-
10 October 2023 | Policy Analysis
New Digital Health Strategy outlines the key principles and information for the advancement of digital health in Latvia
2.1. Organization
Historical background
After regaining independence in 1991, Latvia’s attempts in the mid-1990s to transform its centrally planned health care system were characterized by the privatization of outpatient health care institutions (specifically polyclinics), which were either fully privatized or became non-profit-making state and municipal limited liability companies, and by efforts to decentralize the inherited Soviet health care system.
Most responsibilities for providing primary and secondary care were devolved to local governments (municipalities) and their local “sickness funds”. Decisions on resource allocation, payment mechanisms, service provision and closing or privatization of facilities were made by local health care boards, which were often responsible for only very small populations (i.e. less than 50 000).
Decentralization led to a lack of coordination, duplication, and gaps in service provision, inefficient investments and use of health care infrastructure and services. The number of health care facilities and beds remained high. Decentralization of health care provision affected population access to services as well as the quality of care, which became highly variable across Latvia, with richer areas enjoying better coverage and more services than the minimum service package. Inequalities in access and Latvia’s small territory and population (about 2.5 million inhabitants in the late 1990s) justified the return to the centralization of health care regulation, planning and financing.
The MoH was established in 2003 by separating health policy functions from the Ministry of Welfare. Until then, the Ministry of Welfare was the leading authority in the health sector. Local health boards were disbanded and the 35 local sickness funds were consolidated into eight regional sickness funds. Later, in 2002, the eight regional sickness funds were merged into one State Compulsory Health Insurance Agency (SCHIA). To facilitate central planning, the Development Programme for Outpatient and Inpatient Health Care Services Providers 2005–2010, the so-called “Master Plan”, was developed (Taube et al., 2015).
Primary care physicians were encouraged to work in independent practices. Hospitals became either non-profit-making state or municipal limited liability companies, later also partially subject to privatization. Almost all dental practices, pharmacies and several sanatoria (spas) were privatized.
For the financing of the health care system, the Central Account Fund was originally established in 1993 to supervise and lead the reform, and was then named the State Sickness Fund, the State Compulsory Health Insurance Agency, the State Payment Centre, before finally becoming the NHS in 2011.
Between 1997 and 2004 the compulsory health insurance revenue base was defined as an earmarked portion (28.4%) of the collected income tax revenue, plus a state subsidy financed from general tax revenue. However, this system was abandoned in 2005 in favour of general tax financing, which allowed the Ministry of Finance more flexibility in the use of public resources. The resulting “mixed” system in place in 2007/2008 was described by Tragakes et al. (2008) as “a unique combination of general tax-financed statutory health care provision, within a social insurance institutional structure”.
In response to the economic crisis and severely constrained budgets, multiple administrative reforms took place affecting the reorganization of several public institutions (see Chapter 6). The reforms in the period between 2007 and 2012 (see Chapter 6) focused on: (1) the development of a more centralized system; (2) the establishment of one central institution for purchasing health care (the NHS); and (3) a health care delivery system with a strong focus on primary care and ambulatory care (and substantially fewer hospitals). Virtually every aspect of the health care system has been affected by the ongoing process of reforms (see Chapter 6). In 2017, the mandatory social insurance contribution was increased by 1 percentage point to provide more funds for health care (see Chapter 3).
Organization
Latvia is a parliamentary republic and, consequently, the parliament and the Cabinet of Ministers issue the principal normative acts and regulations for the health sector. Health policy priorities are determined by the MoH. Fig2.1 shows the organizational chart of the health system.
