-
12 September 2025 | Country Update
Hospital Reform in Poland
2.2. Decentralization and centralization
Health system reforms since 1989 followed the very quick transition from centrally planned to market economy and changes in the administrative division of the country (see section 1.2 and Box2.1). Initial health sector reforms, introduced between 1991 and 1998, focused on the decentralization of health tasks and functions. Another goal was decentralization of the management and ownership of public health care provision to the lower levels of territorial self-government and development of private medical practice (Kowalska 2005, 2006, 2009; Kowalska & Mokrzycka, 2012; Kowalska-Bobko, 2017). Health care financing was decentralized in 1999, with the introduction of 17 largely autonomous sickness funds (see Box2.1) that replaced the tax-funded Semashko-style national health service. The lack of a unified strategy and contracting principles for the sickness funds as well as the application of different payment mechanisms for contracted services across the voivodeships resulted in considerable regional differences in access and quality of health services, potentially infringing the “equity” rule prescribed in the Constitution. Consequently, after being in existence for only three years, in 2003/2004, sickness funds were replaced by a single insurance institution – the NFZ, and the purchasing function was thus recentralized (see Sagan et al., 2011). Contracting was deconcentrated to 16 voivodeship branches. To eliminate differences in access to health care across the voivodeships, uniform contracting procedures and point limits for contracted services were introduced. Points were used to determine the value of services – each service was assigned a number of points and points had a monetary value. This structure is still in place today (although there have been proposals to abolish it; see section 6.2).
Box2.1
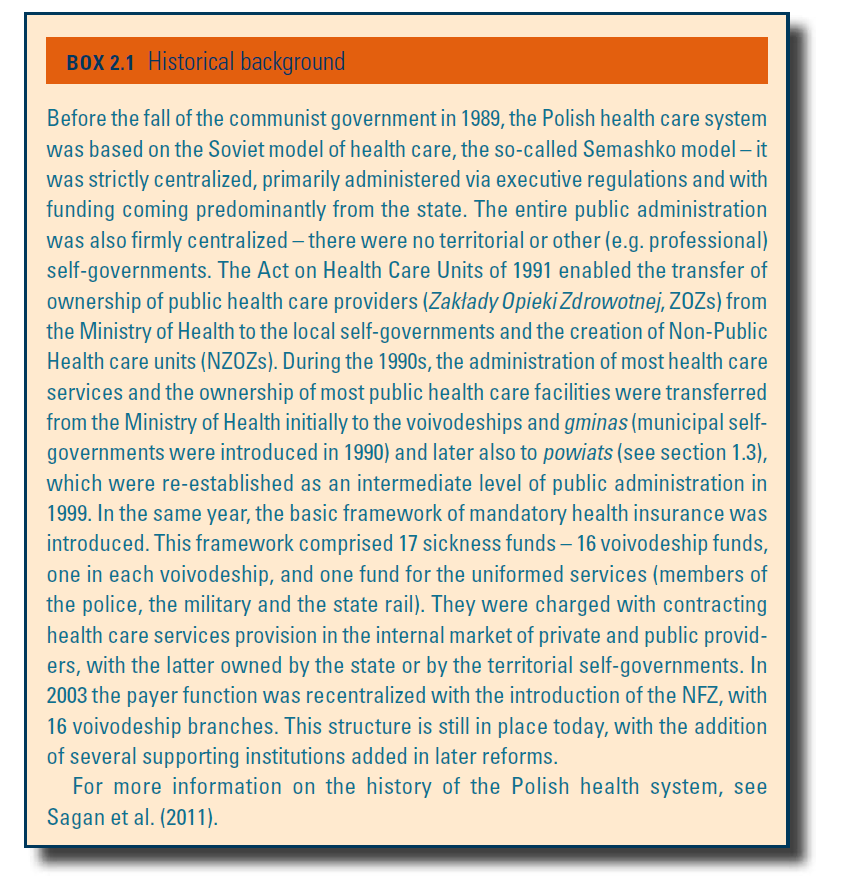
Beginning in 1991, much of the authority over public health care facilities was transferred from the Ministry of Health down to the voivodeships and, to a lesser extent, to the municipalities – they were given, among others, the right to establish health care units and were awarded ownership of public health care facilities. Counties took over responsibility for county-level hospitals. Publicly owned health facilities were given substantial autonomy and responsibility for managing their own budgets.
