-
03 August 2023 | Policy Analysis
Two additional instruments to overcome sector boundaries between inpatient and outpatient care are to be introduced
5.4. Specialized care
Context
In Germany, the organization and financing of hospital and ambulatory care are separated. Several instruments were installed over the years to provide high-quality patient-centred care and to overcome the split between the two sectors. These include pre- and post-inpatient care, that is, hospital treatments without an overnight stay to prepare for or follow-up on an inpatient stay. Also, day care is typically provided in specific day care clinics, mostly covering psychiatric and geriatric care. Thirdly, hospitals can offer outpatient/day-case surgery for a limited number of treatments. For these, hospitals receive the same remuneration as office-based physicians. Despite these efforts, specialized care remains largely separated between hospital and ambulatory care.
Two further instruments are currently being installed to promote intersectoral, patient-centred care and to free up highly needed human and financial resources. The instruments are based on a recommendation from the Government Commission for a Modern and Needs-Based Hospital Sector (See Country Update of 5 November 2022) [1]. They were initiated by the Act on Nurse Staffing and other Regulations in the Hospital Sector (Krankenhauspflegeentlastungsgesetz), which passed parliament in December 2022 [2].
Reform content
Changes to the regular inpatient stay
As of February 2023, hospitals can offer certain patients admitted on an inpatient basis the possibility to leave the hospital overnight [3,4] under the following prerequisites:
- they are acceptable from a medical point of view, which is to be decided individually for each case by the hospital/attending physician;
- the inpatient treatment during the day is of at least six hours;
- the patient’s approval.
Remuneration for the new “day inpatient care” is provided via the regular Diagnosis Related Groups (DRG) system for inpatient care, but a certain amount is deducted for every night the patient stays at home, regardless of diagnosis and treatment (about €160/night). The deduction is limited to 30% of the amount the hospital would have received for a regular inpatient stay.
Equal remuneration for both hospitals and outpatient specialists for specific procedures (Hybrid DRG)
The Act on Nurse Staffing and other Regulations in the Hospital Sector also obliged the self-governing bodies to agree on a new form of cross-sectoral remuneration to be valid for both office-based ambulatory physicians and hospitals, calculated on a per-case basis (“hybrid DRG”). The new remuneration form should be limited to procedures already eligible for outpatient/day-case surgery, especially procedures with a high number of inpatient cases, short lengths of stay, and low clinical complexity [5].
Since the self-governing bodies did not reach an agreement by March 2023, it is up to the Ministry of Health to determine the exact reimbursement criteria and the list of appropriate procedures. This is expected to happen in the second half of 2023 in order to start the new remuneration at the beginning of 2024 [6].
The reforms represent further efforts to lower sector boundaries between inpatient and outpatient care. For the hybrid DRGs, the remuneration details and the number of services included will determine how well service providers will accept the new approach. The implementation of hybrid DRGs will be evaluated in April 2024, and the change to regular inpatient stays in July 2024.
Authors
5.4.1. Specialized ambulatory care
Ambulatory physicians offer almost all specialties; the most frequent ones are listed in Table5.1. Except for a few specialties, e.g. radiology or laboratory services, patients can directly access ambulatory care specialists without a referral. Between 2010 and 2020 the total number of physicians in SHI care increased by 8%. However, the strength of this trend varied according to specialty: whereas the number of GPs decreased by 1%, the number of child psychiatrists increased by 28% and the number of internists by 23%.
