-
04 March 2024 | Country Update
Changes to the complaints system for compensation of treatment abroad -
09 February 2023 | Country Update
Patient choice of hospitals to no longer include private hospitals -
11 October 2022 | Policy Analysis
No decriminalization of substance abuse, but no punishment for users either -
28 August 2022 | Country Update
Prohibition of cosmetic treatment for persons under 18 years old -
31 August 2020 | Country Update
Establishment of the Ombud for Older People
2.5. Patient empowerment
There are a number of patient organizations, ranging in size and set-up. Some are mostly related to particular diseases or disease groups while others have a broader scope, for example, the Norwegian Patient Association, founded in 1983. Patient organizations are often closely linked to user committees, which are a legal entity of all RHAs and local trusts. According to Statistics Norway, almost one in 10 adults were members of an organization for patients or patients’ relatives or other health organizations in 2017 (Statistics Norway, 2019a).
From January 2023, patient choice of hospital has been limited to
public hospitals or hospitals with a tender agreement with the Regional
Health Authorities (RHAs). The previously introduced extension of the
choice of hospital, which extended patient choice to all private
hospitals and was in place between 2015 and 2022, was abandoned after an
external evaluation. The evaluation concluded that the intended goals
of the reform, such as a reduction in waiting times and higher
efficiency, have not been achieved. Challenges in terms of cost control
for hospitals and indications of increased geographical and/or social
inequality have been noted.
As an interim measure, patients under ongoing treatment in a private hospital without a tender agreement will be able to continue their treatment during 2023.
The choice of public hospital will now include not only somatic care but also mental health and substance abuse. In contrast, between 1999 and 2014, that is before patient choice was extended to private hospitals, the choice of public hospital only covered somatic care.
Authors
Decriminalization of substance abuse has been discussed since 2018
(see Reform Update from 18 April 2018) but has not been recommended by
the parliament. In April 2022, in three of its judgements the Supreme
Court decided not to punish substance abuse users for carrying minor
quantities of illegal substances for their own use. In a letter
published in May 2022, the Supreme Court set the threshold for punishing
purchase or possession of cocaine, amphetamine or heroine at 10 grams
(there was no threshold until then). New guidelines for the police
require that careful consideration is given before people are searched.
People with substance abuse problems may receive a conditional
suspension from prosecution if they agree to routine
counselling/supervision by the health services (a representative of the
local council with an expertise in substance abuse).
By
1 July 2022, all municipalities had to establish a council responsible
for ensuring that people with a substance abuse problem can obtain
advice on the support they can receive from the social system. If the
prosecuting authority decides that a person needs to undergo routine
testing for substance abuse, this can now be performed by the local
council, but this is only done in cases when this person has been
involved in an activity that is a punishable offence.
Authors
References
https://www.riksadvokaten.no/document/patalemyndighetens-legalitetskontroll-med-tvangsmiddelbruk
https://www.riksadvokaten.no/document/patalemyndighetens-legalitetskontroll-med-tvangsmiddelbruk
From 1 July 2022, persons under the age of 18 have been prohibited
from receiving cosmetic/esthetic treatment in the form of
injections/fillers, as these (among other reasons) might have adverse
effects. However, exceptions can be made for medical (including
orthodontics) reasons. This change is reflected in the amendment to the
Patients’ Rights Act. Changes have also been made to the 1999 Health
Personnel Act, according to which cosmetic injections that might be
potentially harmful can only be performed by professionally trained
health personnel.
Authors
In July 2020, the Ombud for Older People was established as an
independent national government body. Its mission is to promote the
interests of older people in all areas of society and to monitor their
situation.
Authors
2.5.1. Patient information
The availability of patient information in Norway is good and substantial improvements have been made in this area in recent years. HelseNorge (www.helsenorge.no), launched in 2011, is the main entry portal providing patient information, whether it is general advice or individual patient information (Table2.5). In addition, one of the health trusts in the Western RHA has launched a website with information about patient pathways for young people, focusing on issues such as eating disorders, anxiety problems, traumatic experiences, autism, etc.[3] There is also free public access to guidelines, systematic reviews, and a wide range of scientific journals, as well as other full-text resources, through the Norwegian Electronic Health Library (www.helsebiblioteket.no). The library also provides health care professionals and students with free access to bibliographic databases with over 3000 full text journals.
