-
11 August 2025 | Policy Analysis
The German Government introduces two new legislative bills to make the nursing profession more attractive -
10 September 2020 | Country Update
Act to reform psychotherapist education -
10 September 2020 | Policy Analysis
Act to reform psychotherapist education (analysis) -
15 January 2020 | Country Update
Act to reform midwifery education
4.2. Human resources
Context
Germany’s long-term care (LTC) system is facing increasing pressure due to demographic changes. The number of people requiring care is projected to rise from approximately 6.0 million in 2023 to around 8.2 million by 2055. At the same time, the working-age population is shrinking, raising sustainability challenges for the pay-as-you-go LTC insurance system.
In response to staffing challenges and evolving care needs, the 2017 Nursing Professions Act (Pflegeberufegesetz) made changes to nursing education. For example, it replaced the three separate three-year professional trainings for nurses with a generalist training combining the three branches of geriatric (long-term), pediatric and adult care. Additionally, a university level nursing degree (as a primary qualification) was introduced. However, training for nursing assistants remains fragmented, with 27 different programmes across the 16 federal states.
Impetus for the reforms
Projections indicate a need for 150 000 additional nursing staff by 2040. According to the Federal Ministry of Health, ensuring high-quality professional care cannot be achieved by increasing the number of registered nurses alone. A more diversified and competency-based workforce mix is required, especially one that effectively integrates nursing assistants. The reforms aim to improve care delivery, increase efficiency, reduce bureaucracy and place greater emphasis on prevention.
Main purpose
The primary objectives are to make nursing careers more attractive and to strengthen the professional nursing profile. Expanded responsibilities for qualified nurses are intended to improve chronic disease management, transitional care and prevention, especially in underserved areas, while alleviating pressure on physicians.
Key features of the reforms
The Act on Expanding Competencies and Reducing Bureaucracy in Nursing Care (Gesetz zur Befugniserweiterung und Entbürokratisierung in der Pflege) grants nurses with three-year vocational training or a university degree the authority to independently carry out selected tasks currently under the directive of physicians, such as diabetes care, wound management and dementia-related interventions. A scientifically grounded “scope of practice” will be developed to define professional nursing tasks based on competencies. The act is also intended to reduce bureaucracy, for example, by lowering documentation requirements and extending the intervals between quality assessments in nursing homes in case of positive outcomes.
The Act on Introducing a Federal Nursing Assistant Training Program (Gesetz über die Einführung einer bundeseinheitlichen Pflegefachassistenzausbildung) establishes a uniform, federally regulated 18-month training program for nursing assistants. The curriculum includes mandatory placements across inpatient long-term care, home care and acute care hospitals. Nursing assistants will be recognized as a health profession, enabling consistent, cross-sector remuneration for the training programme. Additionally, simplified recognition of foreign qualifications will rely on competency tests or adaptation courses rather than full equivalency assessments.
Implementation timeline
The Federal Government introduced both legislative proposals on 6 August 2025. The National Association of Statutory Health Insurance Physicians, the Federal Association of Health Insurance Funds, and relevant nursing associations are entering into negotiations about the scope and content of the new competencies for professional nurses and the qualifications required. According to the legislative proposals, they are expected to reach an agreement by April 2027, with the new nursing assistant training program scheduled to begin in 2027.
Authors
References
On 1 September 2020, the Act on the reform of psychotherapist
education, passed by the German parliament on 26 September 2019, came
into force.
Before 2020, a general master’s
degree in psychology and several years of further postgraduate training
had to be completed to receive a license to treat patients. Moreover,
trainees were either not paid at all or only a low amount (on average
€650 monthly in the practical year) [1].
With the Act, psychotherapy becomes a direct study subject at universities, which consists of a three-year bachelor's and two-year master's degree. Permission to practice under supervision is directly granted upon completion. However, further training is still necessary in order to be contracted for services by the statutory health insurance funds. The minimum reimbursement for full-time training after graduation is now €1000 per month [2].
Authors
References
[1] Bühring, P. Reform der Psychotherapeutenausbildung: Studienbeginn ab 2020. Dtsch Arztebl International 2019, 116, A-1762-A-1763.
[2] Federal Ministry of Health. Gesetz zur Reform der Psychotherapeutenausbildung (PsychThGAusbRefG). (https://www.bundesgesundheitsministerium.de/psychotherapeutenausbildung.html, accessed 27 January 2023).
On 1 September 2020, the Act on the reform of psychotherapist
education (Psychotherapeutenausbild-ungsreformgesetz – PsychThGAusbRefG)
came into force. After 15 years of discussion, the German parliament
passed the law on 26 September 2019. Besides the education of
psychotherapists, the reform also revises professional titles in the
field and the coordination of care for users of mental health services,
especially for people with severe mental illnesses [1]. For years there
have been problems with the coordination of mental health care, in
particular, adequately addressing the individual needs of people with
severe mental illnesses, due to, in part, a lack of coordination among
different professional groups [2].
Before 2020, a general
master’s degree in psychology and several years of further postgraduate
training had to be completed to receive a license to treat patients (in
German: Approbation). However, trainees were either not paid at all or
very low stipends (on average €650 monthly in the practical year). In
training, there was the choice to specialize in treating children or
adults and thus obtain the professional title of Child and Adolescent
Psychotherapist or Psychological Psychotherapist. In contrast,
Psychotherapists with a medical background were called Medical
Psychologists [1].
Reform content
Education
With
the Act, psychotherapy becomes a direct study subject at universities,
which consists of a three-year bachelor’s and two-year master’s degree.
Permission to practice is directly granted upon completion. However,
further training is still necessary in order to be contracted for
services by the statutory health insurance funds. The minimum
reimbursement for full-time training after graduation is now €1000 per
month[1].
Professional titles
The previous
professional titles are dropped, and the uniform title Psychotherapist
is introduced. In addition, the prefix Medical is obligatory. However,
further training is still necessary to be able to services to provide
services via the statutory health insurance funds.
Coordination of care
The
coordination of care between several professional groups in the
outpatient sector is improved under the direction of the treating
psychologists. For this purpose, psychologists are allowed to prescribe
occupational therapies and nursing care and treat their patients while
they are still in the hospital [1].
The reform as a balance of interests
The
German Medical Association (BÄK) considers that the changes introduced
by the Act will be far-reaching, going beyond training; it has expressed
concerns that the quality of care may decrease. The level of
qualification for treating patients has been noticeably lowered,
especially since psychologists can treat patients even without
comprehensive practical training. The omission of differentiated
professional titles is also viewed critically [1].
