-
18 September 2025 | Policy Analysis
Evaluation process launched in three well-being services counties -
13 March 2025 | Country Update
Increasing the reimbursement for the use of private health services -
26 January 2024 | Country Update
Increased reimbursements for private services in 2024 -
31 May 2023 | Policy Analysis
Change in legislation to reduce high degree of cost sharing
3.3. Overview of the statutory financing system
The government has planned to channel €500 million to Kela reimbursements in 2023–2027 to reimburse the use of private health services. The aim is to reduce the demand for public primary healthcare in well-being services counties and in that way strengthen primary healthcare. In 2024 the government increased the reimbursements for the use of private health services. The rates for general practitioner and specialist visits rose from €8 to €30 for consultations and €25 for video consultations. The fee for a basic dental examination rose from €15.50 to €30. The fees for psychiatrists’ consultations rose to between €30 and €40, depending on the length of the consultation. The fees for psychotherapies were also increased.
Currently the government is reintroducing Kela reimbursement for infertility treatment. There is also a bill currently in the parliament that would increase the reimbursement rates for certain specialist visits (gynaecology, psychiatry) and visits to the dentist as well as introduce the possibility to have reimbursement for visits to a physiotherapist and dental hygienist without a referral. The government has also decided that it will introduce a pilot for reimbursing private general practitioner visits for those 65 years old and older. This would mean that the 65-year-old and older people would be able to visit a private general practitioner three times a year with a same user fee as in the public health centres.
So far, the evidence suggests that the increase in the reimbursements has not increased the number of users of private services, but the prices of private services seem to have increased.
Authors
References
Ministry of social affairs and health. 2024. https://stm.fi/-/hallitus-uudistaa-kela-korvauksia
The government has increased the social insurance reimbursement (Kela reimbursement) for the use of private health services for the year 2024. The Kela reimbursement rates for general practitioner and specialist visits rose from €8 to €30 for consultations and €25 for video consultations. The fee for a basic dental examination rose from €15.50 to €30. The fees for psychiatrists’ consultations rose to between €30 and €40, depending on the length of the consultation. The fees for psychotherapies were also increased.
Altogether the government has planned to channel additional €500 million to Kela reimbursements in 2023–2027. The aim of the increase in reimbursement rates is to reduce the demand for public primary health care that currently suffers from long waiting times. Over 2024 the government is planning to reform Kela reimbursement model. The aim is that the new model would come to force as of 2025.
Authors
References
3.3.1. Coverage
Breadth: who is covered?
In Finland the rights for social security and health services are based on residence. The Constitution states that the public authorities shall guarantee for everyone adequate social, health and medical services and promote the health of the population. Furthermore, everyone has the right to basic subsistence in the event of unemployment, illness and disability and during older age as well as on the birth of a child or the loss of a provider. In practice, these rights require registration with a municipality according to the Law of Municipality of Domicile, 201/1994. Residents of a municipality are considered as those who permanently live in Finland. Apart from Finnish citizens, citizens of EU countries, Norway, Iceland, Switzerland and Liechtenstein can reside in Finland. In addition, people with a permit for a permanent or continuous residence, or who have a temporary residence permit but can demonstrate the intention to live in Finland permanently, together with their family members, can be registered with a municipality. Other groups who have rights to access publicly funded health services in Finland are covered in the EU social security regulation or international agreements on social security.
Asylum seekers are not entitled to publicly financed health care or social security benefits but services for them are arranged by reception centres until they have been granted a residence permit. If an asylum and residence permit is not granted, the right to reception services stops after a certain time.
Undocumented migrants and other groups who have no health insurance coverage are entitled to obtain urgent health care from public providers. According to the Health Care Law, urgent care goes beyond emergency care and includes care for sudden illness, injury, worsening of a long-term condition or a decrease in ability to function that requires immediate assessment and treatment, as well as urgent dental, mental health, substance abuse care and psychological care. However, these individuals are responsible for covering their medical care costs. If these costs cannot be collected, Kela reimburses the provider. In addition to NGOs, municipal health authorities in some larger cities offer a limited range of health services for undocumented migrants at no charge.
Scope: what is covered?
