-
12 September 2025 | Country Update
Hospital Reform in Poland -
26 January 2024 | Policy Analysis
National Health Fund tasked with financing non-insurance-based healthcare services
6.1. Analysis of recent reforms
Health sector reforms that took place between the publication of the last Health in Transition report (2011) and the cut-off date of the current report (August 2018) can be divided into two periods: (1) reforms implemented between 2011 and late 2015, under the Civic Platform and the Polish People’s Party coalition government (in power since 2008), and (2) reforms implemented under the rule of PiS, which started at the end of 2015.
In September 2025, a law amending the regulations on publicly funded healthcare services and medical activity, known as the hospital reform, was published. This allows network hospitals, with approval from the National Health Fund (NFZ), to transition from providing full hospitalization to offering planned, one-day or long-term care. Local governments can now establish and merge public healthcare institutions. The law also introduces a requirement to prepare recovery programmes for indebted hospitals and analyze their efficiency. The act will come into force on 17 September 2025. This reform is a key part of the National Recovery Plan, which allocates over 17 billion PLN for healthcare, including hospitals. Financial support mechanisms for indebted hospitals are currently lacking, although they are expected soon.
The amendment to the Act on the Medical and Dental Professions and certain other acts introduces significant changes to the financing system of the Polish public healthcare system. According to the new regulations, the National Health Fund (NHF, Polish: Narodowy Fundusz Zdrowia, NFZ) was tasked with financing a wide range of non-insurance-based services, which were previously financed from the state budget and guaranteed to all people in Poland, regardless of their statutory insurance status.
The NHF took over the financing of
- emergency medical services;
- medicines for people over 75 and pregnant women;
- highly specialized services;
- compulsory vaccinations;
- insurance contributions for students, soldiers and the unemployed; and
- medicines under the health policy programmes of the Ministry of Health:
- treatment of haemophilia,
- antiretroviral treatment for people living with HIV, and
- antiviral treatment for hepatitis C for prisoners.
Previously, all these tasks were financed from the state budget. Currently, these tasks are financed from compulsory health insurance contributions (paid as a payroll tax via the social insurance system), without any further increase in this source of NHF income [2].
The reform was met with numerous protests from the medical community, mainly due to the lack of guaranteed additional financial resources for the NHF. As a result, patients’ access to health services may be restricted. The reform was introduced at a time when the NHF has been experiencing a budget surplus since 2021 due to unused health services, initially due to COVID-19 and later due to a shortage of professionals [3]. The surplus is also the result of a new tax reform that increased the health care contributions of self-employed people with higher incomes [4].
References
[1] Law of 16 November 2022 on amending the Act – Law on the medical and dental professions and certain other laws, Ustawa z dnia 16 listopada 2022 r. o zmianie ustawy o zawodach lekarza i lekarza dentysty oraz niektórych innych ustaw (Dz.U. 2022 poz. 2770): https://isap.sejm.gov.pl/isap.nsf/DocDetails.xsp?id=WDU20220002770
[2] Rzeczpospolita, NFZ straci miliardy złotych na leczenie, 18 November 2022 [access: 26 January 2024] https://www.rp.pl/sluzba-zdrowia/art37440561-nfz-straci-miliardy-zlotych-na-leczenie-w-sejmie-przeglosowano-ustawe-pis
[3] Piotr Wójcik, NFZ zamknął 2022 rok z kilkumiliardowym zyskiem, MedExpress: 1 September 2023 [access: 26 January 2024] https://www.medexpress.pl/ochrona-zdrowia/nfz-zamknal-2022-rok-z-kilkumiliardowym-zyskiem
[4] Money.pl, Polski Ład docisnął przedsiębiorców. Kwota odprowadzonej składki zdrowotnej robi wrażenie, 20 June 2023, [access: 26 January 2024] https://www.money.pl/podatki/polski-lad-docisnal-przedsiebiorcow-kwota-odprowadzonej-skladki-zdrowotnej-robi-wrazenie-6910964818020928a.html
6.1.1. Reforms in the 2011–2015 period
The most important changes proposed and/or implemented in the 2011–2015 period are summarized in Table6.1.