In
contrast, the Federal Chamber of Psychotherapists (BPtK) welcomes the
new law as it believes that it will lead to high-quality
psychotherapeutic care for people with mental illness in the future and
improve the financial situation of trainees. Nevertheless, the new
salary falls short of expectations [1].
The National Association of Statutory Health Insurance Funds (GKV-Spitzenverband) expects considerable additional costs, amounting to around €550 million annually, for an estimated 3000 trainees [3].
Authors
References
[1] Bühring, P. Reform der Psychotherapeutenausbildung: Studienbeginn ab 2020. Dtsch Arztebl International 2019, 116, A-1762-A-1763.
[2] Gesetzentwurf der Bundesregierung Entwurf eines Gesetzes zur Reform der Psychotherapeutenausbildung; Deutscher Bundestag, Ed., 2019.
[3] Stellungnahme des GKV-Spitzenverbandes vom 09.05.2019 zum Gesetzesentwurf für ein Gesetz zur Reform der Psychotherapeutenausbildung (Psychotherapeutenausbildungsreformgesetz – PsychThGAusbRefG); GKV-Spitzenverband, Ed., 2019.
On January 1, 2020, the Act on the reform of midwife
training, passed by the German parliament on September 26, 2019, came
into force. The Act aims to make midwifery education more attractive and
modern through academization.
Since the
reform, midwifery training consists of a three- to four-year dual
university program that combines practical training with scientific
studies. The introduction of university study and the retention of a
training allowance is expected to increase the profession’s appeal.
The
prerequisite for entering the program is 12 years of completed general
school education or completion of nursing education. The study program
is completed with a state examination as well as a bachelor’s degree.
The practical components take place in a hospital or within the
outpatient sector, that is, in a birth center or with a freelance
midwife.
Authors
References
[1] Federal Ministry of Health. Gesetz zur Reform der Hebammenausbildung (HebRefG). (https://www.bundesgesundheitsministerium.de/hebammenreformgesetz.html, accessed 25 January 2023).
4.2.1. Planning and registration of human resources
Mechanisms for planning human resources hardly exist in Germany and are only available for SHI physicians and psychotherapists in ambulatory care, and for some study programmes. Places for academic training at universities in medicine, pharmacy and dentistry are limited by individual universities. The ratio between the number of applicants and the available places is between 2:1 and 5:1 (see section 4.2.4 Training of health workers). The number of training schools and the number of training places for allied health professions are not restricted.
Under Germany’s federal structure, the states are responsible for regulating and financing education, as well as for registering and supervising health professions. The state ministries of health are responsible for the registration of health care professionals and grant licences to practise (approbation) for physicians, psychotherapists, pharmacists and dentists, and authorize the use of professional titles for the other allied health care professions. In general, the respective chambers of physicians, psychotherapists, dentists, pharmacists and nurses (the latter only available in three states) are responsible for the organization, implementation and supervision of further training activities. Re-accreditation (relicensing) is not required in any of the health professions.
Each physician has to register with the responsible state-level Chambers of Physicians as a prerequisite for a licence. These chambers represent their members’ interests in the political sphere, define uniform regulations for medical professional duties through the professional code of conduct and outline quality assurance protocols. The chambers are coordinated by an umbrella organization, the Federal Chamber of Physicians (see section 5.3 Primary care). Dentists, pharmacists and psychotherapists are organized similarly. Ambulatory care SHI physicians need to ascertain with their Regional Associations of SHI Physicians that they are undertaking appropriate professional development through further training in order to maintain their accreditation every five years. The EU standards for mutual recognition are applied to physicians, dentists, nurses, midwives and pharmacists.
4.2.2. Trends in the health workforce
Health care is an important employment sector in Germany, providing jobs for almost 5.7 million people and accounting for 12.3% of total employment at the end of 2018. Between 2000 and 2018 the number of people working in the health sector increased by a total of 1 653 000 or 41.1% (Statistisches Bundesamt, 2020f ). Of the 5.7 million people working in health, a total of 2.3 million worked in ambulatory care, 2 million in inpatient care or day surgery and 558 000 worked in health industries. Another 220 000 worked in administration, 71 000 in emergency services, 38 000 in health protection and 450 000 in other facilities. Three quarters of all health care professionals were female (75.6%), with the highest proportion of women in ambulatory nursing care (86.7%) and the lowest in emergency care (31.0%) (Statistisches Bundesamt, 2020d). Of the 5.7 million health workers, around 52% worked part-time, which corresponds to an overall workforce of 4.1 million full-time equivalents (FTEs) (Statistisches Bundesamt, 2020c, 2020d). The share of part-time employees was highest in ambulatory care facilities (71.4%) and lowest in the pharmaceutical industry (15.8%) (Statistisches Bundesamt, 2020d).
Between 2000 and 2018 most health institutions experienced strong job growth in non-physician medical practices, such as physiotherapy, occupational and speech therapy (+112%), in ambulatory care (+49%), in inpatient and day surgery facilities (+27%), in hospitals (+15%) and in the pharmaceutical industry (+65%) (Statistisches Bundesamt, 2020f ). Despite this, the Ministry of Labour reported a critical shortage of health workers in 2017, particularly for physicians, dentists, nurses, emergency care staff and midwives (Bundesministerium für Arbeit und Soziales (BMAS) 2017b). It is predicted that this shortage will increase, mainly due to rising demand for health workers to care for the ageing population and to the retirement of older health workers (Sachverständigenrat zur Begutachtung der gesamtwirtschaftlichen Entwicklung, 2018).
Fig4.3 compares the numbers of practising physicians and nurses per 100 000 population in the WHO European Region, using WHO Health for All data. Norway, Switzerland and Iceland have the largest numbers of physicians and nurses per 100 000 population. Germany, with 431 physicians and 1322 nurses per 100 000 population, is ranked sixth in western Europe.
