-
30 May 2023 | Country Update
Relaunch of the Swiss Health Care Atlas -
22 January 2019 | Country Update
New eHealth strategy aims to establish the electronic health record in Switzerland -
23 May 2017 | Policy Analysis
National cancer registry to be implemented in 2018 -
15 April 2017 | Country Update
Law on electronic health records (EHR) enters into force
2.7. Health information management
The Swiss Atlas of Health Care, published and relaunched in April 2023, documents regional differences in the use of health care services. As an expansion of the original Health Care Atlas 2017, the updated Care Atlas incorporates a larger scope of measures and indicators, including those for outpatient care. It serves as a basis for comparative analysis of regional variability in health care practises and utilisation within Switzerland, forming a basis for health services research. It includes more than 100 indicators of both inpatient and outpatient health care, which are presented as standardized rates in a user-friendly and highly visual care landscape both for hospital regions and cantons.
The current set of indicators in the Care Atlas is the result of data gathered during the years of 2013–2021. The Care Atlas is designed as a learning system with continuous data updates. This learning system approach will will enable relevant authorities to conduct evidence-based planning and assessment of needs-based care. Policy decisions can be informed by tracking and measuring regional quality indicators and geographic patterns.
The Swiss Health Care Atlas was co-financed by the Swiss Health Observatory (Obsan) and the Federal Office of Public Health (FOPH), and the operational realization was headed by Obsan with the support of a broad-based advisory group, including organizations working in healthcare and academic institutions.
The Swiss Health Care Altas can be accessed via: https://www.versorgungsatlas.ch/en.
Authors
References
Bayer-Oglesby, L., Addor, V., & Ruedin, H. J. (2020, December 7). Home. OBSAN Swiss Health Observatory. https://www.obsan.admin.ch/en
BAG. (2023, April 4). Relaunch des Schweizer Versorgungsatlas. Bundesamt für Gesundheit BAG. https://www.bag.admin.ch/bag/de/home/das-bag/aktuell/news/news-04-04-2023.html
In December 2018, the new Strategy eHealth Switzerland 2.0 2018–2022 was adopted, replacing the former eHealth strategy (2007). The strategy accompanies the introduction of the electronic health record (elektronische Patientendossier, EPD). The EHR will become available in spring 2020. By then, all hospitals will be required to integrate relevant data into electronic health records.
The strategy also aims (1) to promote use of mhealth and other digital health solutions, (2) improve data security, (3) promote coordinated use and exchange of health data, (4) enhance multiple use of data and related infrastructure (ensure interoperability), and (5) improve digital literacy of the population to handle health data securely.
The Strategy will be implemented by the Confederation, the cantons, eHealth Suisse and so-called “communities” that are private legal bodies built around population groups (i.e. the whole population residing in a specific area or a Canton) and can be funded by groups of hospitals, GPs, pharmacies or other existing networks of healthcare providers. eHealth Suisse, the joint coordination body of the Confederation and the cantons, coordinates the implementation of the e-Health strategy.
Authors
Context
Every year about 38,000 new cancer cases are diagnosed in Switzerland and about 16,000 people die of cancer. It is estimated that in the next 20 years, cancer-related deaths will increase by one third.
Cancer registries are important monitoring systems that allow data collection on incidence rates of new cancer cases, types of cancer, death rates across regions and/or countries and the analysis of cancer trends over time.
There are currently 15 cantonal and regional cancer registries in Switzerland that register cancer cases for about 94% of the Swiss population. With the exception of three cantons (Jura, Lucerne and Ticino) none of the cantonal cancer registries has a formal legal basis. Yet, all registries have a general register permit that authorizes physicians to pass on non-anonymous data to the respective registry.
Impetus
In Switzerland, efforts to systematically register cancer data reach back into the early 1970s, but a national effort was only proposed in 2007. In December 2010, the Federal Council commissioned the Federal Department of Home Affairs to develop a preliminary draft of a federal law, which was further elaborated by the Federal Office of Public. Between December 2012 and March 2013, the draft was under public consultation and, almost unanimously, supported.