There is no comprehensive list of health services financed from public funds in Finland. The services are considered needs-based and patients’ needs for services are assessed by health care professionals. The range of services are defined broadly in legislation, government decrees and recommendations issued by MSAH, such as the uniform criteria for access to non-emergency treatments (MSAH, 2010).
The Health Care Act (2010) specifies the range of publicly financed health services and lists the services which should be organized by municipalities. The latter include a wide range of preventive and curative services provided by health centres and hospital districts, such as screenings, maternity and child health clinics, and school, student and occupational health care services; as well as diagnostic services, somatic and dental care, mental health services, services for substance abusers, home health care and services for medical rehabilitation. Beyond this, municipalities have substantial autonomy in defining and shaping the services they provide. Therefore, there is variation across municipalities in the basic profile and scope of services provided which can be attributed to, for example, differences in their financial situation, the availability of health workers, and differences in the actual or perceived needs of the population.
Since 2011, the COHERE (see section 2.1) monitors, defines and assesses the range of services and issues recommendations on including and excluding health technologies in the range of publicly financed health services. These recommendations are gradually complementing and updating the range of services covered.
Services covered by NHI are usually reimbursed only partially and include prescribed outpatient medicines, partial reimbursement of all private health care costs (see the section below on the depth of services) and transport costs to health care units (including ambulance service). In terms of private health care reimbursement, Kela has a defined list of procedures and examinations which are included in the reimbursement scheme. It contains such services as dental care, private GP services, pregnancy and childbirth, as well as diagnostic tests, physio- and radiotherapy (Kela, 2018c).
In addition, the NHI covers medical rehabilitation for people with severe disabilities, which includes extensive or elaborate outpatient and inpatient services which go beyond curative treatment and are necessary for improving people’s functional and work capacity. Those eligible must be non-institutionalized and in receipt of disability allowance or pensioners’ care allowance (for people under 65 years of age). NHI also reimburses vocational rehabilitation for people with impaired work capacity due to illness or injury and includes basic and essential vocational training, assistance with running a business or self-employment, as well as expensive and technically advanced aids for people with severe disabilities.
Kela may, at its own discretion, reimburse vocational and medical rehabilitation services other than those described above, including services such as preventive rehabilitation measures geared towards the requirements of a particular occupation, institutional rehabilitation services, training (to adapt to a sickness or disability) and psychotherapy. NHI also covers, through Kela, rehabilitation costs in certain cases specified by the Act on Rehabilitation Benefits of the Social Insurance Institution.
The NHI scheme also compensates for loss of income during illness, pregnancy and childbirth, and for loss of income for parents caring for a sick child. Sickness allowance provides compensation for loss of earnings caused by incapacity due to illness or injury, lasting less than 12 months for people aged between 16 and 67 years. There is a nine working days’ waiting period, starting at the onset of the condition, during which the allowance is not paid. However, many collective labour agreements include a provision that the employer pays up to full salary for its employees during illness for a longer period (in some case up to three months). In these cases NHI reimburses the sickness allowance directly to the employer. Sickness allowance can be awarded even if the requirement concerning prior employment is not met and also covers students, the unemployed, and other population groups. The amount of the allowance depends on the taxable income of the recipient. In case of no income, the minimum allowance of €27.86 per day is paid.
Occupational health services organized by employers must cover health assessments when work involves health risks, provide information on those risks and advice on how to avoid them. They also include physical examinations and first aid at the workplace. In general, occupational health care is seen as preventive rather than curative. However, in addition to compulsory occupational health care, employers can voluntarily arrange additional health care services for their employees. Therefore, many employers also offer curative primary care level services. As a result, there are substantial differences in the scope of curative services offered by employers.
Depth: how much of benefit cost is covered?