Fig4.3
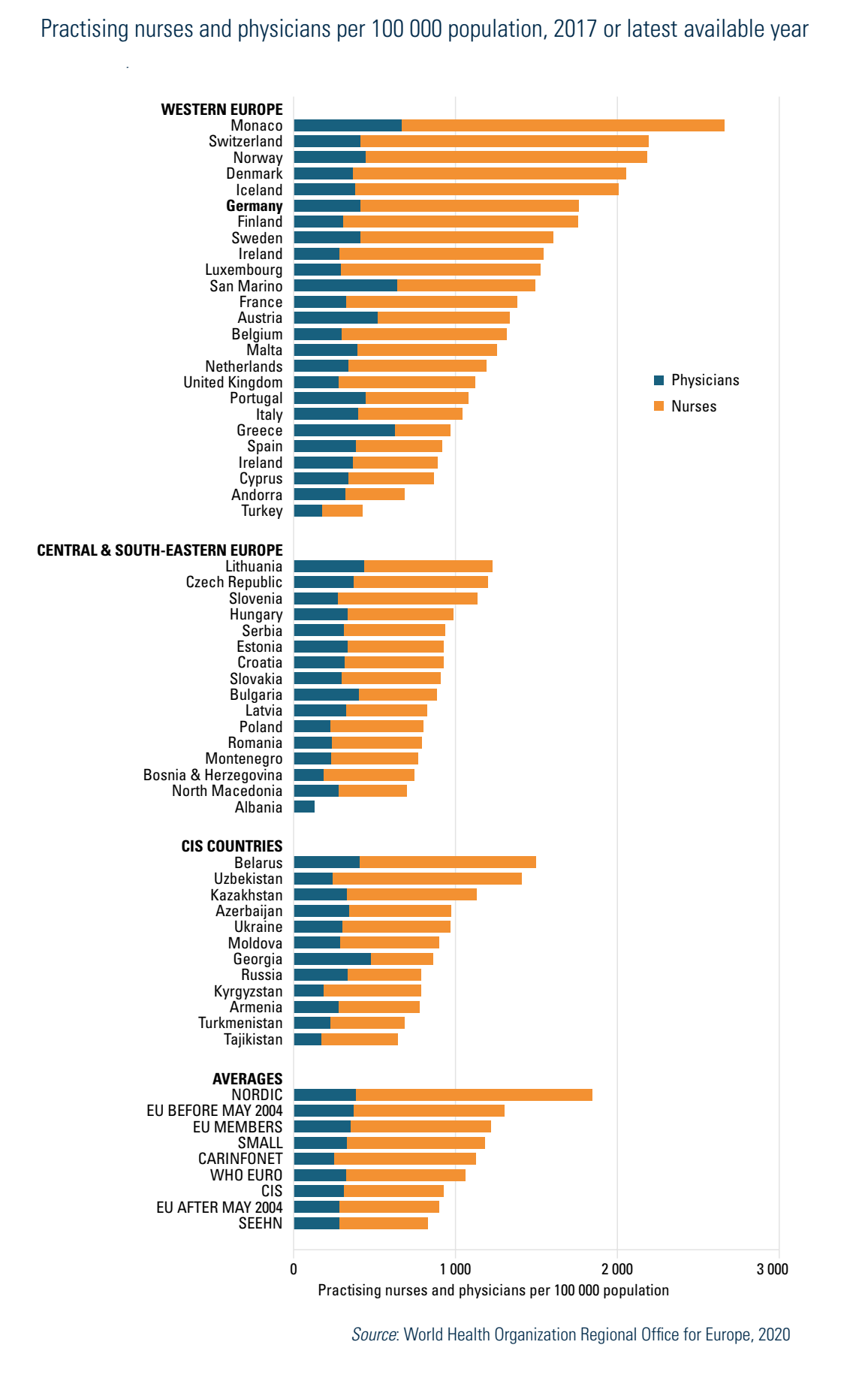
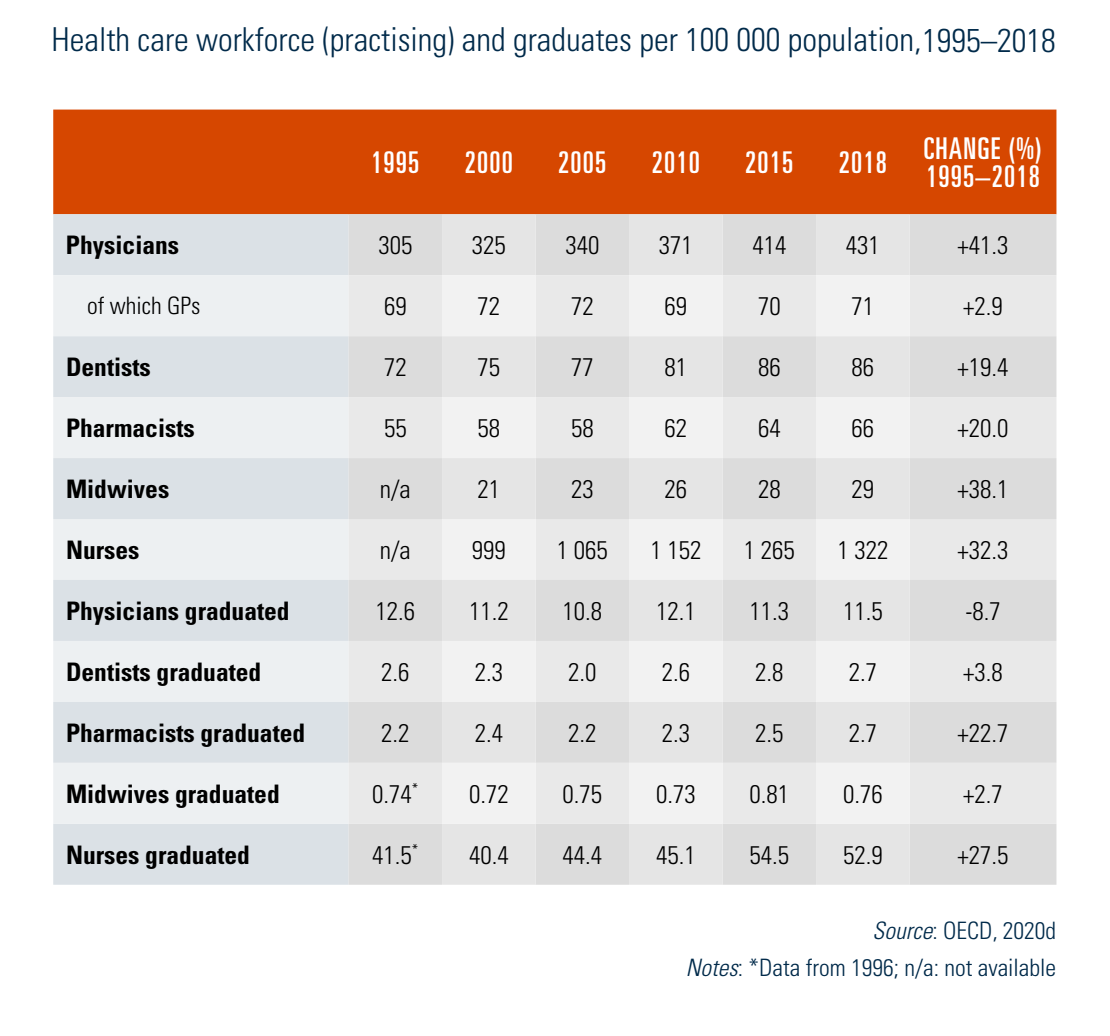
Table4.4 outlines trends in human resources and graduates in different professions since 1995.