Fig2.1
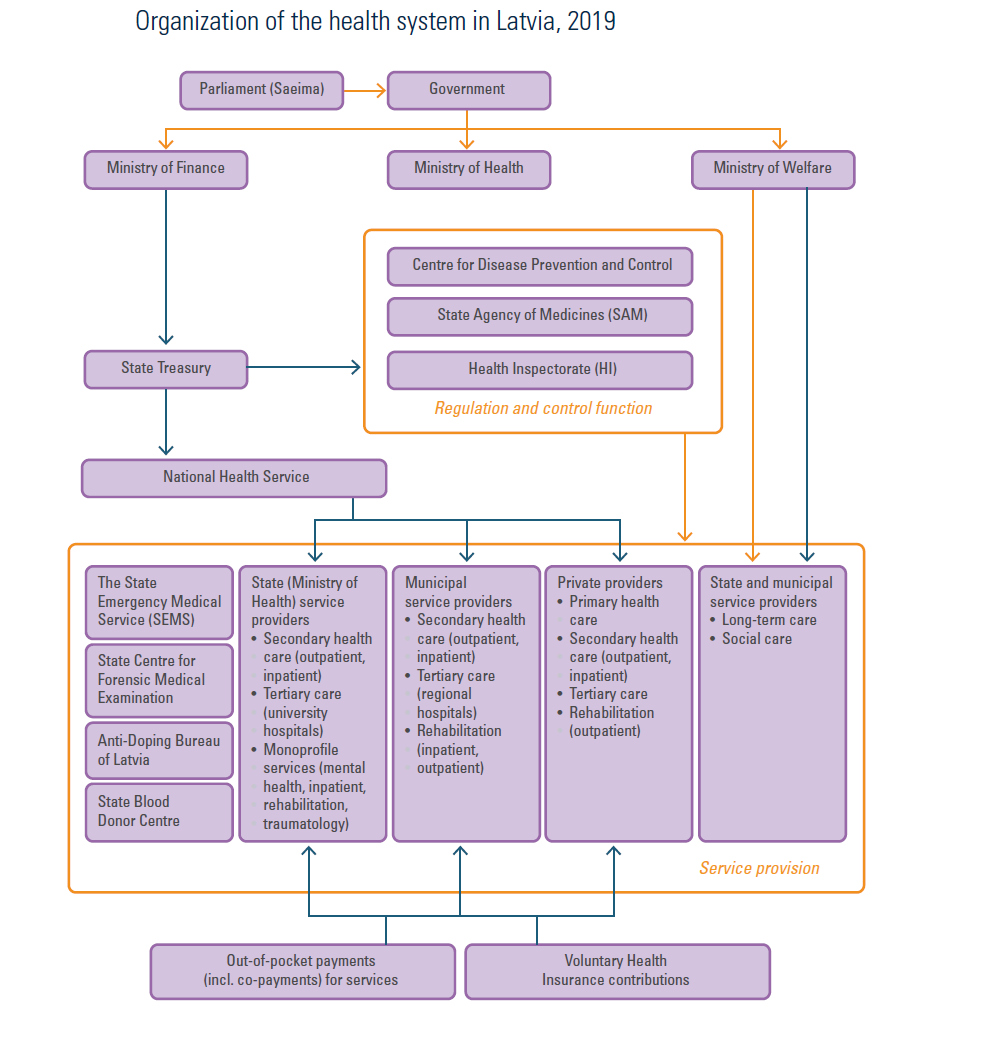
The main features of the system are:
- The central government raises resources for the statutory health care system, mainly through general taxation and a small part through social tax (see Chapter 3).
- Parliament approves the NHS budget and money is transferred from the Ministry of Finance via the State Treasury of Latvia to the NHS.
- The NHS is a state-run organization under the control of the MoH, which allocates public health care funds and contracts health care providers.
- Providers contracting with the NHS may be public or private: they tend to be predominantly private in the case of primary care; public or private in the case of secondary care, and public in the case of tertiary care, with ownership concentrated at the state (national) or municipality (regional) level.
- Social care and long-term care are predominantly under the supervision of the Ministry of Welfare and municipalities.
The most important actors in the system are the parliament, the government (Cabinet of Ministers), the MoH and the NHS.
The parliament (Saeima) has a significant role in the development of national health policy. It approves both the national budget and the budget of the NHS (see Chapter 3). The work of the parliament is organized into several committees. The Health Subcommittee within the Social and Employment Committee possesses legislative initiative and reviews all pressing health-related issues put forth by its members as well as issues brought to its attention by other members of the parliament and the MoH. Proposals to this committee can be submitted by professionals, professional associations and nongovernment organizations. The committee initiates and organizes public discussions and public debates.