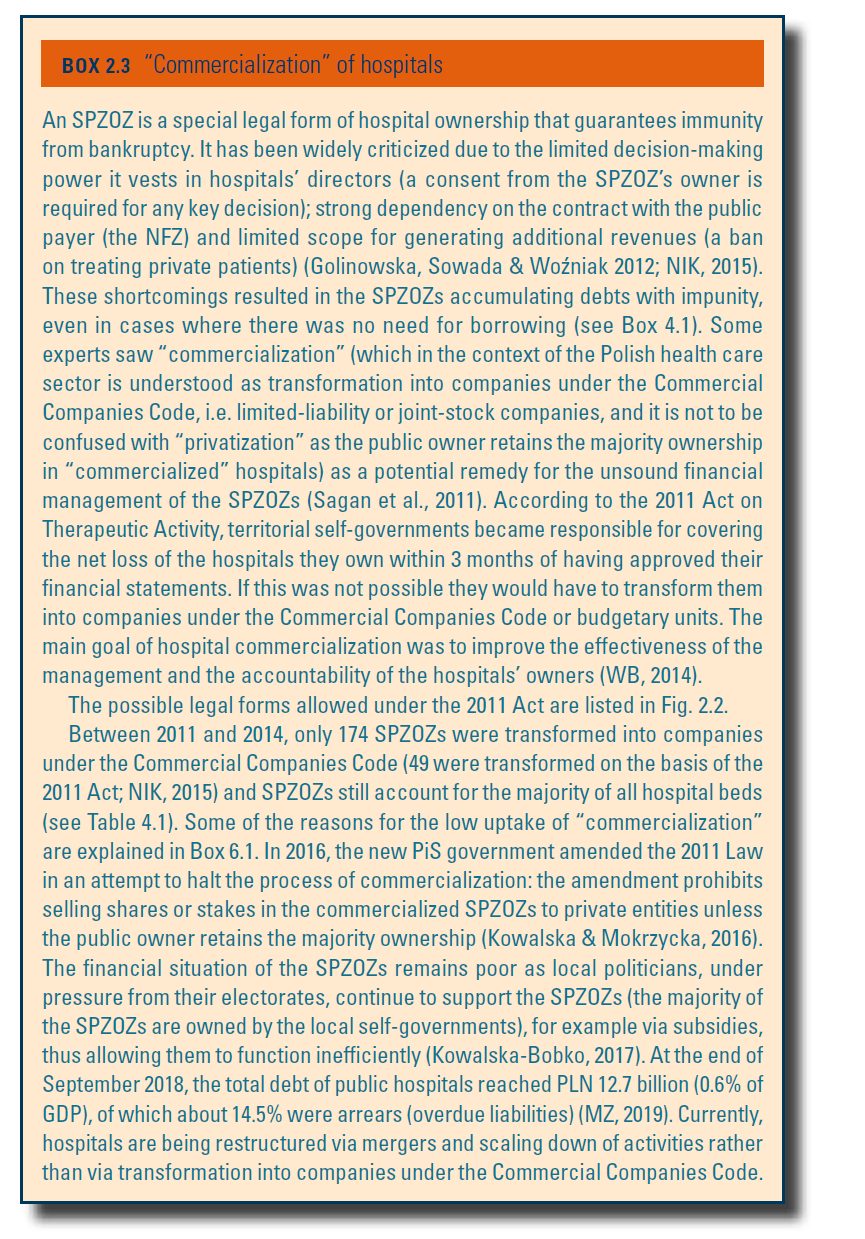
The Constitution of 1997 decentralized public power by allowing territorial self-governments to perform public tasks not exclusively reserved for public authorities at higher levels. In the area of health care, territorial self-governments are mainly responsible for health promotion and prevention (particularly in the area of occupational medicine and mental health care, as well as for alcohol and tobacco addiction and related problems) (Kowalska-Bobko, 2017). They also have responsibilities stemming from their function as the founders of public health care providers (public providers typically operate as SPZOZs; see Box2.3): they are responsible for their financial results (including for covering outstanding liabilities), and covering the costs of equipment and the maintenance of facilities. Territorial self-governments at voivodeship, county and municipal levels are also responsible for monitoring, organization and governance of health care provision at various levels of complexity: municipalities are responsible for primary health care (PHC), powiats for smaller hospitals with basic specialties and voivodeships for larger hospitals offering more complex procedures (see section 4.1). National health institutes and medical university clinics, for which the Minister of Health is the founder, provide services of the highest complexity.
Box2.3
The diversity of competences and responsibilities, and the independence of each level of territorial self-government, obstructs coordination of activities in the health system. Presently, voivodes are responsible for coordination of activities aimed at protecting the health and lives of populations in their respective territories. This includes, for example, planning of the medical rescue system and oversight over sanitary inspection in their territories. Current reform proposals postulate an increased role of the voivodeships in coordinating health care activities of the lower levels of territorial self-government (Kowalska-Bobko, 2017) and the coordinating role of a voivode in the health care system is becoming increasingly visible (e.g. in the mapping of health needs; see section 2.4).
In September 2025, a law amending the regulations on publicly funded healthcare services and medical activity, known as the hospital reform, was published. This allows network hospitals, with approval from the National Health Fund (NFZ), to transition from providing full hospitalization to offering planned, one-day or long-term care. Local governments can now establish and merge public healthcare institutions. The law also introduces a requirement to prepare recovery programmes for indebted hospitals and analyze their efficiency. The act will come into force on 17 September 2025. This reform is a key part of the National Recovery Plan, which allocates over 17 billion PLN for healthcare, including hospitals. Financial support mechanisms for indebted hospitals are currently lacking, although they are expected soon.