Table4.4
Physicians
Based on data for 2018, a total of 515 640 physicians were registered with the Federal Chamber of Physicians. Of these, 392 402 were active and 123 238 retired or not active as physicians. Of all active physicians, 201 811 practised in hospitals (51%) and 157 288 in ambulatory care (40%). Another 33 303 physicians (8%) worked in the public health care sector, administration, government or other sectors (e.g. pharmaceutical industry). In 2018 there were 473 active physicians per 100 000 population, or one active physician per 211 population according to the Federal Chamber of Physicians. The distribution of physicians varies greatly within Germany (see Box4.2), from 400 practising physicians per 100 000 population in Brandenburg to 724 practising physicians per 100 000 population in Hamburg (Bundesärztekammer, 2018; GBE-Bund, (2020c).
Box4.2
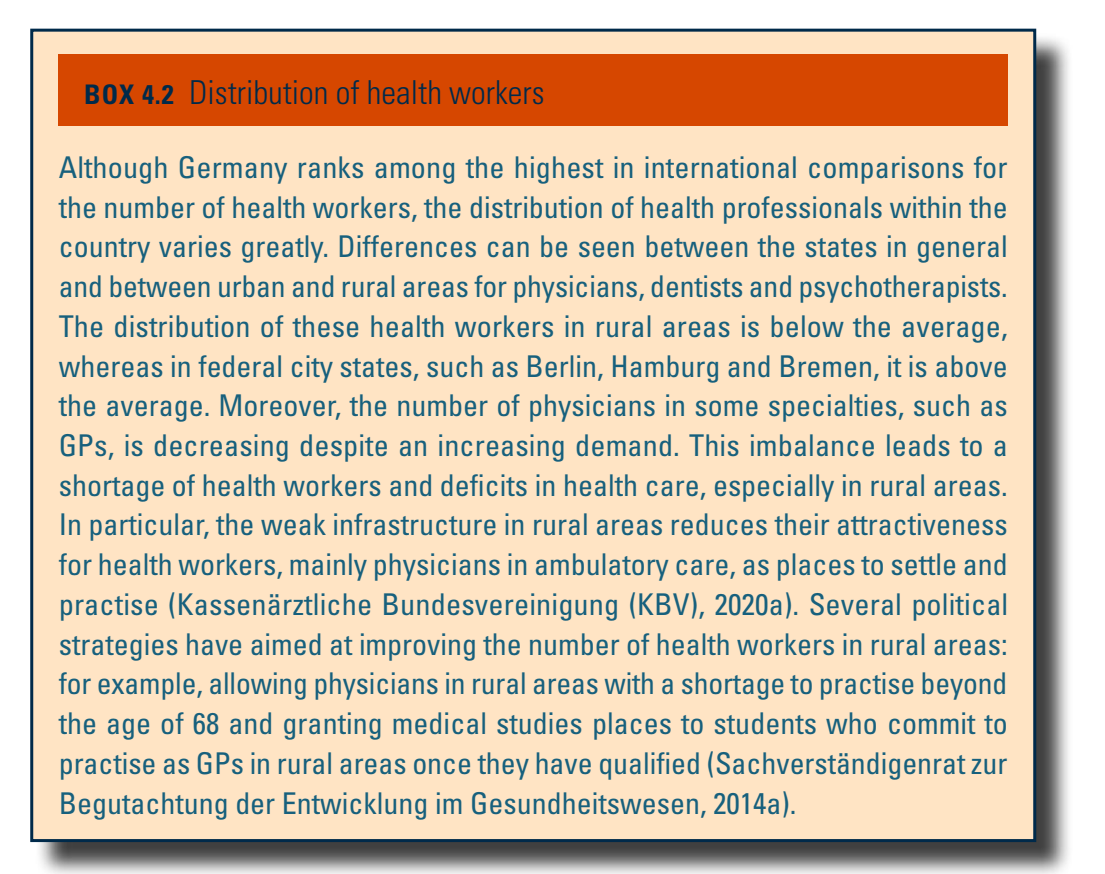
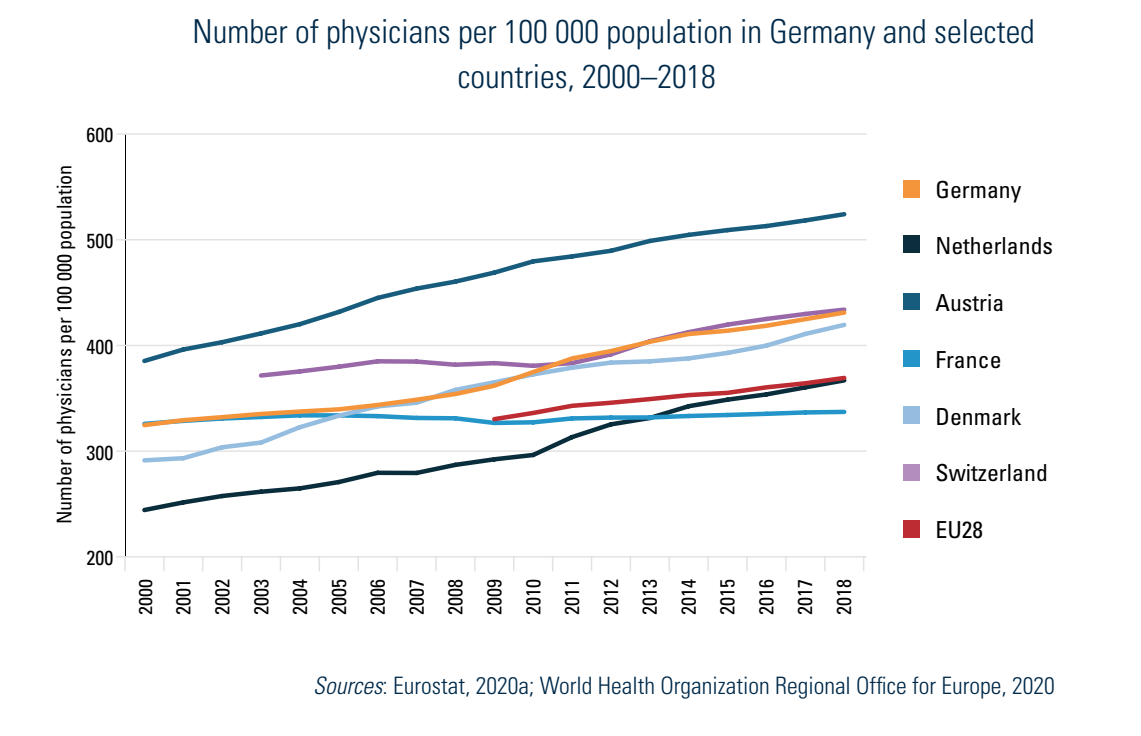
According to Eurostat data from 2018, the average of 431 practising physicians per 100 000 population in Germany[16] was above the EU28 (369 per 100 000) average. The density of physicians was below the number of 524 per 100 000 in Austria and 434 per 100 000 in Switzerland but higher than the other comparator countries featured in Fig4.4 (Eurostat, 2020b). Although the number of physicians in general has increased continuously in recent years, the number of GPs has decreased, both in relation to the population and especially in relation to all physicians, the latter from 27% in 2000 to 23% in 2017 (World Health Organization, 2020a) (see section 5.3 Primary care). Another trend highlights the growing feminization of the health sector: while in 1991 a third of the medical profession was female, in 2018, 47.2% of all practising physicians were female (Bundesärztekammer, 2018).
Fig4.4
Nurses