Table2.5
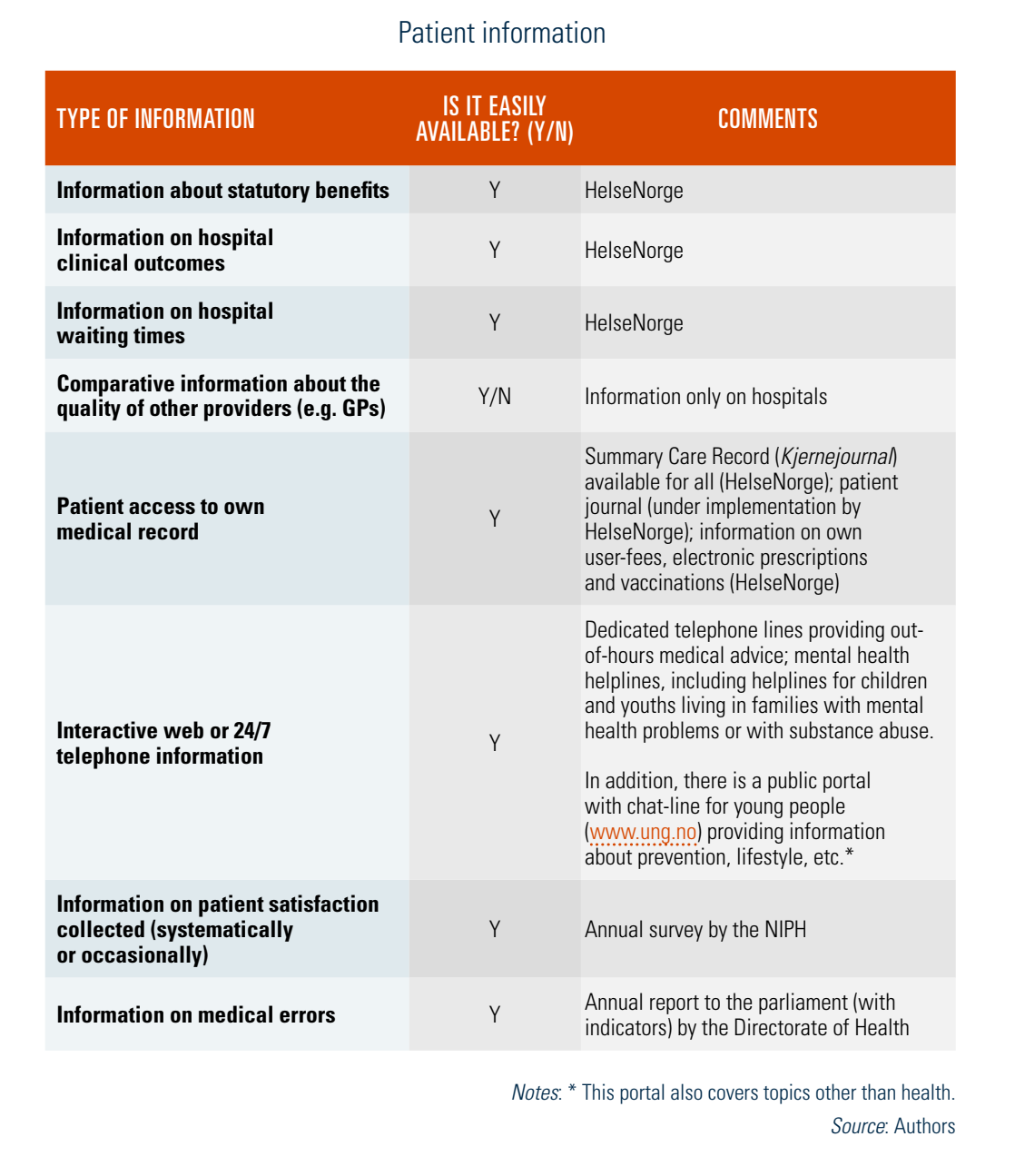
The HelseNorge portal contains information on statutory benefits and serves as a guide to health care services. Information is currently available in Norwegian and selected information is also available in English. Age-specific information is available for children and young adults. The portal provides users with access to several self-service options, for example, they can access information on their user fees, electronic prescriptions and vaccinations, out-of-hours services and hospitals, including information to assist patients with their choice of hospitals. Over 200 quality indicators to support patients in choosing hospitals are available, covering areas such as cancer treatment, childbirth and psychiatric care. This information can also be obtained via a dedicated telephone helpline (800HELSE). Patients can also access their Summary Care Record (Kjernejournal) which contains selected key information about their health that can be accessed by all health care providers (this is in addition to the medical records kept by GPs). It contains information from the national registries, information on serious medical conditions or allergies registered by the physician, and any information entered by the patients themselves and the patients’ physicians in consultation with the patients.