Table5.1
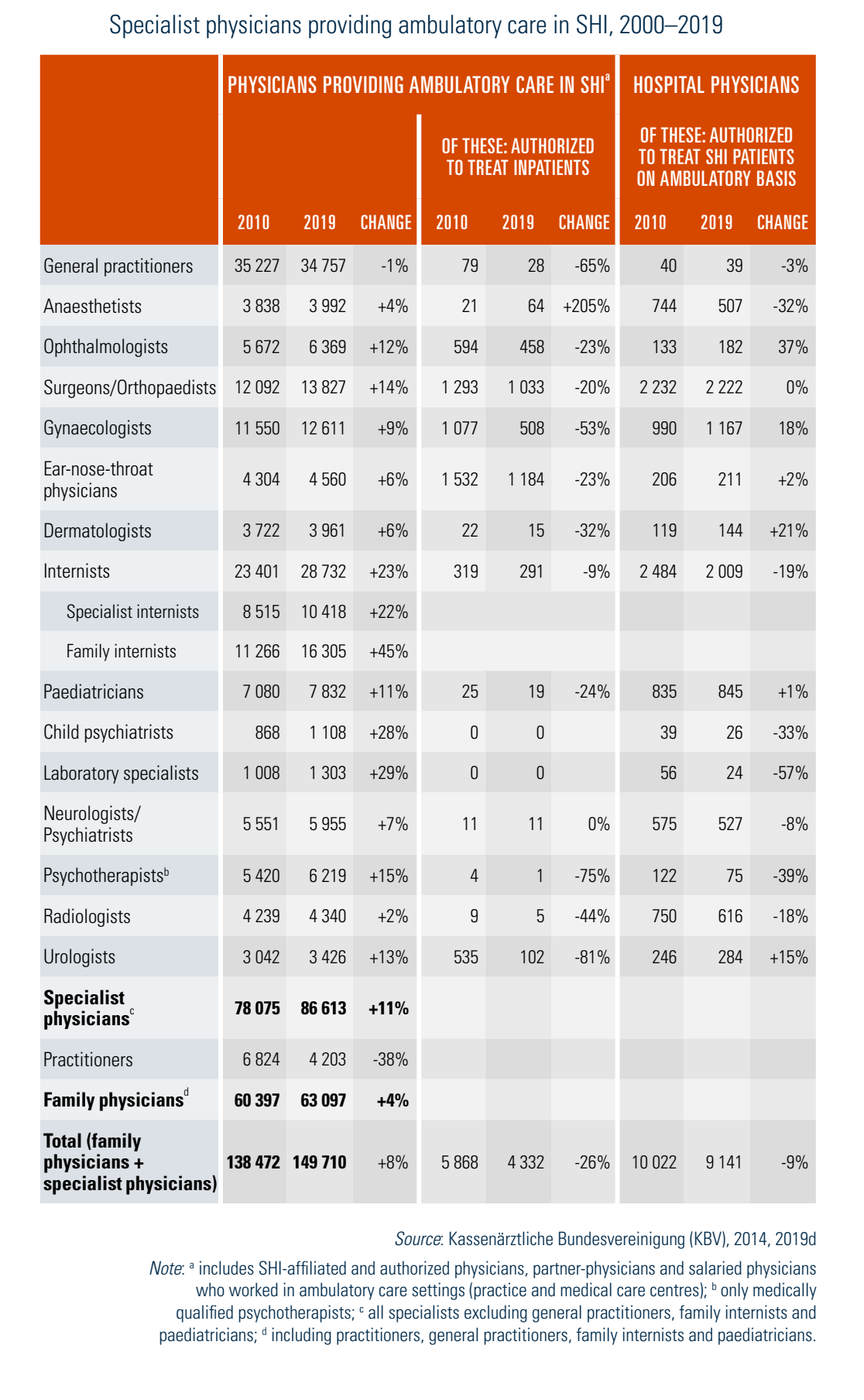
Table5.1 also provides information on two aspects linking the ambulatory and the hospital sectors. Firstly, around 2.9% of all SHI-affiliated physicians have the right to treat patients inside hospitals according to §121 SGB V. This is mainly the case for small surgical specialties in areas where the hospital has so few cases that a physician operating once or twice a week is sufficient. All other physicians transfer their patients to hospital physicians for inpatient treatment and receive them back after discharge (for example, post-surgical care is usually done by office-based physicians). Ambulatory-based specialists for ear, nose and throat medicine provided 26%, more than a quarter, of all hospital-attending physicians in 2019, followed by orthopaedic surgeons (7.5%), gynaecologists (4%) and urologists (3%). Although this form of care is a promising approach to bridging the strong sector fragmentation between ambulatory and secondary care, the share of attending SHI physicians decreased by 26% between 2010 and 2019. Secondly, in 2019 in addition to office-based physicians, around 9141 hospital physicians were accredited to treat ambulatory SHI patients. These accredited physicians are mainly heads of hospital departments who are allowed to offer certain services or to treat patients during particular times (e.g. when practices are closed). Their number has also decreased.
5.4.2. Day care
Day care is defined as medical services delivered to patients who are formally admitted to hospital for diagnosis or treatment (including pre-inpatient and post-inpatient care) with the intention of discharging the patient the same day. In 2018, 710 hospitals (37% of all hospitals) provided a total of 28 224 day-care places. About 72% of these places (20 297) were in units for psychiatry (including childhood and adolescent psychiatry and psychosomatic units), another 9% (2465) in geriatric units and 6% (1707) of places in units for internal medicine (Statistisches Bundesamt, 2020g).