The parliamentary secretary of the MoH ensures a link between the parliament and the ministry and is a representative of the Minister of Health in parliament. The MoH is the central government institution responsible for planning and regulation of the health system. It elaborates health policy, organizes and supervises its implementation. It is in charge of public health and it coordinates the health promotion and disease prevention activities of local governments. The MoH creates the preconditions for cost-effective health care and ensures accessibility and quality of services. In addition, it oversees medical education at the Rīga Stradiņš University postgraduate and professional medical education centres.
In response to the financial and economic crisis, the MoH cut administrative expenditure and employment and reorganized itself in 2009 to adjust to a smaller budget. In real terms, the direct administrative budget of the MoH in 2010 was 51% below the 2008 level. The current structure of the MoH consists of eight departments: (1) Department for European Affairs and International Cooperation; (2) Department of Document Management and Personnel; (3) Department of Public Health; (4) Department of Health Care; (5) Department of Pharmaceuticals; (6) Department of Projects Management; (7) Department of Budget Planning; and (8) Department of Investments and Monitoring of the European Union Funds. The MoH also has 10 permanent divisions: Accounting Division, Audit Division, Information Technology Division, Human Resources Development Division, Legal Division, Division of Capital Enterprises and Monitoring of Sectoral Finance and Investment, Communication Division, Procurement Division, Property and Technical Security Division and the Policy Coordination Division. In addition, there are subordinate institutions in which the MoH has a supervisory and governing role. These include the NHS, the Centre for Disease Prevention and Control (CDPC), the Health Inspectorate (HI), the State Agency of Medicines (SAM), the State Emergency Medical Service (SEMS), the State Blood Donor Centre, the State Centre for Forensic Medical Examination, the Anti-Doping Bureau of Latvia, Pauls Stradiņš Museum of Medical History and Rīga Stradiņš University.
The NHS is under the MoH and responds directly to the Minister. It is the main institution responsible for the implementation of state health policies and for ensuring the availability of health care services in the country. The institution has changed names several times in its history (see subsection Historical background within this section and Chapter 6). Today, the main tasks of the NHS include: administering public financial resources for the health sector; concluding contracts with health care providers; calculating health care tariffs; determining the positive list of pharmaceuticals; and implementing e-Health. In addition, the NHS performs the function of contact point and information centre for the cross-border health care provision, and runs the Medical Treatment Risk Fund. The CDPC registers clinical guidelines and the SAM registers medical technologies, among other functions.
The NHS consists of a Central Office and five territorial branches. The Central Office contracts directly with all hospitals for inpatient services. The territorial branches are subordinated units responsible for contracting with primary care practitioners (mostly GPs), secondary-level outpatient service providers, and pharmacies for pharmaceuticals from the positive list of approved pharmaceuticals (see section 2.4.4). However, they do not have their own budgets and pharmaceuticals are reimbursed directly by the Central Office of the NHS.
In addition to the MoH, a number of other ministries are involved in the health care system in Latvia.
- The Ministry of Finance, through the State Treasury of Latvia, ensures financial flows from the state budget to the health care system (as well as for social care services).
- The Ministry of Welfare deals with social security of Latvia, including social rehabilitation and nursing care of disabled and impaired individuals, and all other social care services, although services (e.g. for the elderly) are generally organized and provided by the local governments.
- The Ministry of Agriculture, through its Food and Veterinary Service, controls food safety.
- The Ministry of Education and Science deals with health promotion as well as several educational facilities in the health sector in Latvia, including the medical schools at the University of Latvia.
- The Ministries of Defence, Interior and Justice have their own budgets to finance health services for specific population groups (e.g. armed forces, inmates).
Local governments are responsible for ensuring geographical accessibility, and depending on budget and local priorities, they maintain hospitals and long-term social care facilities (e.g. for the elderly), and engage in promoting healthy lifestyles, controlling alcoholism and protecting vulnerable groups. Local governments are not involved in direct payments for health care services, which is the responsibility of the NHS.