Table6.1
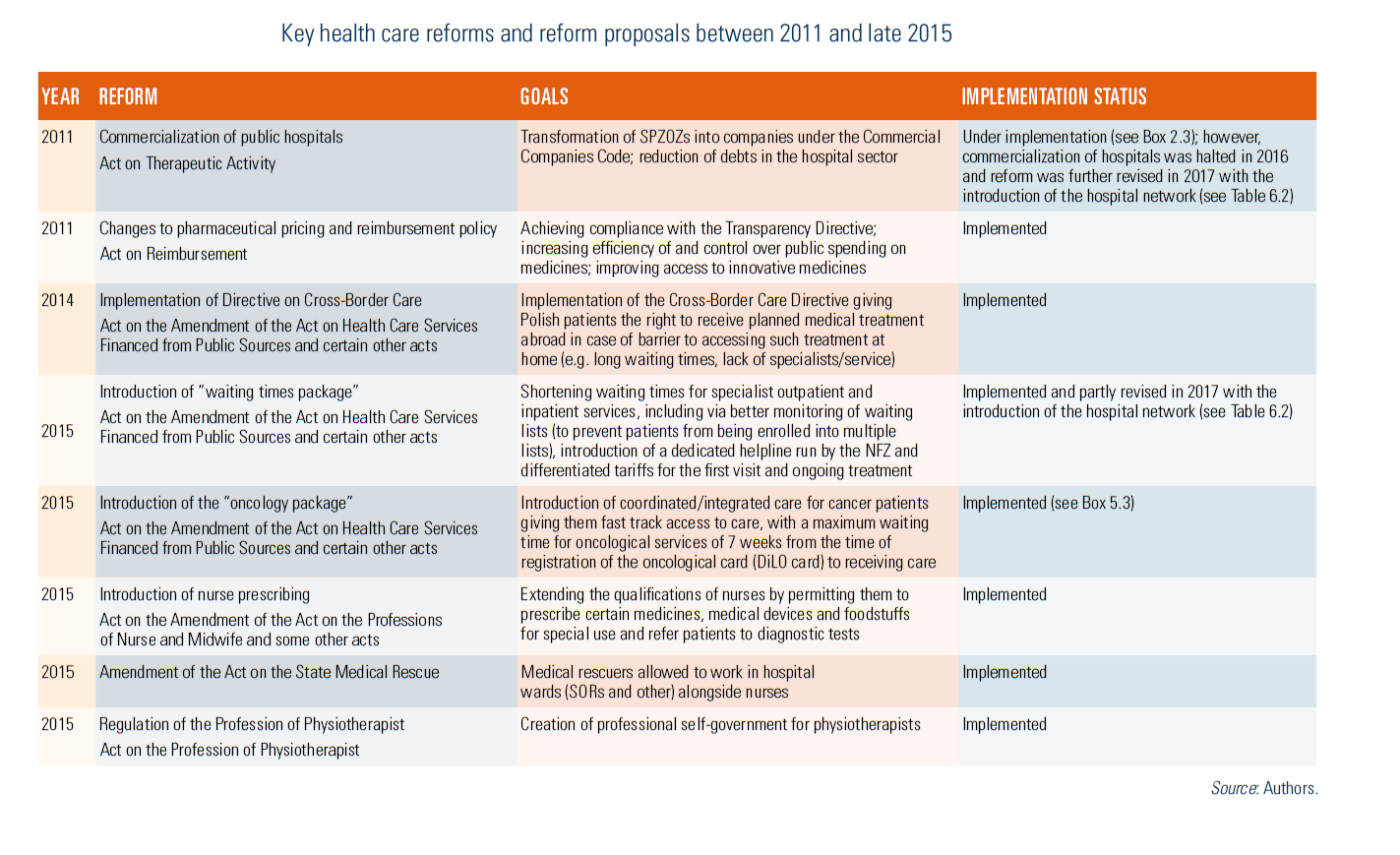
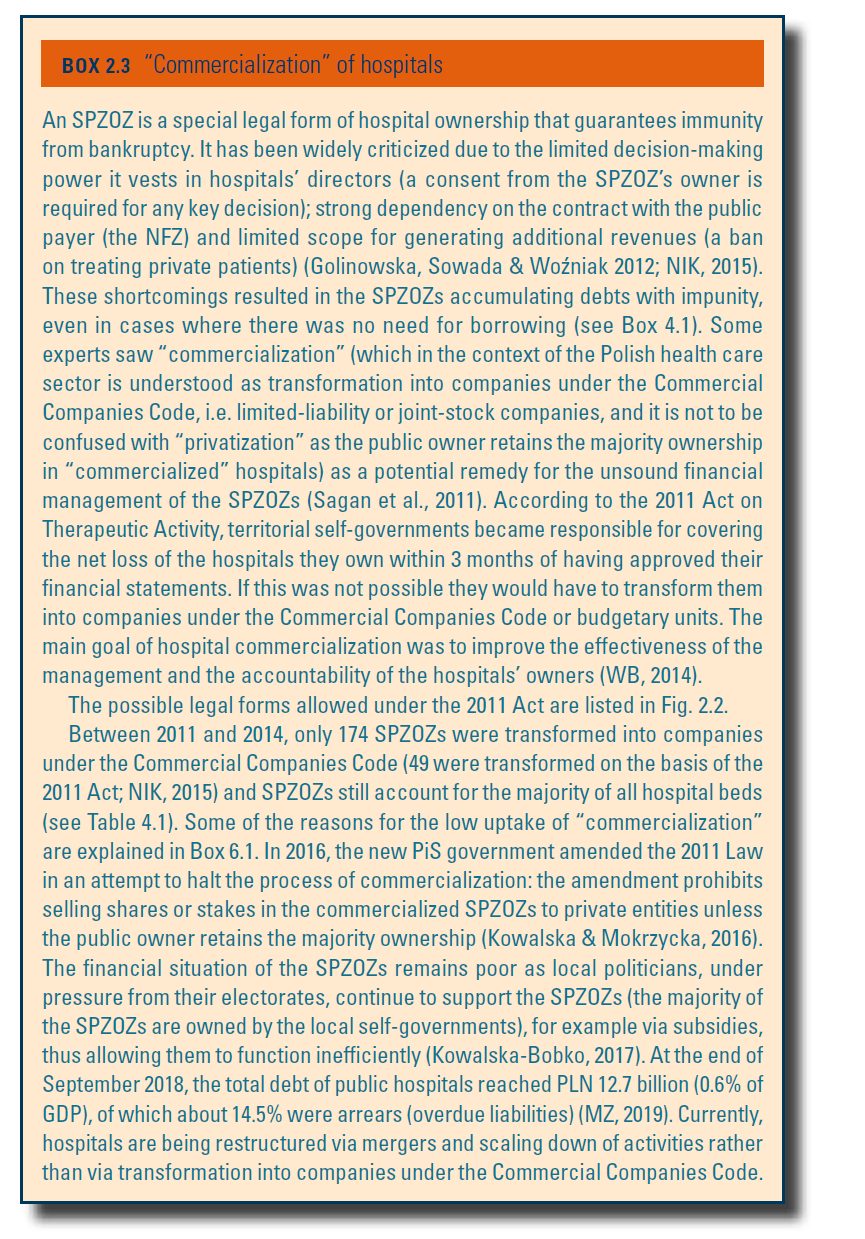
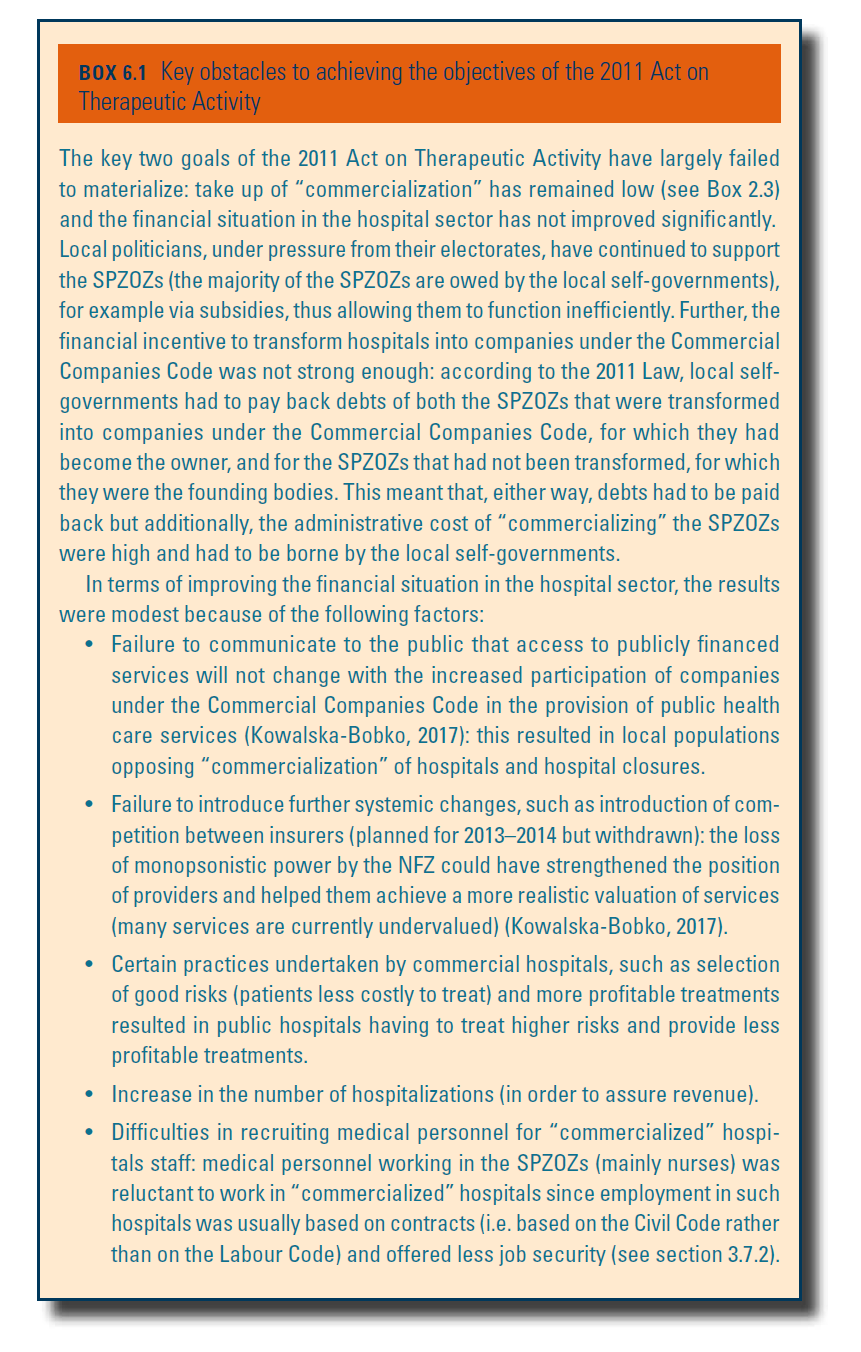
The most controversial reform in the 2011–2015 period was the transformation (known as “commercialization”) of health care providers operating as SPZOZs into companies under the Commercial Companies Code. This was initially implemented through the so-called plan B “Save Polish Hospitals” introduced in 2009 and then through the 2011 Act on Therapeutic Activity (for more information see Box2.3 and Sagan et al., 2011). It was