According to the Patients’ Rights Act (1999), patients are entitled to access their medical records and, upon request, they are also entitled to a free copy of these records plus a brief explanation of the medical terms used. This may be ordered through the HelseNorge portal. The portal has been increasingly used by patients to view their logged hospital appointments and obtain information about their personal point of contact at the hospital. The portal also contains information on prevention, health, wellness, illness, treatment and patients’ rights, with the aims of helping people take better care of their own health and encouraging more active involvement in the health system. According to a survey conducted in 2018, 76% of the respondents were aware of this portal (Norwegian Directorate of eHealth, 2019).
- 3. https://helse-fonna.no/barn-og-unges-helseteneste. ↰
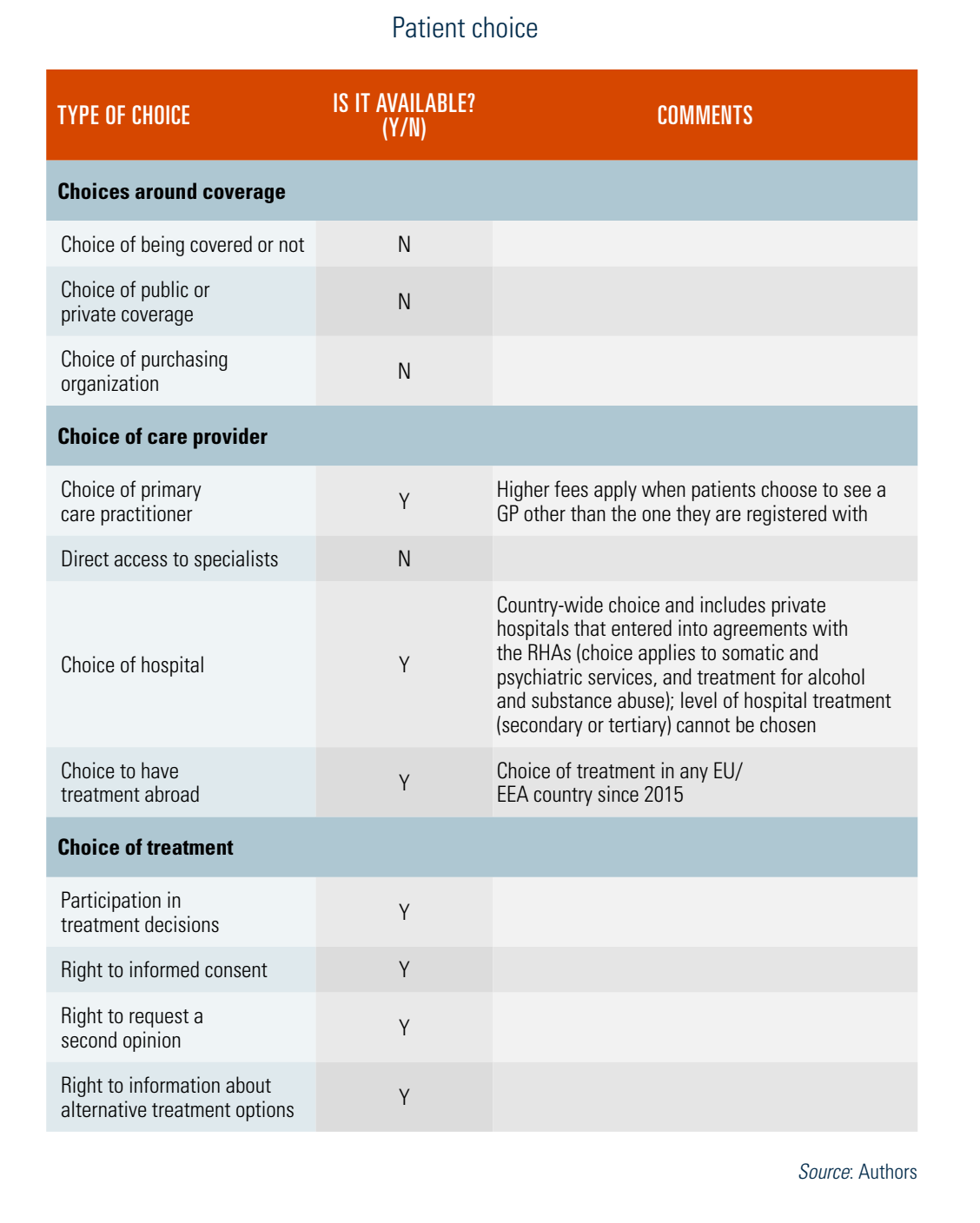
2.5.2. Patient choice
Statutory coverage in Norway is obligatory and opting out is not permitted. There is no choice of the statutory benefits package. Patients can choose their provider (GP, specialist and hospital for elective care) and participate in treatment decisions (see Table2.6).