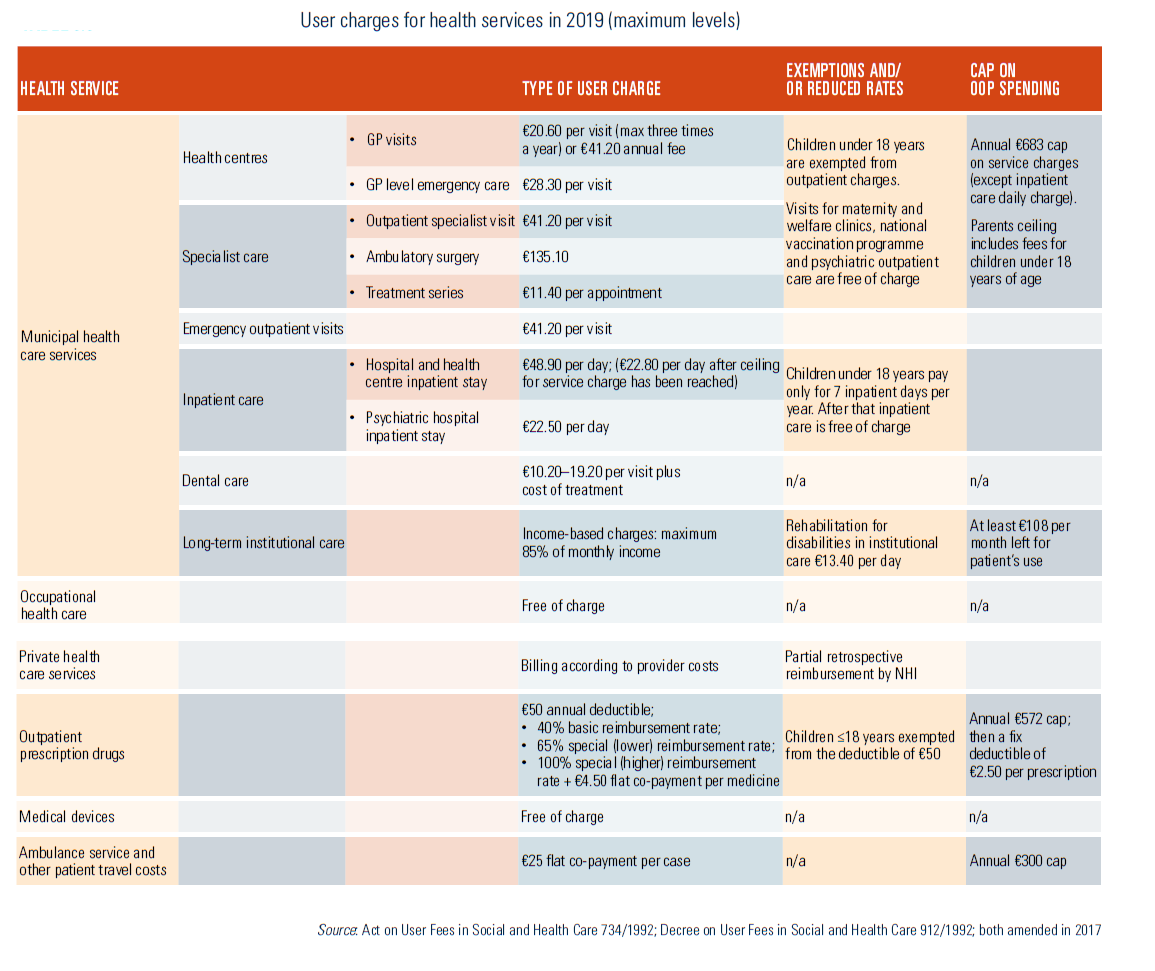
The Act on User Fees in Social and Health Care (1992, last amended in 2016) and related legislation define services provided free of charge and set limits for the maximum fees which municipalities can charge for services which involve cost sharing. While municipalities can charge less, usually they charge maximum fees (see section 3.4).
Services that are free of charge include maternity and child health clinics, immunizations included in the national vaccination programme, testing and treatment for certain communicable diseases (e.g. sexually transmitted diseases (STDs), tuberculosis, hepatitis and some others), medical aids, such as wheelchairs and other moving aids, prostheses, transportation from a health care unit to another treatment centre, and inpatient medication. In addition, appointments with a nurse and diagnostic tests are free of charge in the municipal health centres.