The inequities between regions and local authorities in terms of both income and economic activity result in vast differences in access to health care services, especially in municipalities located far from Rīga. As a result, local governments, who are responsible for finding health professionals, raise funds to attract health care practitioners or to support the infrastructure for primary and secondary care specialists.
Inpatient and outpatient care in Latvia are provided by state and local government-owned institutions, private clinics and hospitals, and individuals (see Chapter 5). Independent of the type of property, all providers within the statutory system have to comply with regulations defined by the MoH and can be contracted by the NHS. In 2017, the hospital sector was reorganized into a five-tier hospital system, with clearly defined structures and designated responsibilities for each level.
Primary care practices run by independent GPs form the backbone of the primary health care system in Latvia. Health centres are the most important providers of secondary ambulatory care. They often operate in the premises of former polyclinics and usually employ a range of different specialists as well as GPs. About 70–80% of health centres are private (mostly in Rīga), with the remaining percentage owned by municipalities. In addition, regional (municipal) hospitals provide an important share of secondary outpatient care. Almost all dental practices and pharmacies are private. Rehabilitation is provided by general hospital care or selected institutions (see Chapter 5).
Emergency care is provided by the SEMS with emergency medical assistance (EMA) teams, and by the emergency departments of hospitals.
Mental health care is provided in both outpatient and inpatient settings. Psychiatric hospitals exist for acute and long-term treatment of psychiatric patients and patients with addiction problems. However, long-term care services are considered as social care, which is the responsibility of the Ministry of Welfare.
Since the 1990s various patient groups have been founded, for example, for psoriasis, lymphoma, diabetes etc. Most of these organizations are members of the Latvian Umbrella Body for Disability Organizations (SUSTENTO), established in 2002. SUSTENTO actively participates in the European Disability Forum. The Association of Oncology Patients “Living Tree”, founded in 2004, is the leading nongovernmental organization (NGO) in Latvia supporting oncologic patients and their relatives. The NGO Apeirons, founded in 1997, aims to integrate people with disabilities into society.
The largest medical professional organization is the Latvian Medical Association. This is an umbrella organization for more than 110 associations organized according to medical specialties, including dentists. The Latvian government delegated the function of professional certification to this organization. It is the only institution that can withdraw a doctor’s certificate, abolishing the right to practise. The nursing profession has a similar organization, the Latvian Association of Nurses. The Pharmacists’ Society of Latvia is a professional organization that represents economic and legal interests of pharmacists, and is also involved in the certification of the professional qualification of pharmacists and pharmacists’ assistants in Latvia.
A number of international organizations have a presence in Latvia (see section 3.6.2 for more details about the role of the EU and the World Bank in providing financial resources for health care). The World Health Organization (WHO) has been active in Latvia since 1991, when Latvia regained independence. WHO’s two main priorities over the years have been (1) health promotion with emphasis on control of tobacco, alcohol and drugs; cancer prevention; mental health; and promoting healthy life styles and nutrition; and (2) health system strengthening, especially with regard to public health services, primary health care, health financing and human resources for health. Other United Nations agencies also have close cooperative arrangements with Latvia. Since 1992 the following have had a presence: United Nations High Commissioner for Refugees (UNHCR), United Nations Development Programme (UNDP), United Nations Children’s Fund (UNICEF) and United Nations Educational, Scientific and Cultural Organization (UNESCO).
Health information systems
Latvia’s official statistical system, the competence of the statistical authorities, and the organization of statistical provision, including rights of data protection and access to data, are clearly defined in the Statistics Law (2016) and the Programme of Official Statistics, 2018–2020.
According to the National Information Systems Law (2002), the Ministry of Environmental Protection and Regional Development maintains the State Information System, a structured set of information technologies and databases, which provide the creation, compilation, accumulation, processing and use of information necessary for the performance of state functions. There are 20 different health sector-related state information systems, in which the information is generally available. These systems are administrated by the CDPC, the NHS, the SAM, the HI, the National Blood Donor Center and the Emergency Medical Service.