Table2.6
Choice of provider
Patients are in general free to choose their GP. All citizens who are registered in the National Population Register are entitled to a regular GP. Switching a regular GP is possible up to twice a year, provided that the new GP has space on his or her list. Patients may choose to stay on a waiting list if no space is available. Although registration with a GP is voluntary, it covers virtually the entire population and it is strongly encouraged – patients who do not have a regular GP will be responsible for finding a GP who can give them an appointment and will also have to pay a higher fee for the service.
In order to access specialist care (i.e. privately practising specialists or hospitals), patients need a referral from their GP or from another specialist. According to the Patients’ Rights Act (1999), patients have the right to choose any hospital. Patients cannot choose the level of hospital treatment (secondary or tertiary). In November 2015 amendments to the Patients’ Rights Act came into force, changing access to elective specialist care. According to these changes, all patients in need of specialist care, regardless of the degree of need, have the right to receive such care. Access to treatment is determined according to two criteria: (1) clinical effectiveness of treatment; and (2) cost-effectiveness of treatment. The severity of the condition is only used to determine the maximum waiting time. The new legislation also required a revision of 33 discipline-specific clinical priority guidelines, which set condition-specific thresholds for obtaining access to specialist care.
User involvement in treatment decisions
According to the Patients’ Rights Act (1999), patients are entitled to participate in the decisions around their health care. This includes the right to participate in choosing between available and medically sound methods of examination and treatment. The form of participation needs to be adapted to the individual patient’s ability to give and receive information. If a patient is not competent to give consent, their next of kin is entitled to participate in decisions, together with the patient. Patients are entitled to information that is necessary to obtain an insight into their condition and treatment options, and have to be informed of possible risks and side-effects.
In 2014 important amendments to the Public Administration Act and the Electronic Public Administration Regulations were made in order to implement ICT solutions. The requirement to obtain consent from recipients before corresponding online with individuals, enterprises and others was abolished. For individuals, the requirement for consent was replaced by an option to opt out from receiving correspondence from public administration digitally.
In addition to receiving information, there is an increased focus on shared decision-making. It was included as a specific measure in the annual letter of instruction from the government to the RHAs in 2015/2016. In 2017/2018 the government requested that access to high quality decision-making aids (such as leaflets) should be made available on the HelseNorge portal (Kasper et al., 2017).