Health centres may charge a single or annual payment for an appointment with physicians (children under 18 are exempt), and a daily charge for up to seven days of treatment on an inpatient ward of a health centre. Hospitals usually charge for outpatient services, a daily hospital fee for inpatient care, and fees for series of treatments and rehabilitation. Fees for care provided at home depend on whether the service is occasional (paid per visit) or long-term (paid monthly). A monthly fee is incurred for continuous treatment, whereas fees for occasional treatments by physicians or dentists are charged per visit.
In the private sector, patients pay full fees, but may claim partial reimbursement from the NHI. Private health care providers who have an agreement with Kela can charge the reimbursed proportion from the NHI directly. Fees for private services (both outpatient and inpatient care) are reimbursed by the NHI according to reference rates defined by the Government for every individual procedure. Since 2013 the rates are given as euros per procedure (and were specified as a share before 2013). Reimbursement covered on average 16% of practitioner’s fees in 2017 (Kela, 2018d).
NHI also reimburses costs of travelling to a public or private health care provider due to illness, pregnancy, childbirth or rehabilitation. The costs which exceed the fixed co-payment of €25 are covered only for the nearest available place of treatment using the least expensive means of transport. In 2017, NHI covered 38% of the costs of outpatient prescription medicines, reimbursed 14–16% of private health services and 86% of travel and ambulance costs (Kela, 2018d).
In occupational health care there are no service fees for patients.
For prescribed outpatient medication three levels of reimbursement exist (basic at 40%, and special rates and 65% and 100%; see section 3.4.1 for further details). The special reimbursement rates are based on severity of condition. For example, medication for some chronic or long-term conditions, such as some cancers, is reimbursed at a 100% rate, while medication for diabetes is reimbursed at a 65% rate. The PPB decides upon the applications of pharmaceutical companies the reimbursement categories of the products. It can also restrict the special reimbursement to apply only for a certain or severe form of the disease. Finally, Kela decides the requirements and indications for special reimbursements.
There are few exemptions to user charges (see above for selected services and in some cases for children under the age of 18), and no exemptions based on income. Instead, welfare benefits exist for low-income households to assist with meeting the cost of living, including health care costs. The payment of the benefit is stipulated by the Act on Social Assistance (1997, revision 563/2019) and is the responsibility of municipalities. Social assistance includes a basic sum of money and supplementary benefit which takes into account certain expenses (e.g. user charges for health services and outpatient medicines). Under this system, user charges can be paid directly to the health care unit or pharmacy, or they can be reimbursed to the patient.
High levels of user charges led to the introduction of annual ceilings in the beginning of 2000. Over the years the ceilings have gradually increased and in 2018–2019 they amount to €1550 per year (see Box3.1, section 3.4 and Table3.3 for further details).
| Box3.1 | Table3.3 |
 |  |
Health care service users are responsible for monitoring whether the payment ceiling is met. A certificate of reaching the ceiling can be issued by a health centre or other public health care provider. Patients may be asked to present original receipts. The payment ceilings for parents also cover the fees for their children under 18 years of age.
In 2009 the use of service vouchers (previously covering municipal social and home care) was expanded to non-acute health services provided by municipalities. This expansion of the voucher scheme to cover municipal health services has provoked a discussion about equity, as patients using service vouchers may have access to higher quality services than those who do not use vouchers.
In comparison with many other Nordic and EU countries, Finland has a relatively high degree of cost sharing in health care, with 20% of health spending coming from out-of-pocket payments. The distribution of these payments as a share of total household consumption is regressive, and the incidence of catastrophic health spending linked to these payments is relatively high compared to other Nordic countries (Tervola et al., 2021). The main objectives of the legislative amendments in 2021 were to remove barriers to accessing healthcare and to increase health equity.
The new measures to reduce co-payments for publicly provided care were introduced in 2021, as the Act on User Charges in Health and Social Services was reformed. The renewed legislation abolished co-payments for nurse consultations in primary care, all outpatient clinic visits by people under the age of 18, and matters related to the treatment of certain communicable diseases. Additionally, co-payments for long-term home-based care were reformed.
The annual payment cap for user charges for the services remains at EUR 692, but the scope of this ceiling was broadened to include, for example, user charges for dental care, temporary home nursing, temporary home hospital care, and certain remote services. User fees covered by social assistance were also included in the annual payment ceiling calculation. Service users must monitor the completion of their payment caps themselves. Separate annual cap for co-payments for medicines (EUR 592,16) remains.