hoped that commercialized hospitals would adopt governance principles set out in the Commercial Companies Code, such as strict control of the management board over the hospital’s finances (Kowalska-Bobko, 2017), and that this would help resolve the problem of indebtedness in the hospital sector. Overall, due to numerous obstacles (see Box6.1), the effect of this reform was limited.
Box2.3 | Box6.1 |
 |  |
6.1.2. Reform priorities since 2018
Following the elections in late 2015, the new PiS government published its reform proposals in a document titled Strategy for changes in the health care system (MZ, 2016a). The five priority areas and the specific objectives within these areas are summarized in Table6.2.
Table6.2
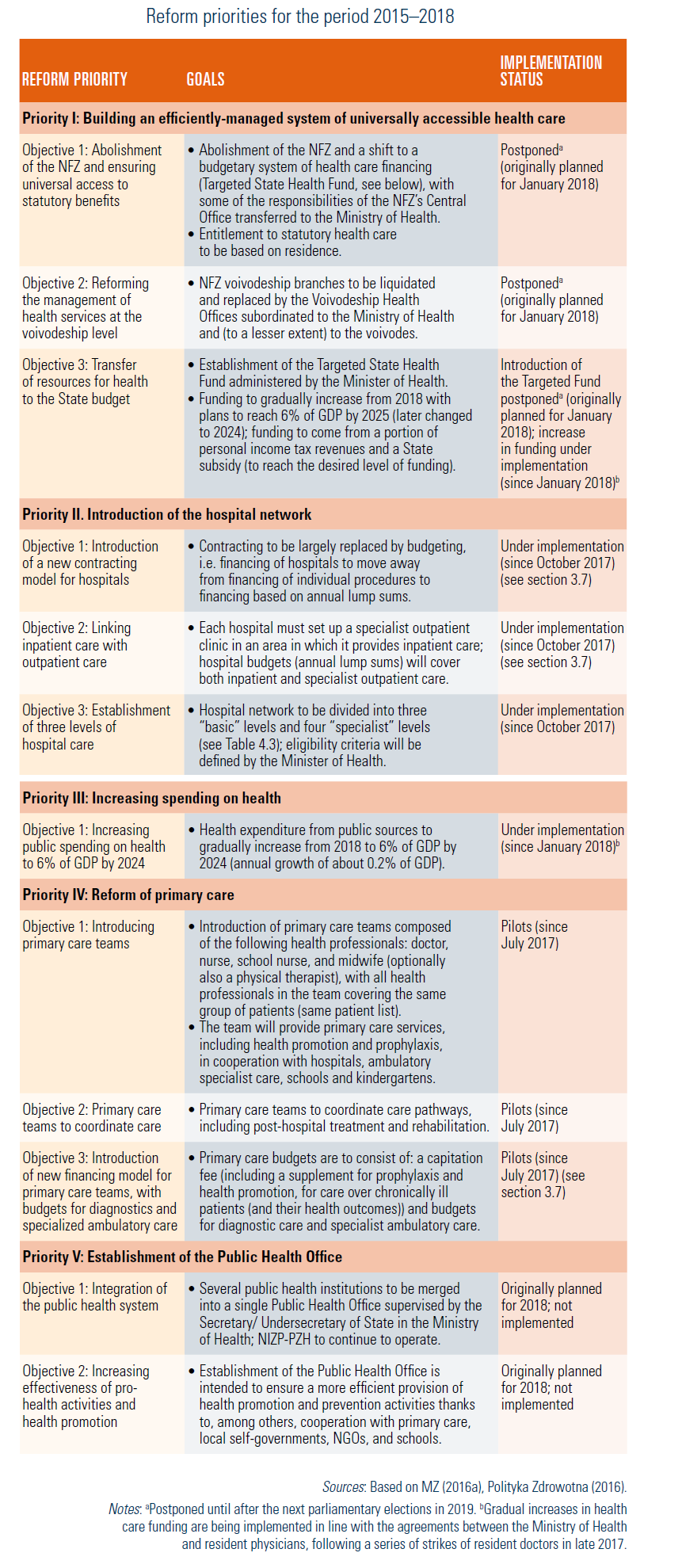
The priorities have quickly been revised as the government realized that certain proposed changes, such as the abolishment of the NFZ and transfer of contracting of services to the voivodes, were administratively difficult and could seriously destabilize the health system.
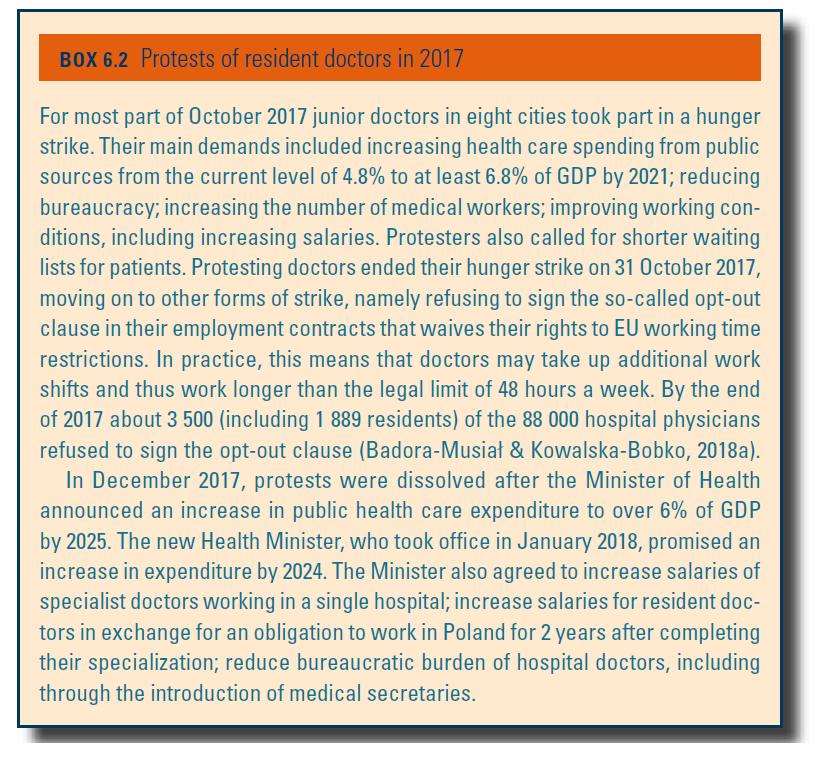
The government also had to deal with day-to-day problems such as protests of resident doctors (since late 2017; see Box6.2), mass protests related to the tightening of the abortion law (2017, 2018) as well as mass protests related to reforms outside the health sector (including reforms to the judiciary system). As a result, some of the plans have been postponed indefinitely. However, it should be stressed that two very important planned changes, i.e. creation of the hospital network and reform of primary care, have been/are being implemented. Other changes have also been introduced (see below).