The number of nurses has also increased substantially, although at a slower pace than that of physicians. Between 2000 and 2018 the number of professional nurses and midwives increased by 30.5% from 721 000 to 941 000, and the number of all practising nurses (including associate nurses) and midwives by 33.7% from 838 000 to 1 120 000 (Eurostat, 2020g). Based on data from the Federal Bureau of Statistics (Statistisches Bundesamt, 2020a, 2020c), the number of nurses is significantly lower when taking FTEs as 55% of nurses and midwives are working part-time (this represents a total of 746 000 nurses (FTE)). Based on head counts, 84% of all nurses are female. In 2018 most nurses (60%) worked in hospitals and other inpatient facilities, followed by ambulatory care facilities. Some 84 000 nurses were working in nursing specialties (psychiatry, intensive care), of whom 6000 practised paediatric nursing (Statistisches Bundesamt, 2020c, 2020e).
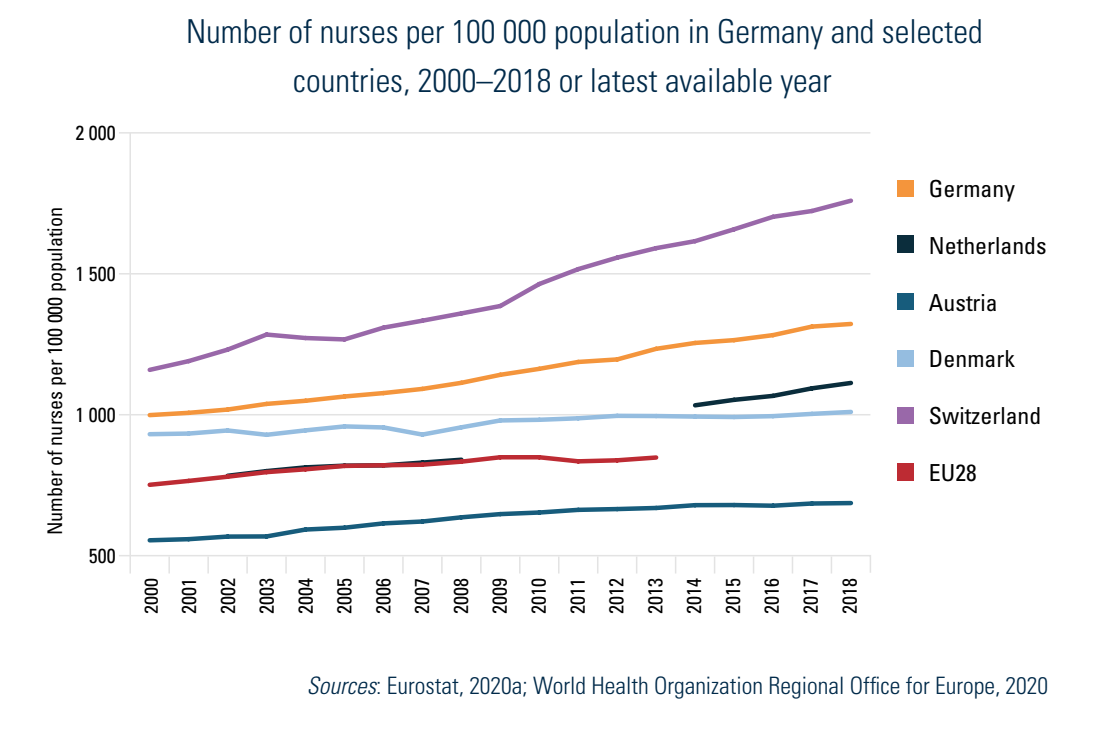
According to Eurostat data, in Germany there were 1322 practising nurses per 100 000 population in 2018, which is above the EU28 average, and the highest among the selected countries, except for Switzerland (1759 per 100 000) (Fig4.5).
Fig4.5
In order to make nursing and LTC more attractive as an occupational field, the Federal Ministry of Health, in a joint action with the Federal Ministry for Family Affairs, Senior Citizens, Women and Youth and the Federal Ministry of Labour and Social Affairs, initiated the Concerted Action for the Care Workforce (Konzertierte Aktion Pflege) in 2018, bringing together the relevant actors for long-term and hospital care. In 2019 all involved actors agreed on numerous measures to improve working and training conditions in the care sector. Five working groups adopted comprehensive measures covering training, personnel management, occupational health and safety and health promotion, innovative care approaches and digitalization, the recruitment of nursing staff from abroad and remuneration conditions in the care sector. A first status report on the implementation of these measures was published in 2020 (Bundesministerium für Gesundheit (BMG) et al., 2020). In addition, the Nursing Care Professions Act (Gesetz zur Reform der Pflegeberufe), adopted in 2017, aimed at modernizing nursing care training, including training for LTC professionals (see section 4.2.4 Training of health workers).