The changes to co-payments and the payment cap were estimated to reduce co-payments for 18% of the population (Government proposal 129/2020). In addition to financial objectives, the amendments aim to ensure that people would not need to resort to social assistance just to pay their user charges. Therefore, the Act emphasizes the preference for reducing or not collecting user charges over granting social assistance.
The amendments to the Act on User Charges in Health and Social Services entered into force on 1 July 2021. Amendments concerning the payment caps came into effect at the beginning of 2022. The renewal of this legislation is two-phased, and the second part has been planned to coincide with the overall health system reform implemented in 2023. In the second phase, the fees will be examined as part of the goals set for the establishment of Wellbeing Service Counties.
Authors
References
Tervola J, Aaltonen K, Tallgren F. Can people afford to pay for
health care? New evidence on financial protection in Finland.
Copenhagen: WHO Regional Office for Europe; 2021.
Ministry of Social Affairs and Health. 2023. User charges in healthcare and social welfare https://stm.fi/en/client-fees
3.3.2. Collection
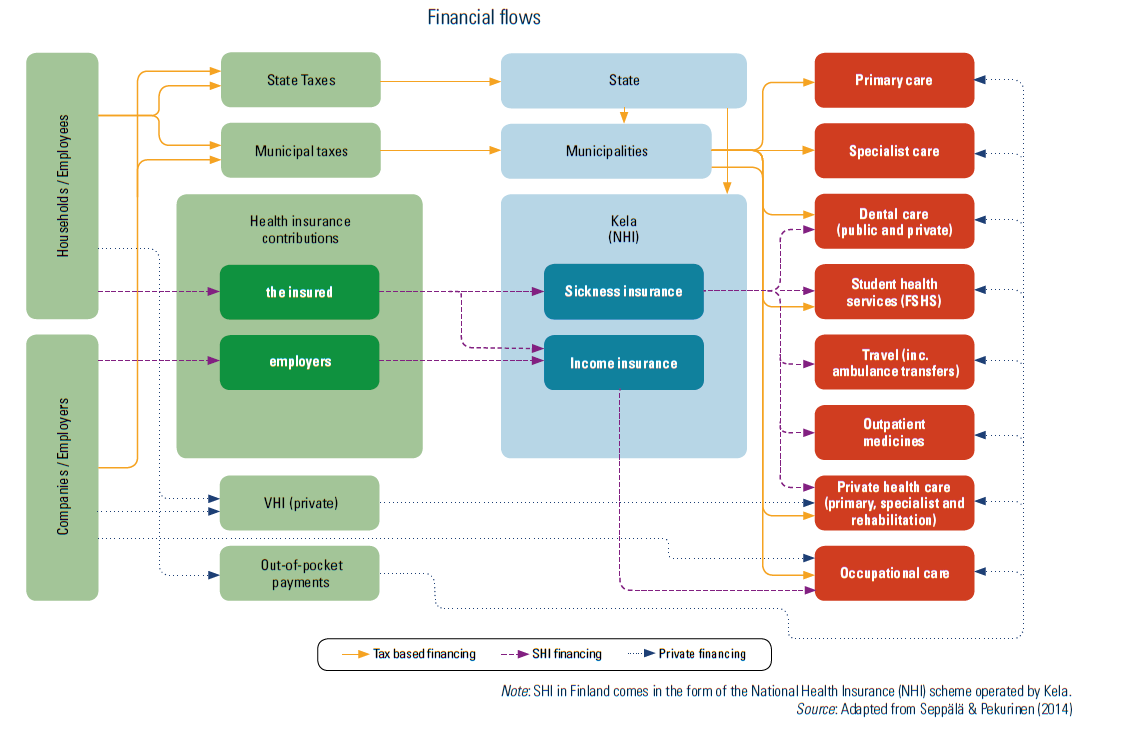
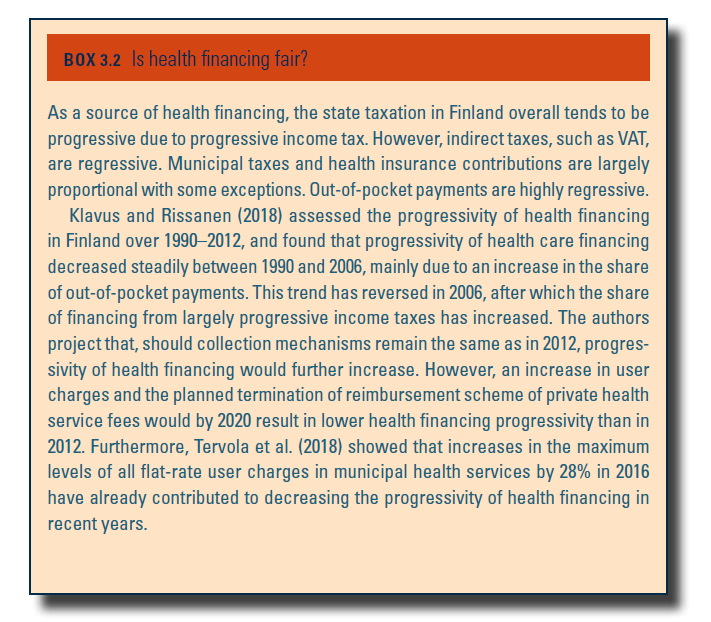
The financing of health care in Finland is collected mainly through six channels: state and municipal taxation, mandatory (national) and voluntary insurance fees, employer payments and out-of-pocket payments (see Fig3.6; see also Box3.2 for progressivity and regressivity of health financing). This section discusses the state, municipal and social insurance collection mechanisms, while user charges are discussed in section 3.4.
| Fig3.6 | Box3.2 |
 |  |
Central government
Regarding state taxation, over half of the total revenue in 2017 came from two sources: income and wealth tax (24.2%) and VAT (31.8%). Due to the slow economic growth, public spending relies on borrowing. In the 2019 state budget, the increasing Government debt amounted to €1.4 billion (3.2% of total state revenues). State-level financing is mainly channelled to health care in the form of state subsidies to municipalities and as state contributions to NHI funding.
Municipalities