Box6.2
Other key reforms introduced since late 2015 include:
- Halting of the “commercialization” of hospitals: In July 2016, the 2011 Act on Therapeutic Activity was amended. The amendment introduced a ban on selling the majority of stocks or shares in commercial companies owned by the state or local self-governments; banned capital companies with majority public ownership (at least 51%) from paying dividends; and reinforced supervisory powers of the founding entities over the SPZOZs. The amendment also allowed local self-governments to finance health care services and the SPZOZs to cover their losses from their own capital fund. If the capital fund is exhausted, the founding entity is obliged to cover the loss or may liquidate the SPZOZ. In practice, the introduced changes have made “commercialization” of SPZOZs an unattractive option for their founders and further reduced the already low rate of transformation of the SPOZOZs into companies under the Commercial Companies Code (see Box2.3).
- Introduction of the IOWISZ system for appraising investments in the health sector: In 2016, the IOWISZ system has been implemented in order to evaluate investment proposals in the health sector and thus ensure that an efficient use of resources that is cost-effective (e.g. no similar investments in the neighbouring locations) and tailored to local needs (taking into account health needs maps and local health policy priorities). Prior to the reform, there was no national system for assessing new investments in the health care sector. Under the IOWISZ system all investments that result in the creation of a new therapeutic entity or any large investment are subjected to a prior assessment. Obtaining a positive opinion within the IOWISZ system will also be a necessary condition for obtaining financing from European funds.
- Further progress in the implementation of e-health solutions: Further efforts are being undertaken to implement, by early 2020, the Electronic Platform for Collection, Analysis and Sharing of Digital Medical Records (Project P1). This platform will comprise a number of sub-platforms and applications (e.g. Internet Patient Account, various Medical Data Collection Systems) and is meant to enable public administration bodies and (Polish and EU) citizens to collect, analyse and access digital health care information, such as information on medical conditions and medical events, prescriptions, referrals, and so on. It is hoped that this will help improve, among others, quality of care, planning of services and crisis management.
- Changes in the Act on the Pharmaceutical Law: The Council of Ministers is working a major overhaul of the Pharmaceutical Law Act. The proposed key changes (to be introduced in early 2019) include: (1) strengthening the supervision over the production and marketing of medicinal products through work towards implementing Directive 2001/83/EC on the Community code relating to medicinal products for human use, for example, wholesalers of medicinal products will not be able to be involved in the provision of medical activities, in order to limit the so-called reverse distribution chain of medicines and the related illegal export of medicinal products; (2) reducing conflicts of interest in the pharmaceutical sector, i.e. persons responsible for the supervision of medicinal products who are employed at the State Pharmaceutical Inspection will not be allowed to have any financial connections with the pharmaceutical industry; (3) simplification of procedures for obtaining permission for clinical trials, i.e. applications for permissions to start clinical trials will not require a prior review by bioethics commissions or submission of certain related documentation (Kawalec & Kowalska-Bobko, 2018).
- Improving access to vaccines: In July 2018 influenza vaccines were added to the statutory reimbursement lists. They will be available with 50% reimbursement for people aged 65+. In future, reimbursement will also be granted for other recommended vaccinations. This is a big step towards improving epidemiological prevention in Poland, especially given recent anti-vaccination movements and declining rates of immunizations (see section 5.1). Until now, vaccines have not been included in the reimbursement lists, although some vaccines for children and adults have been financed directly by the Ministry of Health. Mandatory vaccination schedule for children was extended to include vaccination against pneumococci (Streptococcus pneumoniae) for all children born after 1 January 2017 (until then only certain vulnerable groups of children were covered).
- Increasing funding for health care: In August 2018, the president signed the amendment to the Act on Health Care Services Financed from Public Sources. According to this amendment, public spending on health care will account for 4.78% of GDP and 2018 and will be gradually increased to reach 6% of GDP in 2024. Salaries of resident doctors undergoing specialization will also be increased: by PLN 600 per month for specializations in non-priority areas and by PLN 700 for specializations in priority areas. Base salaries of doctors who have completed specialization training will also be increased if they commit to working in a therapeutic entity that receives public financing (for 2 years in the first 5 years after having completed the specialization training). The main objective of these changes is to increase access to health care services and improve their quality.
Box2.3