Quick and easy access to the information and services provided by state and local government institutions can be had via the official web portal (www.latvija.lv). The portal provides information on health care services contracted by the NHS, recommended actions in case of illness, reporting options for violations in health service provision, and other health system-related information. The portal also offers a range of health care e-services, which allows citizens to access their health-related information, such as basic medical data, e-prescriptions, etc., quickly and easily.
The planned e-Health portal (www.eveseliba.gov.lv), maintained by the NHS, will be the entry point, and is planned to be used by medical practitioners to record and review patient medical data, prescribe medications and issue disability certificates. Pharmacists can access patients’ prescriptions and record their dispensing at the pharmacy, and residents can now view information about their GP, provide their contact information and contact person for communication to allow other e-Health users access to their medical information, as well as view and print e-prescriptions, etc. for themselves or their dependants.
The principal institutions responsible for health data collection are the CDPC, the NHS and the Central Statistical Bureau (CSB). The CDPC is responsible for collecting and summarizing all health-related statistical data in Latvia, including data collected by the NHS and the CSB. The CDPC is also responsible for complying with international obligations by submitting data to WHO and Eurostat. All health care providers, irrespective of their ownership, have a legal obligation to prepare register cards for a number of disease-based registers kept at the CDPC branch offices, and to submit data electronically about notifiable diseases directly to the CDPC Central Office (see also section 5.1). All statistical reports consist of aggregated data and do not include personal identifiers.
The CDPC collects cause of death statistics, which are produced from data submitted by health care providers.
The NHS collects all data related to state-paid health services, processing the service provision and payment information received from all contracted providers (hospitals, health centres, GPs). The NHS data system contains information on all services provided for individual patients, including patient personal data, diagnoses (primary and secondary coded according to the International Classification of Diseases, 10th revision), procedure codes (according to a national coding system), and a provider identifier. As every patient is identified in the database with a personal ID number, it is possible to link patient data across different providers and over time, including information from other sectors (e.g. social services). However, data about non-contracted care, for which patients have to pay out of pocket, are not collected by the NHS.
The CSB collects statistical information on key health indicators, for example, the use of emergency medical services and population morbidity, and reports directly to Eurostat and OECD.
Most statistical reports, for example about health care service utilization and financing, are available for download from the NHS and the CSB free of charge. Survey results and register based statistics are available from the CDPC.
On 15 August, the Cabinet of Ministers approved the Digital Health Strategy (until 2029) prepared by the Ministry of Health. The strategy covers the period until 2029, in line with the programming period of the EU Structural Funds, which ends on 31 December 2029. This period is critical for leveraging EU funding, making it a primary source of investment for the strategy. While other healthcare development plans may include digital health measures, this strategy specifically outlines the directions and tasks for digital transformation to achieve public health policy goals for 2021–2027.
The strategy presented in this document serves as an informative report outlining key principles and information for the advancement of digital health in Latvia. It aims to create a common understanding and vision among all stakeholders, including healthcare providers and developers of digital solutions. This collaborative approach aims to improve data availability, interoperability and the development of digital services within the healthcare sector. The strategy covers several critical aspects, including its timeframe, alignment with EU structural funds and impact on public health policy.
The strategy aims to significantly reduce the circulation of “paper” medical documents, to promote the digitization of health data by medical institutions in order to process patients’ health data in a structured way, and to provide medical staff with access to patients’ digital health data created in all medical institutions, regardless of the type of service (government-funded or fee-paying). The strategy also foresees that digital solutions will enable patients to participate more actively in their healthcare, in order to implement measures to promote the use of remote solutions and other digital technologies in treatment and prevention, thus providing more accessible (also in the regions), higher quality, more efficient and more convenient health services. The strategy aims to raise awareness of digital health solutions among health professionals in order to fully exploit the opportunities offered by new technologies.
Funding for the strategy will come mainly from EU structural funds and the state budget, including funding allocated to support patient-oriented digital solutions, telemedicine and the maintenance of health information systems. EU Cohesion Policy programmes for 2021–2027 will also contribute to the funding of the strategy, along with other EU investment programmes focused on digitalization.