In 2017, 50.8% of overall municipal revenues came from municipal taxes. The taxation rate is decided every year by each municipal council. Municipalities levy municipal income tax, real estate tax and receive a share of the revenues from corporate tax, although income tax is by far the most important (84% of municipal tax income in 2017). Municipal income tax is a fixed proportion of gross wage, which in 2017 varied between municipalities from 16.5% to 22.5% of taxable income (in 2017 the average was 20.7%). This has resulted in considerable variation across municipalities in the amount of revenues raised from taxation.
NHI
The funding of the NHI scheme consists of two parts: sickness insurance and income insurance. The range of contributions is defined in the Health Insurance Act (2004) but adjustments are made through annual decree by the Council of State. Since 2016, employees and self-employed people pay income insurance contributions (1.54–1.77% of income), while the employers’ contribution is 2.12% of gross wages. Other beneficiaries, such as pensioners, pay a sickness insurance contribution of 1.47% of income.
3.3.3. Pooling and allocation of funds
Allocation from collection agencies to pooling agencies
Due to the complex financing and provision arrangements for health care, there is no predefined overall public budget for health in Finland. However, there are two main pooling mechanisms: municipalities act as pooling agencies for municipal health care services, and Kela pools funds for private and occupational health services as well as for health care costs related to services and benefits, such as outpatient drugs, transport and sickness allowance (see Fig3.6). This dual public financing creates challenges for overall efficiency of service production which are described in section 7.5.
Fig3.6
Apart from organizing health services for their residents, municipalities are also responsible for many other public services, such as social care and primary and secondary education. The share dedicated to health is decided simultaneously with the budgets for other municipal services. As pooling agents, municipalities have two main sources of funding: municipal tax revenue described in section 3.3.2 and state subsidies.
