-
18 September 2025 | Country Update
Freedom of choice pilot for persons aged 65 and over -
13 March 2025 | Country Update
Increases in user fees -
31 May 2023 | Policy Analysis
Change in legislation to reduce high degree of cost sharing
3.4. Out of pocket payments
As shown in Table3.1, about a fifth of total health spending in Finland comes from out-of-pocket payments. This share has remained relatively stable since the mid-2000s and has varied between 19.0% and 20.4%. Out-of-pocket spending per person has doubled in Finland from US$ 423 PPP in 2000 to USPPP in 2000 to US$ 837 PPP in 2016. Before the financial crisis of 2008, per capita growth in public expenditure on health was overtaking growth in out-of-pocket payments (8% and 5% average annual growth between 2000 and 2008 respectively), whereas since 2009 out-of-pocket spending per capita increased at a faster pace (4% vs 3% growth in public spending) (WHO, 2018b).
Table3.1
 nbsp;837 PPP
in 2016. Before the financial crisis of 2008, per capita growth in
public expenditure on health was overtaking growth in out-of-pocket
payments (8% and 5% average annual growth between 2000 and 2008
respectively), whereas since 2009 out-of-pocket spending per capita
increased at a faster pace (4% vs 3% growth in public spending) (WHO,
2018b).
nbsp;837 PPP
in 2016. Before the financial crisis of 2008, per capita growth in
public expenditure on health was overtaking growth in out-of-pocket
payments (8% and 5% average annual growth between 2000 and 2008
respectively), whereas since 2009 out-of-pocket spending per capita
increased at a faster pace (4% vs 3% growth in public spending) (WHO,
2018b).
Table3.1
User charges in municipal health centres were introduced in 1993, during the deep recession. Meanwhile, inpatient hospital care has traditionally been subject to cost sharing. In 2008, the legislation on user charges was reformed again, allowing the MSAH to set maximum charges biannually, taking into account inflation. In the beginning of 2016 the user fees for municipal health care services were raised by 28% with the aim to increase the revenue collection from out-of-pocket payments by €150 million (Klavus & Rissanen, 2018). At the same time, NHI reimbursement for private services has decreased, mainly because the NHI levels of reimbursement have not followed increases in actual service fees.
In 2015, about half of the population in Finland incurred out-of-pocket spending for health and social welfare services. Among these, 36% paid flat fees (e.g. for primary or specialist care), amounting to €197 on average; about 5% paid income-related fees (e.g. for home-based, long-term or social care), amounting to €3505 on average; and 22% paid for dental services, amounting to €104 on average (Vaalavuo, 2018).
Concerns that extensive user charges may lead to issues with accessing services and financial protection led to the introduction of an annual ceiling for health care costs in the beginning of 2000. The existence of separate ceilings for services, medicines and travel costs raised the total annual cap on out-of-pocket payments for health care services to €1550 (see Table3.3) and service users may still incur further charges. In 2015, 6% of the population (about 330 000 people) reached at least one of the ceilings, while 0.1% reached all of them (Vaalavuo, 2018). There are no exemptions from user charges based on income.
Table3.3

The government launched a freedom of choice pilot that allow persons aged 65 and over to use private GP services with a user fee similar to that in public primary care centres. The pilot began on 1 September 2025 and ends at the end of 2027. The aim of the pilot is to improve the availability of and access to primary healthcare and provide more freedom of choice for customers.
The pilot is funded through Kela, which reimburses service providers for the amount exceeding the deductible. Maximum prices will be set for the services included in the pilot. This is the first time price regulation is used for the reimbursements Kela pays for the costs of private health services. The pilot is intended to also help Kela to advance its reimbursement system.
The pilot covers two private GP appointments per person in 2025 and three in 2026 and 2027. The number of appointments is limited to curb costs. Also some examinations and tests in the private sector are included in the pilot such as certain laboratory tests and imaging services. For those, the reimbursement will be half of the maximum fee determined by Kela. The private providers contract with Kela to receive the reimbursements.