Due to the strict separation between the ambulatory care and the hospital care sectors, hospital services in Germany were restricted to inpatient settings for a long time (see Box5.4). In the last 20 years the scope for hospitals to provide outpatient services has expanded significantly. Since 2004 hospitals have been able to provide care in specialties where the law (§116a SGB V) stated there was under-provision (for example, pneumology and rheumatology). Furthermore, ambulatory care for patients with certain rare diseases (e.g. tuberculosis, cystic fibrosis, Morbus Wilson) and diseases with severe progressive forms (e.g. AIDS, multiple sclerosis, oncological diseases), as well as highly specialized services (e.g. CT/MRI-aided interventional pain therapy), are areas that largely take place in hospital settings. The Strengthening Competition in SHI Act has further expanded this provision since 2007, allowing hospitals to deliver outpatient care services pursuant to §116b SGB V without prior authorization from the sickness funds insofar as the prerequisites for delivering these services are present and an application has been approved by the state government. The Federal Joint Committee regulates the details of the diseases involved, the scope of treatment and the requirements for participating hospitals. In addition, the Committee has listed criteria according to which new diseases are to be selected for hospital-based outpatient care. The SHI Care Structures Act (2011) replaced this §116b SGB V and introduced a new care sector – “highly specialized medical care provided by specialists in outpatient care” (Ambulante spezialfachärztliche Versorgung – ASV) – with the aim to promote cross-sectoral and interdisciplinary care for special complex diseases, which are difficult to treat and need special equipment. It provides a uniform legal basis for SHI-affiliated practice-based specialists in ambulatory care and hospital outpatient departments in terms of organization and financing. The Federal Joint Committee regulates the details for this highly specialized care, especially the conditions for participation of the interdisciplinary treatment teams and the necessary quality prerequisites.
Box5.4
Total expenditure for outpatient hospital care has risen continuously since 2008. In 2015 treatment for patients according to §116b SGB V (under the new definition for outpatient care) was billed for the first time. Expenditure for hospital outpatient care under the old definition and according to the ASV guideline increased from €202 million in 2015 to €247 million in 2019, corresponding to an increase of 22%. Expenditure on ASV by physicians in practice-based ambulatory care who are authorized to treat patients in hospitals rose from €1.6 million in 2015 to €22.3 million in 2019 (Bundesministerium für Gesundheit (BMG), 2020f ).
Another field of ambulatory services within the hospital sector is pre- and post-inpatient care (§115a SGB V). The share of hospitals offering pre- or post-inpatient care has increased steadily. Between 2003 and 2017 the number of cases of pre-inpatient care increased from 1.42 million to 4.7 million. During the same period the number of cases of post-inpatient care increased from 0.75 million to 1.1 million (Statistisches Bundesamt, 2018a).
Although hospitals have been allowed to offer surgery on an ambulatory or day-case basis only since 1993 (§115b SGB V), day-case surgery is not new in Germany. Due to the separation of the hospital and the ambulatory care sectors, surgeons, ophthalmologists, orthopaedic surgeons and other office-based specialists have performed minor surgery for a long time. The number of ambulatory surgeries has increased over the last decade. In 2017 almost 2 million surgeries according to §115b SGB V took place in a total of 1175 hospitals. In 2019 €0.65 billion of SHI expenditure was spent on ambulatory surgeries in hospitals and another €2.05 billion on surgeries provided by SHI-affiliated physicians in practice-based ambulatory care, which together accounts for 1.1% of SHI spending in that year (Bundesministerium für Gesundheit (BMG), 2020f ).
5.4.3. Inpatient care
Planning and regulation of treatment facilities for inpatients are carried out by ministries of health – and in the case of university hospitals, by ministries of science – at the state level, but based on the federal legal framework of the Hospital Financing Act (see sections 2.7 Regulation and 3.7.1 Paying for health services). This applies to highly specialized “tertiary” care (for example, neurosurgery) as well as regular secondary inpatient care. Planning units are institutions, departments and, in certain states, beds. The content and methods of the hospital requirement plans differ substantially among states. Regulation of capacities is planned according to the principles of need (for specific departments) and performance, but criteria differ substantially. Several states define capacities as sufficient if the departments available for one specialty in a given municipality or county had an occupancy rate of 80%. Moreover, close to 90% of the population can reach a general hospital in less than 20 minutes (Klauber et al., 2015). Hospital care, however, is not always and everywhere proportionate to need. For example, the average bed occupancy rate across the country is less than 80%. As a result, the economic situation of hospitals is in some cases critical, especially against the background of dwindling investments in hospital infrastructure by the states over the last years (see section 4.1.1 Infrastructure, capital stock and investments). Thus, in recent years several of Germany’s governments have sought advice from research institutes on how to define need and interpret hospital performance.
The Reform of Hospital Structures Act (2015) determined to strengthen the link between hospital planning and hospital payment to quality of care, with the aim of optimizing need-oriented patient care. Furthermore, additional or reduced reimbursement will be agreed for some performance areas with exceedingly high or low quality. If quality is poor, the states may formally exclude the respective hospital from hospital planning (i.e. from the state hospital requirement plan) but it is unclear to what extent this occurs in practice. For example, in a directive the Federal Joint Committee defined a total of 11 indicators relating to gynaecological surgery, obstetrics and breast surgery which are evaluated by the IQTIG annually. In 2018 there were 62 irregularities in 1063 evaluated hospitals, but without consequence regarding hospital planning (Institut für Qualität und Transparenz im Gesundheitswesen (IQTIG), 2019).