Since 2010, subsidies are allocated for financing of the aforementioned primary municipal services. The purpose is to reduce differences in municipal tax revenues, cost structures and service needs. The subsidies are determined by a number of factors, such as population age structure, morbidity, unemployment rate, the number of students at local schools and education-related unit costs. Depending on tax revenues, municipalities can also receive additional top-up payments or have their subsidies reduced. These balancing items comprise about a fifth of all central Government subsidies for municipalities. In addition, municipalities can receive general subsidies not tied to any specific functions, and discretionary grants in the case of serious economic problems. Therefore, the total state subsidy varies greatly between municipalities.
Besides collecting contributions (see section 3.3.2), Kela also pools health care financing, and runs the NHI scheme. The state participates in the financing of NHI by defining the level of contributions (overall, while the employers and employees shares are often negotiated with labour market organizations) and covering a considerable part of the expenditure of sickness and income insurance from the state budget. In 2017, the state share of the NHI funding was 42%.The remaining funding came from contributions from the population (employees, the self-employed and pensioners), amounting to 38%, and the employers (21%).
Allocating resources to purchasers
While NHI uniformly covers the whole population for services covered by the NHI scheme, municipal health care allocation is much more fragmented (see above). In the beginning of 2017 there were 295 municipalities in mainland Finland (excluding the Åland Islands with its own health care system), with populations ranging from 811 to 635 000 people. To purchase specialized health care, municipalities have formed 20 hospital districts, while for tertiary care the country has been divided into five special responsibility areas.
Municipalities running their own health centres usually use prospective budgets. In federation-owned health centres the budgets are built in a similar way, but sharing of costs between member municipalities is usually determined based on the volume of services provided. For specialist level care provided by hospital districts (federations of municipalities), the majority of funding is based on the volume of services provided.
Occupational health care is purchased by employers for their employees. Kela reimburses part of the cost of occupational health care for employers. The total estimated costs of occupational health care in 2016 were €809 million, of which €347 million (43%) were reimbursed to the employers by Kela. This amounted to 13.4% of all NHI reimbursements (Kela 2018; THL, 2018b).
Well-being services counties (WBSC) are responsible for organizing health, social and rescue services for their residents and they get their funding from the state budget. WBSCs have to balance their budgets within three years, otherwise the Ministry of Finance (MoF) may initiate an evaluation procedure.
The WBSCs were established in 2023 and they began their first years with deficits. In the summer of 2025, MoF decided to launch the evaluation procedure in three of the WBSCs that are financially more vulnerable. The purpose of the process is to ensure WBSC’s capacity to organize the services. When the process is ongoing the WBSC is not allowed to make long term financial or other commitments, which limits their self-governance.
An evaluation team lead by an independent chairperson and including representatives from the WBSC, MoF, Ministry of Social Affairs and Health, and Ministry of Interior will provide recommendations on how to stabilize the county’s financial situation. The reports are expected by the summer of 2026. The team will also take a stand on an assessment of the regional division, initiated after the evaluation process if seen necessary. The process can lead to, for instance, merging the financially underperforming WBSC with a neighbouring WBSC.
MoF is also preparing a temporary regulatory change which would allow some WBSCs additional time to cover deficits that were created before 2025 with a deadline of end of 2028. This would apply to those WBSCs, that have successfully improved their financial situation (no new deficit in 2025) but have difficulties to fully balance their budget by the end of 2026 without risking the service system performance.
References
Ministry of Finance. 2025a. Finances of the wellbeing services counties – Valtiovarainministeriö https://vm.fi/en/finances-of-the-wellbeing-services-counties
Ministry of Finance. 2025b. Additional funding – Valtiovarainministeriö https://vm.fi/en/additional-funding
Ministry of Finance. 2025c. Hyvinvointialueen arviointimenettely käynnistyy kolmella alueella – Valtiovarainministeriö https://vm.fi/-/hyvinvointialueen-arviointimenettely-kaynnistyy-kolmella-alueella
Ministry of Finance. 2025d. Täysimääräisesti talouttaan tasapainottaville hyvinvointialueille harkinnanvarainen lisäaika alijäämien kattamiseen – Valtiovarainministeriö https://vm.fi/-/taysimaaraisesti-talouttaan-tasapainottaville-hyvinvointialueille-harkinnanvarainen-lisaaika-alijaamien-kattamiseen
3.3.4. Purchasing and purchaser–provider relations
There are three different health care systems which receive public funding: municipal health care (primary and specialist), private health care and occupational health care. Kela operates nominally as a purchaser of services which are covered by NHI reimbursements. With an exception of rehabilitation and, since 2018, ambulance services (see section 3.4.1), Kela does not make any purchasing contracts with private providers; instead reimbursements are made directly to service users upon application.