Midwives
Around 24 000 midwives were practising in Germany in 2018, of whom 13 000 were in ambulatory care (Statistisches Bundesamt, 2020e). In 2017 a total of 11 233 midwives (48.8% of all practising midwives) were working in hospitals (IGES Institut, 2019). The number of midwives in Germany has continually increased (by 14.3%), from 21 000 in 2012 to 24 000 in 2018 (Statistisches Bundesamt, 2020e).
Dentists
Of a total of 97 372 registered dentists, 72 592 were practising in 2018. This number represents 87.4 practising dentists per 100 000 population. The density varies from 70.4 practising dentists per 100 000 population in Saarland to 118.4 per 100 000 population in Berlin. Of the practising dentists, 46% were female and 69% were working in their own practice as self-employed dentists (Bundeszahnärztekammer & Kassenzahnärztliche Bundesvereinigung, 2020; Bundeszahnärztekammer, 2020). A total of 41 097 dentists’ practices were reported in 2018. In 2018 a total of 356 000 persons were employed in these dentists’ practices for ambulatory dental care, of whom 82.9% (295 000) were female (Statistisches Bundesamt, 2019g). In the academic year 2018/2019, a total of 12 714 persons studied dentistry, of whom 66.3% were female. In 2017, 1762 graduated from their studies (Bundeszahnärztekammer, 2020).
Pharmacists
In 2018, 52 048 pharmacists worked in 19 423 community pharmacies while another 2445 pharmacists worked in one of the 375 hospital pharmacies (Bundesvereinigung Deutscher Apothekerverbände e.V., 2019). Between 2000 and 2018 the number of pharmacists in community pharmacies increased by 13% from 46 078 to 52 048, of whom 73.0% were female, and the number of all persons employed in pharmacies increased by 16.6% from 136 470 to 159 141 (GBE-Bund, 2020d).
Allied health professionals
In 2018 there were around 240 000 physiotherapists, 64 000 occupational therapists and 30 000 speech therapists in Germany (Statistisches Bundesamt, 2020e). According to the German Association for Physiotherapy, about half of the physiotherapists (46%) were working full-time. In 2018 around 10% of the practising physiotherapists worked in hospitals, and 6% in prevention and rehabilitation facilities (Deutscher Verband für Physiotherapie (ZVK) e.V., 2020). Around 20% of physiotherapists were self-employed in 2018, of whom 39% had no employees (Statistisches Bundesamt, 2019g). In 2018, 14 of the 16 states (except for Bremen and Hamburg) reported a shortage of physiotherapists (Deutscher Verband für Physiotherapie (ZVK) e.V., 2020).
Psychotherapists
In Germany psychotherapeutic care involves medical psychotherapists (physicians) and psychotherapists (previously named “psychological psychotherapists” or “child and youth psychotherapists” (Bundesgesundheitsministerium, 2019). Psychotropic pharmaceuticals cannot be prescribed by psychotherapists. The number of psychotherapists in ambulatory care has increased in recent years, with large differences between states. In 2019 the number of medical psychotherapists ranged between 0.3 and 17.4 per 100 000 population, and the number of psychotherapists varied between 17.2 and 68.3 per 100 000 population (Kassenärztliche Bundesvereinigung (KBV), 2019b). In 2018 there were approximately 46 000 psychotherapists (including child and youth psychotherapists), most of them employed in the ambulatory care sector (34 000 or 73.9%) (Statistisches Bundesamt, 2020e).
Using available data for 2018, a total of 15 501 physicians were working in the field of medical psychotherapy, 7388 (47.7%) in ambulatory care and 6906 (44.6%) in inpatient and day care. Of the 2449 medical child and youth psychotherapists, 1202 (49%) worked in ambulatory and 1108 (45%) in inpatient care (Bundesärztekammer, 2018).
- 16. The data for practising physicians exclude the 8% of physicians working in e.g. administration and government. ↰
4.2.3. Professional mobility of health workers
The number of foreign health workers in Germany has been growing constantly since 2000. In 2018 the Federal Chamber of Physicians registered 48 672 foreign physicians practising in Germany, a 7.3% increase over the previous year (and an overall increase of 317% since 2000, when there were 11 651 foreign physicians). Of all practising physicians in 2018, foreign physicians accounted for 12.4%. Of these, 22 577 (46%) came from EU Member States, 11 559 (24%) from Asia, 9220 (19%) from other European countries, 3601 (7%) from Africa, 1240 (3%) from Central and South America, 371 (1%) from North America and 30 (0.1%) from Australia. Most foreign practising physicians came from Romania (4312), the Syrian Arab Republic (3907), Greece (2776), Austria (2309), the Russian Federation (2180) and Poland (1918) (Bundesärztekammer, 2018). The majority of foreign doctors worked in hospitals (80.1%) and only 12.2% worked in ambulatory care (GBE-Bund, 2020a). The reason for this imbalance is probably due to the higher investment costs for practice-based physicians and the strict legal framework for establishing a practice (Ognyanova & Busse, 2011).
In terms of out-mobility of doctors, 1941 physicians left Germany in 2018, of whom 56.7% were German. Of these physicians 800 (41%) migrated to EU Member States, 643 (33%) to other European countries, 147 (8%) to the Americas, 120 (6%) to Asia, 32 (2%) to Africa and 32 (2%) to Australia. Most physicians went to Switzerland (643), Austria (254), the United States (122) and the United Kingdom (59). Most German physicians migrated to the United Kingdom and Switzerland (Bundesärztekammer, 2018).
According to Microcensus data, a total of 593 000 foreign non-physician health workers were reported in Germany in 2014, accounting for 15% of all health workers. Of those, 140 000 worked as qualified nurses for the elderly and 127 000 in nursing. The share of foreign health workers among all health workers was highest in carers for the elderly (23%), dental assistants (22%) and nurses (17%). Most foreign non-physician health workers working in Germany were from Poland (100 000), Turkey (62 000), the Russian Federation (53 000), Kazakhstan (45 000) and Romania (25 000) (Kraemer, 2016).