Reform
In March 2016, the Swiss parliament passed a bill to establish a national cancer registry and the executive regulations of the law are currently in public consultation. The law is supposed to come into force gradually beginning 2018. The national cancer registry will serve as a comprehensive database to inform the development of prevention and early-detection programs. Further, it will support cantonal care planning, future evaluations of the quality of health services, and other cancer related research.
The law will regulate the collection, registration and transmission of data. According to the new law physicians, as well as hospitals and other private or public health institutions, will be obliged to report all diagnosed cancer cases but patients will be able to object to the registration of their data at any time.
Regulations will build on already existing structures of cancer registration, i.e. the cantonal registries. Only cancers diagnosed in children and adolescents will be registered in the children’s cancer registries, which are managed by the federal government. Data collected by the cantonal registries and the children’s cancer registries will be merged and processed at the national level by the national cancer registry. Data will be used for an annual cancer monitoring process (Federal Statistical Office) and published in an in-depth report on cancer.
In order to answer to specific questions that are relevant to current health policies, the Federal Council is allowed to demand further data collection efforts, for example, concerning particular types of cancer and/or groups of patients , such as children or adolescents, if needed to answer specific policy-relevant questions.
Authors
References
Federal Office of Public Health (2016). Geltende Regelungen zur Krebsregistrierungen. [Current regulations related to cancer regsitration] https://www.bag.admin.ch
Federal Office of Public Health (2017a). Krebsregistrierungsgesetz vom Parlament verabschiedet. [Law on cancer registries passed by parliament] https://www.bag.admin.ch
Federal Office of Public Health (2017b). Entwurf Krebsregistrierungsgesetz. [Draft law on cancer registration]
https://www.bag.admin.ch
A new law on electronic health records (EHR) officially entered into force on April 15, 2017. The EHR is part of the federal health strategy 2020 and aims at increasing quality and patient safety, and improving overall efficiency of medical care.
A central element of the new regulation includes specifications for the certification of EHR communities. Communities are associations of hospitals, doctor’s offices, pharmacies and other healthcare facilities, which ensure the safe electronic exchange of EHR embedded data. The regulations also specify the new patient identification number, which will allow the clear identification of individual patients.
Hospitals will have three years to introduce the EHR, and nursing homes and birthing homes will have five years. For medical practices and other health care facilities in outpatient care, adoption of EHR via parent communities will remain voluntary. The first patients should be able to open an EHR in the second half of 2018.
Authors
References
2.7.1. Information systems
Data collection and analysis of health-related information are regulated by different federal laws, most importantly the 1992 Federal Statistics Act (BStatG/LSF) and the KVG/LAMal. Since the 2007 revision of KVG/LAMal (see section 6.1), the law specifies that the FSO collects the data necessary for monitoring the effects of the law, including data collection from insurers, providers and the population.
Table2.1 provides an overview of the most important health-related statistics in Switzerland. All statistical reports are usually available for download from the responsible institutions free of charge. The FSO and the FOPH are the two most important institutions for the collection of information. The FSO aggregates data from municipal bureaus of vital statistics (via the registry Infostar) into the federal cause of death statistics; collects data on the health status of the population through the Swiss Health Survey every five years; and summarizes data from cantonal cancer registries. It is also responsible for different hospital statistics and for statistics on Spitex (home care) providers and sociomedical institutions (particularly nursing homes) (see Table2.1) as well as for the national statistics of costs and financing of the health system, which follow the international standard System of Health Accounts (OECD/Eurostat/WHO, 2011).