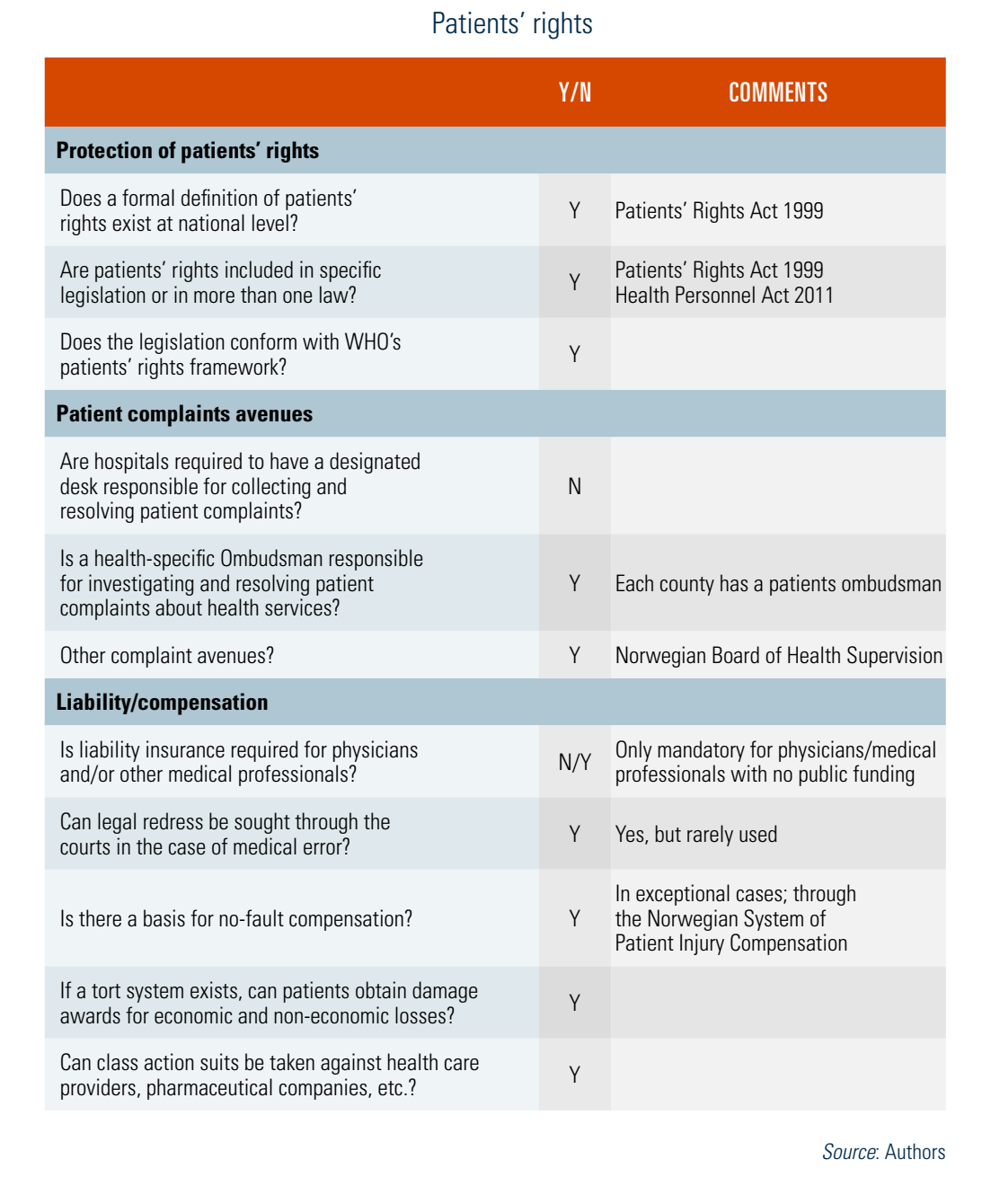
2.5.3. Patient rights
The key legal act governing patients’ rights in Norway is the Patients’ Rights Act (1999). The Act has been amended several times, further strengthening patients’ rights (Winblad & Ringard, 2009). Patients’ rights guaranteed in the Act can be divided into three main groups: rights to become a patient, rights as a patient, and procedural rights such as the right to have decisions reviewed and reversed (Table2.7).
Table2.7
In June 2017 the parliament sanctioned amendments to the Patients’ Rights Act, the Health Personnel Act and the Personal Health Data Filing System Act in order to strengthen the rights of children and adolescents as patients. Important changes concern the right to be heard as a patient, as well as the right to confidentiality and shared decision-making. Children from 7 years of age are entitled to have a say in consenting to treatment and to receive information about planned treatment; children and adolescents from 12 years of age have increasing influence on decisions regarding their treatment (Saunes & Lindahl, 2017).
Complaint procedures (mediation, claims)
Patients’ rights in Norway are well defined legal rights and can be actionable against specific parties. There are several mechanisms in place for patient complaints.