EU mobility statistics from 2000 to 2017 show that during this period 10 622 nurses left Germany for other European countries and 3459 nurses came to Germany from European countries (Eurostat, 2020f; Verdi, 2018). The OECD reports a total annual inflow of foreign-trained nurses of 5142 in 2018 (OECD, 2020d). The main reasons for nurses leaving Germany are high workloads, poor working conditions, limited decision-making powers, lack of recognition, low remuneration, lack of collaboration between nurses and physicians, and poor advanced training opportunities (Ognyanova & Busse, 2011).
Measures in recent years have aimed at recruiting health workers from foreign countries to deal with the shortage in skilled health workers, especially nurses. These strategies have mainly been based on pilot projects, such as the Federal Ministry of Economic Affairs and Energy’s initiative to recruit young people from Viet Nam to train as nurses in Germany (Bundesministerium für Wirtschaft und Energie, 2020) or the newly founded German Agency for Nursing Professions (Fachkräfteagentur für Gesundheits- und Pflegeberufe – DeFa), in cooperation with the German Competence Centre for International Health and Care Professions (Deutsches Kompetenzzentrum für internationale Fachkräfte der Gesundheits- und Pflegeberufe – DKF). These agencies have been established by the Federal Ministry of Health and support the quick entry of international nurses into Germany and the recognition of their qualifications (Deutsche Fachkräfteagentur für Gesundheits- und Pflegeberufe (DeFa), 2020; Deutsches Kompetenzzentrum für internationale Fachkräfte in den Gesundheits- und Pflegeberufen (DKF) unter Trägerschaft des Kuratorium Deutsche Altershilfe (KDA), 2020).
4.2.4. Training of health workers
The training of health workers is a shared responsibility between the federal government, state governments and professional associations. The states are generally responsible for regulating and financing education, as well as for registering and supervising professions, including health professions. However, health professions differ from other professions because of the national regulations for their primary education and the virtual autonomy of the bodies regulating their specializations (secondary professional education) and continuing education.
National standards for curricula and examinations exist for medical studies, dentistry, pharmacy and for most allied health care professions, such as nursing, paediatric nursing, geriatric nursing, assistant nursing, midwifery, physiotherapy, occupational therapy, speech therapy, dietitian, podology, technical assistance or emergency and rescue care.
Other health care professions are either subject to the Vocational Training Act (Berufsbildungsgesetz) (e.g. medical and dental assistants, pharmaceutical commercial employees) or regulated by the Trade and Crafts Code (Handwerksordnung) (e.g. opticians, hearing aid acousticians, orthopaedic shoe technicians, dental technicians) (Bundesministerium für Gesundheit (BMG), 2020a). In addition, a large number of health care professions are regulated by state law (e.g. nurse assistant, village helper, social assistant) (Robert Bosch Stiftung GmbH, 2013).
Primary professional education and registration
Medicine, dentistry and pharmacy
Many German universities offer degrees in medicine (38 state universities and three private universities in April 2020), dentistry (29 state, one private) and/or pharmacy (22 state) (Stiftung zur Förderung der Hochschulrektorenkonferenz, 2020). Candidates require a higher education entrance qualification (Allgemeine Hochschulreife) after 12 or 13 years of school. The limited study places for these three degrees are allocated as follows for the state universities: 30% of the places are allocated according to the higher education entrance qualification grade, 10% of the places according to aptitude (defined by each university, e.g. vocational training in a health profession, success in competitions) and 60% of the places are allocated through a selection procedure conducted by the universities (Auswahlverfahren der Hochschulen – AdH) (Stiftung der Hochschulzulassung, 2020). The “Master Plan for Medical Studies 2020” has initiated changes to the structure and content of the curricula, focusing, for example, on the physician–patient relationship, ambulatory care and general medicine.
In the winter term of 2018/2019, 43 631 people applied for the 9232 places in medicine, 6190 applied for the 1518 places in dentistry, and 3980 for 1841 places in pharmacy (Stiftung für Hochschulzulassung, 2018). The duration of studies is four years for pharmacy, five years for dentistry and six years for medicine. The curricula are highly standardized by federal law and organized around three state examinations. After graduation, physicians, dentists and pharmacists receive their licence to practise (Approbation) from the state ministries responsible for health. The number of students and graduates has increased continuously since 2005 (Table4.5).
Table4.5

Nursing, therapeutic and other health care professions
Primary training of most other health professionals requires vocational technical training after secondary school, leading to qualifications/diplomas, and increasingly university degrees (see below), and usually takes three years. After graduation, health care professionals are eligible for authorization by the state authorities responsible for health to use the professional title.
The primary training of nurses currently takes place in publicly financed facilities, mostly affiliated to hospitals. Their practice-based training in inpatient facilities is combined with course-based instruction at the training facility (some days per week or in blocks throughout the week), and they receive a vocational training salary. Starting from 2020, according to the 2017 Nursing Care Professions Act (Gesetz zur Reform der Pflegeberufe), all nurses will receive joint, generalist training for two years. In their third year they can choose to specialize in the care of children (“paediatric nurse”) or the elderly (“geriatric nurse”) or to follow generalist training and acquire the qualification of professional nurse (Pflegefachfrau, Pflegefachmann). Fees for nursing training were abolished in 2020 (Deutscher Bundestag, 2018a).
Medical assistants and dental assistants are trained separately in a three-year vocational training based at training facilities and physicians’ practices, including obligatory rotation, and they receive a basic income. In contrast, schools for other health professions, such as physiotherapists, occupational therapists, dieticians and speech therapists, are often privately funded and charge fees (from about €150 to €700 per month). Some states have already abolished these fees, but the nationwide regulation to abolish all fees for health professionals’ training and to introduce a vocational training salary is still in progress (Bundesministerium für Gesundheit (BMG), 2020c, 2020o).
According to EU Directive 2013/55/EU, the training of midwives at universities is required for all Member States. The Midwifery Reform Act (Hebammenreformgesetz) entered into force in January 2020. Training takes place at universities, ending with a bachelor’s degree in midwifery. During a transitional period until 2022, midwifery vocational schools are still allowed to offer courses, which have to be completed by 2027 (Bundesministerium für Gesundheit (BMG), 2019f; Deutscher HebammenVerband e.V.).