References
Social Insurance Institution of Finland (Kela). 2025a. A pilot study on freedom of choice in healthcare for persons aged 65 or over. | Our Services | Kela https://www.kela.fi/appointments-with-a-private-general-practitioner-for-persons-aged-65-or-over
Social Insurance Institution of Finland (Kela). 2025b. Pilot study on freedom of choice in healthcare for persons aged 65 or over | About Kela | Kela https://www.kela.fi/pilot-study-on-freedom-of-choice-in-healthcare-for-persons-aged-65-or-over
Ministry of Social Affairs and Health. 2025. 65 vuotta täyttäneiden valtakunnallinen valinnanvapauskokeilu – Sosiaali- ja terveysministeriö https://stm.fi/65-vuotta-tayttaneiden-valtakunnallinen-valinnanvapauskokeilu
Authors
References
Ministry of social affairs and health 2024. https://stm.fi/terveydenhuollon-maksukatto
Ministry of social affairs and health 2024. https://stm.fi/-/sosiaali-ja-terveydenhuollon-asiakasmaksujen-enimmaismaarat-nousevat-vuoden-2025-alusta
In comparison with many other Nordic and EU countries, Finland has a relatively high degree of cost sharing in health care, with 20% of health spending coming from out-of-pocket payments. The distribution of these payments as a share of total household consumption is regressive, and the incidence of catastrophic health spending linked to these payments is relatively high compared to other Nordic countries (Tervola et al., 2021). The main objectives of the legislative amendments in 2021 were to remove barriers to accessing healthcare and to increase health equity.
The new measures to reduce co-payments for publicly provided care were introduced in 2021, as the Act on User Charges in Health and Social Services was reformed. The renewed legislation abolished co-payments for nurse consultations in primary care, all outpatient clinic visits by people under the age of 18, and matters related to the treatment of certain communicable diseases. Additionally, co-payments for long-term home-based care were reformed.
The annual payment cap for user charges for the services remains at EUR 692, but the scope of this ceiling was broadened to include, for example, user charges for dental care, temporary home nursing, temporary home hospital care, and certain remote services. User fees covered by social assistance were also included in the annual payment ceiling calculation. Service users must monitor the completion of their payment caps themselves. Separate annual cap for co-payments for medicines (EUR 592,16) remains.
The changes to co-payments and the payment cap were estimated to reduce co-payments for 18% of the population (Government proposal 129/2020). In addition to financial objectives, the amendments aim to ensure that people would not need to resort to social assistance just to pay their user charges. Therefore, the Act emphasizes the preference for reducing or not collecting user charges over granting social assistance.
The amendments to the Act on User Charges in Health and Social Services entered into force on 1 July 2021. Amendments concerning the payment caps came into effect at the beginning of 2022. The renewal of this legislation is two-phased, and the second part has been planned to coincide with the overall health system reform implemented in 2023. In the second phase, the fees will be examined as part of the goals set for the establishment of Wellbeing Service Counties.
Authors
References
Tervola J, Aaltonen K, Tallgren F. Can people afford to pay for
health care? New evidence on financial protection in Finland.
Copenhagen: WHO Regional Office for Europe; 2021.
Ministry of Social Affairs and Health. 2023. User charges in healthcare and social welfare https://stm.fi/en/client-fees
3.4.1. Cost sharing (user charges)
Table3.3 shows maximum fees which municipalities can charge for health care services in 2018–2019, according to the latest Decree on User Fees in Social and Health Care (2017). Municipalities can set lower fees (e.g. some do not charge for GP visits), but this is not a widespread practice. According to a recent municipal survey, 70% of the population lived in municipalities charging the maximum fees for doctors’ and nurses’ visits in 2018 (Haaga, 2019). Usually user charges for services are not paid at the point of service use at the health care facility. Instead, patients are invoiced after the visit.