According to the Patients’ Rights Act, every county must have a POBO, whose purpose is to safeguard patients’ rights, interests and legal rights in relation to primary and specialist health care, and to improve the quality of the health service. The ombudsman can provide information, advice and guidance to anyone who requests it on matters within their remit of work. The ombudsman determines whether the request provides adequate grounds for investigation. If the ombudsman decides not to handle the case, the person who made the request must be notified and be given a brief explanation for this decision.
Patients can make a complaint if they think that they have not received health services to which they are entitled, or if they disagree with the assessment of their treatment needs. Complaints should be addressed to the person or body who took the disputed decision. If the complaint is not upheld, it will be referred to the county office of the Board of Health. Decisions made at county level can be appealed to the central office of the Board at the national level. The Board has the power to issue warnings to health personnel and to revoke licences/authorizations. The assessment by the county office does not give any automatic right to compensation or to a new course of treatment. The vast majority of complaints are brought to the county office of the Board of Health, and only a few cases are brought to the courts (Norwegian Board of Health Supervision, 2017).
The Norwegian Complaint Body for the Health Services was established in 2016. It is an independent agency and secretariat for the Norwegian System for Patient Injury Compensation (NPE) as well as other complaints within the health services. It ensures an independent assessment when patients disagree with the decisions of complaint bodies.
Compensation
The Patient Injury Act (2001) was expanded in 2009 to handle compensation claims free of charge for patients who have sustained an injury while accessing statutory health services. Since then it has also encompassed harm caused by private for-profit providers (e.g. dental care services for adults). In order to be eligible for compensation, four conditions must be fulfilled: the injury must have been caused by the treatment and, specifically, by failings in the treatment provided; it must have caused financial loss; and it must have occurred no more than three years before the claim is made. The NPE plays an active part in the handling of such cases and in establishing possible grounds for liability (they do not apportion blame but find out whether or not the patient is entitled to compensation). Decisions made by the NPE are binding for the hospital authorities and municipalities, but can be appealed by a complainant to the Norwegian Complaint Body for the Health Services or before the civil courts.
The compensation process, including the assessed compensations (by the NPE, the Board or court), is financed by contributions from both hospital owners and municipal authorities.
2.5.4. Patients and cross-border health care
Cross-border health care has not been an important issue on the policy agenda in Norway (Ringard et al., 2013). The number of hospital contacts made by foreigners is reported on an annual basis by the Norwegian Patient Register and it is very small compared to the total number of patients treated within the system (NOMESKO, 2017). Foreign patients seeking medical care in Norway must cover all treatment costs, except citizens from Nordic countries and European Health Insurance Card holders.
Since March 2015 Norwegian patients referred for specialist treatment can choose to receive it in any EU/EEA country. Treatment expenses are covered up to the cost of the equivalent treatment in Norway, while any additional treatment and travel expenses are usually not covered. The Helfo decides on the reimbursement on a case-by-case basis. Only treatments equivalent to those that the patients are entitled to at home may be covered. Patients who have had their waiting-time guarantee breached have the right to receive assistance in selecting a foreign provider and to extended cost coverage.
Norwegian citizens who are in another EU/EEA country when the need for health care arises must obtain a referral from a health care professional who is authorized to make referrals in the country of treatment. In the case of emergency care, no referral is required.
Members of the NIS are entitled to travel to a country outside the EU/EEA to give birth, but only the costs of the actual childbirth will be covered. Neither mother nor child will be entitled to coverage of further expenses outside the EU/EEA.
Members of the NIS with the right to extended subsidization (i.e. students and persons stationed abroad by their Norwegian employer) are eligible for reimbursement of a percentage of the expenses during their stay abroad. Only health care services covered by the NIS are subsidized. As a consequence, no subsidization is granted for vaccination, ordinary dentistry for children, home help service, nursing home residence, rehabilitation services, health checks and other services under the Norwegian Health and Care Services Act, Dental Health Services Act and Specialist Health Services Act.
In 2017 reimbursement for health services in another EEA country totalled NKr 63 million (€6 million). The main types of care that were reimbursed were physiotherapy and dental care and most treatments took place in Spain (Norwegian Ministry of Finance, 2018). There are no official figures on the number of Norwegians travelling abroad to receive treatment and care at their own expense.