With 602 hospital beds per 100 000 population, Germany had the second highest ratio of hospital beds per inhabitant (after Bulgaria) in the EU in 2017 (Eurostat, 2020a). A fifth (18%) of all hospitals were in the state of North Rhine-Westphalia, providing almost a quarter (24%) of all hospital beds. In terms of bed density, however, most beds per 100 000 population were in the state of Bremen (761 beds), followed by Thuringia (740 beds) and Saxony-Anhalt (717 beds).
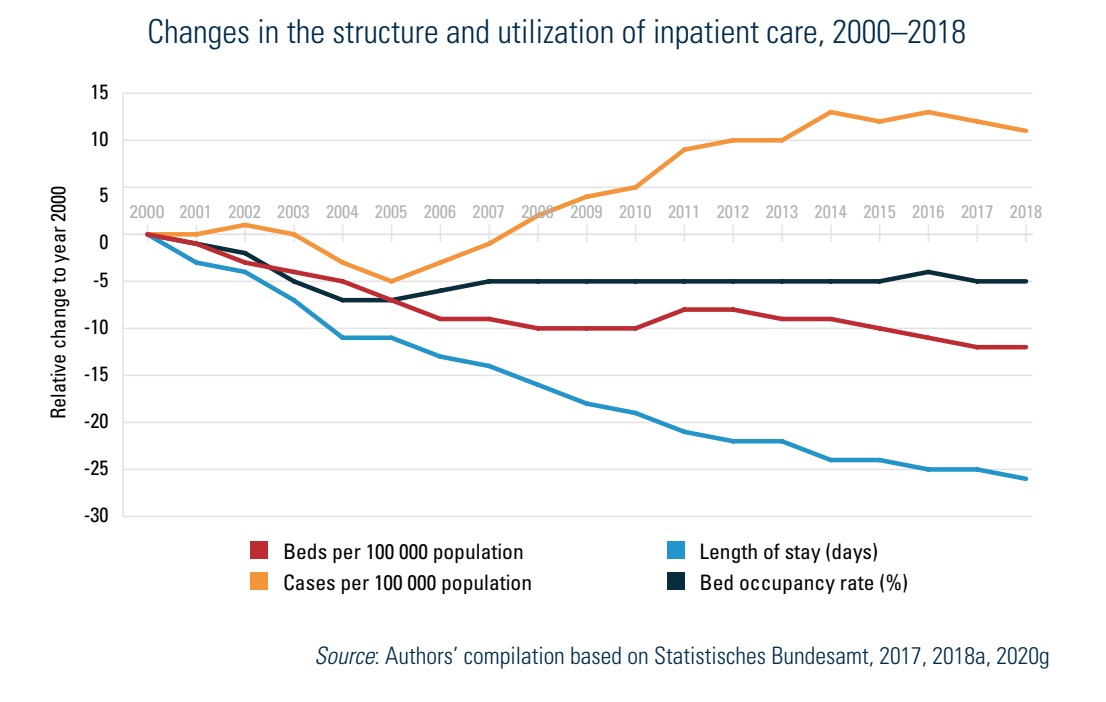
Fig5.3 shows the development of inpatient care (both structure and utilization data) for hospitals in Germany between 2000 and 2018. During this period the per capita number of general and psychiatric hospital cases rose by 14%, to 23.7 cases (admissions) per 100 population. During the same period the total number of beds decreased by 12%, from 681 beds to 601 beds per 100 000 population in 2018 (see also section 4.1.1 Infrastructure, capital stock and investment). Although the number of cases increased and the number of beds decreased, occupancy rates also decreased from 81.5% in 2000 to 77.1% in 2018. This resulted from the relatively strong decrease in the average length of stay, from 9.7 to 7.2 days. The trend of increasing admissions was pronounced in the period 2007 to 2014, while the trend of decreasing length of stay is an old phenomenon not as strongly related to the introduction of DRGs for hospital payment as is often assumed (see section 3.7 Payment mechanisms).
Fig5.3
The high density of hospitals generally ensures good availability of hospitals and access to hospital care, but with regional variations. Almost 90% of the population living in urban areas in Germany could reach the nearest acute care hospital within 15 minutes in 2016. In rural areas only 64% of the population could do so (Statistische Ämter des Bundes und der Länder, 2020). However, good availability and accessibility do not always mean high quality assurance. In general, many small hospitals provide inpatient services without adequate human resources (e.g. 24-hour availability of a range of specialists) or the technical equipment (e.g. CT scanners, intensive care units) necessary to provide high quality of care. While hospital planning still has little consideration for quality of care, in recent years Germany has introduced financial incentives for more outcome-related services (see section 3.7 Payment mechanisms).