Table3.3
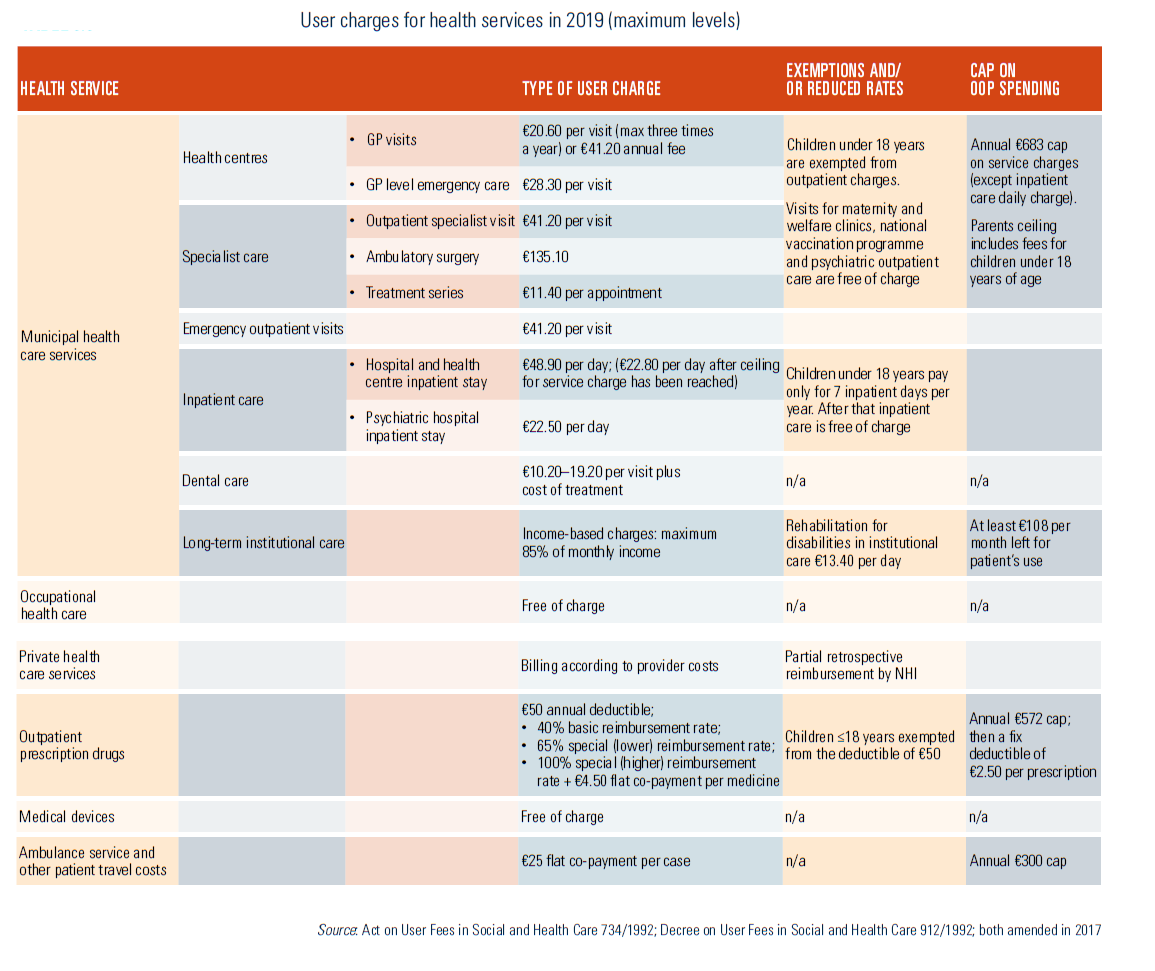
Health centre user charges
In health centres, patients can choose to pay per visit or by annual charge for appointments with a GP. People aged 15 years and older may be required to pay a penalty charge of €50.80 for not attending appointments. There is a charge for a visit to the health centre emergency clinic on weekdays between 8 p.m. and 8 a.m., and on Saturdays, Sundays and bank holidays. A basic fee for dental care depends on the health professional’s qualifications. On top of this, a fee for treatment from €8.40 (for a basic examination) to over €200 (dentures) can be charged. There is also a daily charge of inpatient care in a health centre inpatient ward. Several services, such as maternity and child welfare visits, laboratory tests, X-ray examinations and national programme vaccinations, are free of charge. In 2015, 12% of the population received health care centre outpatient treatment for free, 17% paid the annual fee of €32–42, and 70% paid according to use, up to €21 per visit (Vaalavuo, 2018).