The Psychotherapists Training Education Act regulates the training of psychotherapists from 2020 onwards and aims to improve psychotherapeutic care. Psychotherapists’ training will take place in universities (Bachelor and Master’s programmes) and will end with a licence to practise psychotherapy. Further (paid) training in inpatient and ambulatory facilities is organized according to state law which entitles psychotherapists to SHI accreditation (Bundesgesundheitsministerium, 2019).
In recent years an increasing number of undergraduate degrees have been created on the basis of a pilot from 2009 (Bundesgesetzblatt, 02.10.2009). These courses are mostly for nursing, therapeutic-rehabilitative professions, midwives and for diagnostic-technical assistant professions (Robert Bosch Stiftung GmbH, 2013). The vocational training is either fully integrated into a bachelor’s programme or interlinked and parallel, where studies continue after completion of the vocational training until the bachelor’s degree is reached. Both paths lead to a Bachelor of Science or Bachelor of Arts degree and a vocational qualification (Stöcker & Reinhart, 2012). The scheduled end of this model phase in 2017 was extended by 10 years in order to better adapt the training to university conditions and to scientifically evaluate the long-term and also financial effects of academic training (Bundesministerium für Gesundheit (BMG), 2016). In line with the Nursing Care Professions Act (2017) (Gesetz zur Reform der Pflegeberufe) undergraduate studies in nursing are no longer in the pilot phase: from 2020 onwards they constitute a three-year degree.
Secondary professional training (specialization) and continued education
Specialization usually takes two or three years for vocational health care professions and three to six years in academic professions, and another two years for a sub-specialization. Medical graduates are required to specialize if they want to work as SHI-accredited physicians in private practice, while specialization is optional for the other health care professions. German states recognize a maximum of four specialties in dentistry, nine in pharmacy, 13 in nursing and 36 in medicine, with another 79 sub-specialties or additional qualifications. Based on decisions by an assembly of physician representatives from the assemblies of the state-level chambers of physicians, the Federal Chamber of Physicians issues a model advanced training regime that is further detailed by the state-level chambers of physicians. For each of these qualifications, a minimum length of training, as well as a catalogue of procedures and skills, is detailed in the training regime. Subsequent to the advanced training period, physicians must pass an examination approved by specialists in the target qualification.
The duration of specialization in general medicine takes five years. The low number of generalists (GPs) has been interpreted as reflecting lower income prospects, a lack of training facilities in ambulatory care and lower (social) prestige attached to this specialization compared to medical doctors in secondary and tertiary hospital care. To redress this, since 2015 the Healthcare Strengthening Act (Gesetz zur Stärkung der Versorgung in der GKV) has promoted at least 7500 further training places for GPs and their salary is adjusted to that of physicians in further training in hospitals (§75a SGB V) (Kassenärztliche Bundesvereinigung (KBV), 2019c).
In 2018, of the 13 336 physicians obtaining a specialist degree, 15.4% were internists, 11.7% GPs, 9.5% anaesthesiologists, 6.6% orthopaedics, 5.1% gynaecologists and 4.8% paediatricians (Bundesärztekammer, 2018). In addition to the general “academization” of nursing that has led to the start of degree qualifications, a large number of full-time or part-time postgraduate and continuing education courses at bachelor and master level are offered in the fields of nurse education, (quality) management, nursing sciences, public health, health or therapy sciences. These are aimed at people with professional training in a health profession as well as graduates of undergraduate courses of study.
Public Health is also available in postgraduate courses of study at universities, mostly in medical faculties. Partly free of charge, partly subject to tuition fees, they are aimed at students with university degrees in both medical and nonmedical fields. The health trade professions can proceed with further training for master craftsmen (e.g. master optician). Medical and dental assistants, as well as commercial health professions, can obtain a degree as a specialist in health and social services. Medical assistants have access to 15 different specialization qualifications, including practice or care assistant (e.g. AGnES, EVA, NäPA, VERAH®), which enables them to undertake home visits, wound care, blood sugar and blood pressure monitoring, thus relieving the burden on GPs, particularly in rural areas.
Continuing education is obligatory for all health care professionals who are active in ambulatory care provided under SHI. Evidence of appropriate professional development has to be presented to the Regional Associations of SHI Physicians every five years. In the case of SHI-affiliated physicians, lack of adequate evidence may lead to a reduction of reimbursement (and even a withdrawal of the SHI-accreditation). In general, the respective chambers of physicians, psychotherapists, dentists and pharmacists are responsible for the organization, implementation and supervision of further training activities.
4.2.5. Physicians’ career paths
After graduation and obtaining the medical licence (Approbation), physicians can choose their career paths, either in hospitals or in ambulatory practice. In hospitals physicians start as assistant physicians (Assistenzarzt) during their “residency” (Facharztausbildung). This training to become a medical specialist continues for about five to six years and includes working in different specialties or units, according to the intended medical specialty. Senior physicians (Oberarzt) lead this training and have responsibility over all the assistant physicians in their wards. The chief physician (Chefarzt) is the head of the overall specialty and provides leadership, including management tasks. These designations are not legally defined, however, and therefore hospitals can determine and adjust the designations and also define prerequisites for the promotion of physicians. These decisions are made locally, mostly under the influence of the leading physicians of the clinic or department, and individually for each hospital.
In ambulatory care, directly after graduation physicians can only treat privately insured patients in their own practice. To open a practice that treats SHI-insured patients, a completed residency is mandatory. During their residency physicians are allowed to work in ambulatory care practices of SHI physicians which have been authorized as a “medical education institution”.
Physicians can already start their Medical PhD (Dr. med.) while still studying. The Doctoral Regulation (Promotionsordnung) of each university specifies the requirements regarding form, scope, submission deadlines and admission regulations for doctoral theses. In general, a doctoral degree or habilitation is not required to work as a physician. Since some hospitals (e.g. university hospitals) have internal regulations, a medical PhD can be mandatory for some senior physician positions and a habilitation for a chief physician position.
4.2.6. Other health workers’ career paths
The career paths of other health workers in Germany are less predetermined than for physicians and depend mostly on individual initiatives and are on a voluntary basis. For example, nurses can apply for a position as a senior nurse, including management tasks, or they can attend further education courses to become a specialized nurse. Another option for further training is academic studies, such as nursing management or nursing science. Dentists and pharmacists can also attend further education courses for a specialty, to become a specialist dentist (Fachzahnarzt) or expert pharmacist (Fachapotheker).