being established and will be functional by the end of the
year.
The screening programme for risk factors of cardio-vascular
diseases received funding (25 million euros) for five years of
operation. The programme will be implemented by family physicians, who
will receive an additional pay for this new task, in collaboration with
cardiologists. The programme is among the priorities of the Ministry of
Health (and is listed as such in the 2014 National Health Strategy).
More information (in Romanian):
https://www.agerpres.ro/sanatate/2018/03/20/ministrul-sanatatii-anunta-ca-va-fi-introdus-un-program-de-screening-privind-factorii-de-risc-pentru-bolile-cardiovasculare--76313
https://www.agerpres.ro/sanatate/2018/03/16/ministrul-sanatatii-spune-ca-se-vor-infiinta-opt-centre-de-screening-pentru-cancerul-de-san-si-de-col--74306
Authors
Context
The reported annual rates of nosocomial or healthcare-associated infections (HAI) in Romania between 1995 and 2015 varied between 0.3% and 0.7% of patients (CNSCBT, 2015). However, a point prevalence multi-country survey conducted by the ECDC in 2012 which included ten hospitals in Romania reported a much higher rate: 2.8% of patients with at least one HAI on a given day, and over 5% for the re-validated data in five hospitals. This is more in line with the EU average rate of 5.7% and indicates that the nationally reported figures are likely to underestimate the actual rates (ECDC, 2017). The following factors may suggest that this is indeed true: the very low number of epidemiologists and hygiene nurses in hospitals; lack of compliance with hygiene and other HAI prevention norms of medical staff; old hospital infrastructure with no advanced isolation units; and high bed occupancy rates in some hospitals. However, the main reason for underreporting is the fact that the rate of nosocomial infections has been included among the indicators against which the performance of hospital managers is evaluated.
Impetus for the reform
The government that acceded to power in November 2015 listed HAI prevention as one of the internal processes to be improved in order to attain its health policy objectives (Government of Romania, 2016). This may have been partly motivated by public pressure following a nightclub fire in Bucharest earlier in October (that also precipitated the change of government). The media revealed that many of the fire’s burn patients died or had to be transferred to clinics outside of Romania due to multi-drug-resistant nosocomial infections.
Consequently, in April 2016, a Strategic Plan for Prevention and Fighting of Nosocomial Infections 2016–2018 was launched. This plan was developed based on findings of site cross-checking evaluation of a sample of 112 hospitals.
Content of the reform
The main objectives of the HAI prevention policy are: (1) Increasing capacity for diagnosis, prevention and control of HAI; (2) Development of an effective reporting system; (3) Improving surveillance and reducing antibacterial resistance in the hospitals; and (4) Reducing the overuse of antibiotics. The measures to be implemented during 2016–2018 include: development of the legislative framework, development of an investment plan in order to improve the endowment of the microbiology laboratories and HAI control and prevention structures of the hospitals, and training the staff involved in the prevention, surveillance, diagnosis and control of HAI (Ministry of Health, 2016a).
The implementation of this policy will be evaluated based on indicators set out in the National Programme for Surveillance and Reduction of HAI. They include a prevalence study of the HAI and sentinel surveillance in the high risk departments. The targets set for 2018 for the 108 hospitals included in the Programme are: an increase in HAI reporting to 2% of patients, and of HAI incidence to 5% in the sentinel surveillance medical units. The only data available on these indicators for 2015 is the HAI incidence in the sentinel surveillance medical units, which was 2.51% (Ministry of Health, 2016b). The 2016 values are not yet available.
References
CNSCBT (2015). [National Centre of Surveillance and Control of Communicable Diseases] Consumul de antibiotice, Rezistența microbiană și Infecții Nosocomiale în România-2015 [Antibiotic consumption, Antimicrobian resistance and nosocomial infections in Romania] (http://www.cnscbt.ro/index.php/analiza-date-supraveghere/infectii-nosocomiale-1/684-consumul-de-antibiotice-rezistenta-microbiana-si-infectii-nosocomiale-in-romania-2015/file, accessed 13 June 2017)
ECDC (2017). European Centre for Disease Prevention and Control. Exploring opportunities for support in healthcare-associated infections – Romania, 4–7 July 2016. Stockholm: ECDC; 2017. (http://ecdc.europa.eu/en/publications/Publications/mission-report-HAI-Romania-4-7-July-2016.pdf, accessed 13 June 2017)
Government of Romania (2016). Priorități strategice și planuri de acțiuni sectoriale ale ministerelor pe anul 2016 [Strategic priorities and sectorial action plans of ministries for 2016] 15 January 2016
Ministry of Health (2016a). Lansarea Planului Strategic de Prevenire şi Combatere a Infecţiilor Nosocomiale [Launch of the Strategic Plan for Prevention and Fighting of Nosocomial Infections 2016–2018]. Comunicate de presa[Press Release] 26 Aprilie 2016 Bucharest, Ministry of Health.
Ministry of Health (2016b).Strategia Națională de Sănătate 2014–2020. Sănătate pentru prosperitate. Raport annual privind stadiul implementării. 2015. [National Health Strategy 2014–2020. Health for wealth. Annual report on implementing stage. 2015]. Bucharest, Ministry of Health.
Since 2016, the very expensive interferon free treatment
for Hepatitis C has been reimbursed by social health insurance for
patients with stage 4 of fibrosis. Hence, innovative treatment has been
made available for only 5,860 patients, while the total number of
patients registered with Hepatitis C in Romania is 16,000. From 2017,
the interferon free treatment for Hepatitis C will be extended to
patients with less advanced stages of fibrosis (F3 and F2). The National
Health Insurance House has announced that new cost-volume-outcome
contracts will be signed to cover the treatment of almost 10,000
patients with Hepatitis C in different stages of fibrosis.
More information (in Romanian):
http://www.cnas.ro