Municipal health care
In municipal health care there is no formal purchaser–provider split. The most common way for municipalities to organize health care services is still to provide primary health care in municipal health centres and to purchase specialized care from their respective hospital districts. They can also purchase services from other municipalities, other hospital districts, private providers or from the third sector. But, increasingly, municipalities establish integrated joint municipal authorities which provide primary and specialist health care as well as social services (Keskimäki et al., 2018).
Primary care
In the early 2000s, some large municipalities adopted a purchaser–provider split in their administration but since then most of these have departed from the model of somewhat artificially separating purchasing and delivery in their administration (Tynkkynen et al., 2013). However, municipalities can contract services from the private sector. For instance, in 2016, 27 health centres had contracted services from the private sector (Parhiala et al., 2016). In these cases, the contracts are signed after a procurement process, usually for up to three years with a potential option for extension. In the contracts, municipalities set criteria on content, staffing and quality of service. The payment mechanisms may vary but usually contracted providers are paid on the basis of capitation or, to a lesser extent, on the basis of global budget.
Municipalities’ purchasing know-how has often been considered inadequate (Tynkkynen et al., 2013). In particular, municipalities have recognized that the skills required for strategic purchasing have been lacking. Nevertheless, purchasing has been used by municipalities as a means to benchmark their own provision against private providers. Some municipalities have claimed that they want to provide residents with more choice in terms of providers. However, this strategy has not gained much traction due to the lack of consistent payment arrangements and thus the lack of economic incentives for the providers.
Specialist care
There are different contractual and negotiation mechanisms between hospital districts and municipalities for agreeing target volumes and payments, which comprise elements of purchaser and provider separation. Overall, there has been a tendency for budgets to be too low, which sometimes results in revisions in the course of the year.
In addition to contracting specialized health care services from their hospital districts, municipalities can organize specialist level services themselves; for example, by using health centres as a base for specialist consultations. Municipalities can also purchase services from other hospital districts or from private providers, normally on a case-by-case basis. However, the volume of such arrangements remains fairly minor.
Hospital district invoicing and pricing are in a continuous process of change, varying from district to district (Rättö et al., 2012) and the increasing tendency to establish the aforementioned joint authorities has further diversified the situation. Apart from some special arrangements for maintenance of readiness for catastrophes (such as large-scale traffic accidents or natural disasters) or pooling of exceptionally high costs, payments of municipalities have usually been based on price lists by either service item or a package of services (along the general principles of NordDRG pricing).
Occupational health care
In occupational health care services there is a purchaser–provider split, as employers contract private or municipal health service providers. In the contracts, employers define the level and scope of services purchased for their employees. Some larger companies may also have their own health units to provide services. Services are covered fully by employers, who are partly reimbursed retrospectively by the NHI, based on actual costs.
Private health care
For private sector patients, the NHI reimburses costs for some services and pharmaceuticals (see section 3.3.1). Kela is in general a passive purchaser and does not contract providers of health services, with the exception of rehabilitation services. Since 2003, the latter are contracted based on competitive biddings every fourth years. Kela defines the service standards (objective of a particular rehabilitation type, content of services, personnel qualification requirements, and outcome indicators). In addition, providers are being rated on quality (e.g. of premises, staff training and patient experience). This contracting system has been criticized for accepting nearly all tenders, which led to increasing costs and variations in provider charges (Aalto University, 2018). In the latest 2018 bidding round, Kela underlined price competition more than previously, prompting criticism regarding the omission of quality standards and overall cost-efficiency due to patients’ longer distances to services.
For services funded by VHI, the insurance companies have largely been passive purchasers (Alexandersen et al., 2016). Usually they do not have contracted providers in ambulatory care. However, they often have negotiated prices with the largest private providers. For inpatient care and day surgery the private insurers may use contracting. Some insurance companies also have their own hospitals (see section 4.1).