Hospital user charges
Hospitals charge for a visit to an outpatient department, an outpatient surgery procedure, a daily hospital fee for inpatient care, a series of treatments and rehabilitation. Daily inpatient hospital charges cover examinations, treatment, medicines and meals. A maximum of 85% of a patient’s monthly income (for example, retirement pension) can be charged for long-term hospital or institutional care. At least €108 per month out of patient’s income must remain available for the patient after paying the user charge.
Other specialist care charges
With regard to a series of treatments, a fee of €11.40 is charged for each appointment for up to 45 appointments a year. A series of treatments can consist of, for example, dialysis, radio- or chemotherapy and medical rehabilitation. A daily fee of €16.90 can be charged for rehabilitation of a physically or mentally disabled person. A fee of €61.00 can be charged for a medical certificate (for a driver’s licence), but other certificates have a maximum charge of €50.80.
Home care charges
The fees for care provided at home depend on the nature of care/treatment. A maximum of €18.90 per visit is charged for occasional treatment by a physician or a dentist, while €12.00 is charged for a visit by other types of health care professionals. A monthly fee is applied for long-term care/treatment, which depends on the type and extent of service, as well as on household’s composition and monthly income.
Ceiling for user charges in municipal health care
In 2018–2019, the ceiling for user charges in municipal health care is €683. The ceiling covers outpatient charges for most chargeable services, such as visits to the health centre, physiotherapy, and hospital care, but it does not include charges for dental care and ambulance services, and services with income-related charges. Dental care, certificates, diagnostic tests based on private sector referrals and patient transportation are excluded from the ceiling, but there is a separate cap for transportation. Once the ceiling is reached, service users can claim a certificate (based on receipts) from a municipal health care provider, relieving them of further user fees. After that, patients receive outpatient services free of charge, and pay for hospitalization at a reduced daily rate. The payment ceiling for parents also covers the fees for their children under 18 years of age.
Private health care services
In the private sector, patients pay all treatment costs themselves, but may claim partial reimbursement (according to the reimbursement tariff) from the NHI. Private providers set their price for services, which always exceeds the level of reimbursement. In 2017, the average reimbursement rate for private sector physician services was 16%, for dental services 14%, and for various examinations and treatments 13% (Kela, 2018). In case the provider has a direct reimbursement contract with Kela (e.g. for rehabilitation services), the payment up to reimbursement level is charged to NHI, while the patient pays the difference between the actual costs and the reimbursement tariff.
Ambulance and other transportation
For ambulance services the patient pays a flat fee of €25 with the rest (and up to €67) covered by NHI directly to the service provider. NHI also reimburses the cost of other forms of transportation for examination or treatment (for example, a taxi) if the sum exceeds €25. If the cost of transportation exceeds €300 per year, NHI reimburses all transport costs in excess of this limit.
Outpatient medicines
NHI reimbursements are paid for outpatient medicines, clinical nutrients and emollient creams prescribed for the treatment of an illness and included in the reimbursement list. Since 2017, reimbursement for adults can be received only for costs exceeding the initial deductible of €50 per calendar year. The rate of reimbursement (see also section 3.3.1) depends on the category of the product: 1) basic rate of reimbursement at 40%; 2) lower special rate of reimbursement at 65%; and 3) higher special rate of reimbursement at 100%. The latter still requires a co-payment of €4.50 per medicine per purchase. The reimbursement is deducted from the price of the medicine at the point of purchase. There is an annual ceiling on out-of-pocket payments for prescribed medicines (€572 in 2019), after which all costs are covered by the NHI with the patient paying a fixed deductible fee of €2.50 per prescription.
Medical devices
Medical devices, such as assistive devices for people with disabilities and devices for treating diabetes and monitoring blood glucose, are provided free of charge by municipal health services (a local health centre or a hospital district). The need for the device is assessed by a medical professional and registered in the patient’s treatment plan.
3.4.2. Direct payments
Direct payments apply for services not covered by the public financing schemes (e.g. private non-curative services, such as cosmetic surgery), and for pharmaceuticals not on the reimbursement list (e.g. hormonal contraception).
3.4.3. Informal payments
No comprehensive evaluation has been carried out on informal payments, but there is no indication that these payments play any role in Finnish health care.