Table2.1
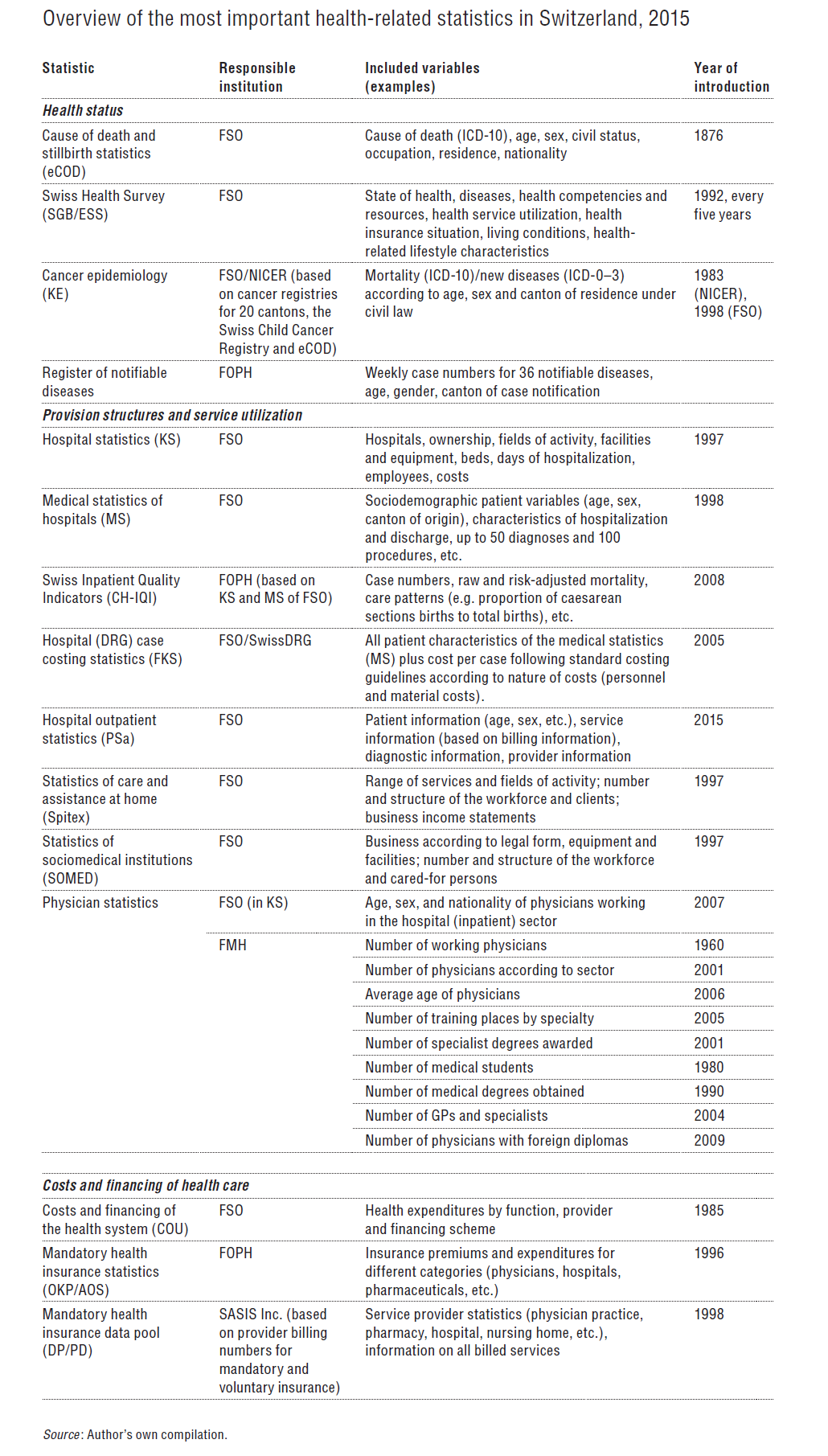
The FOPH collects data on MHI (OKP/AOS statistics); operates the register of notifiable diseases; and organizes the Swiss Inpatient Quality Indicators (CH-IQI) database. The FOPH also monitors the development of costs and expenditure of MHI based on a data pool operated by SASIS Inc. – a subsidiary organization of santésuisse, which collects data from all providers with a billing number for services reimbursable by MHI (about 99% of providers). The physician statistics of the FMH provide information about practising physicians, medical graduates, postgraduate training (specialization), places in hospitals, etc.
Another important resource for information on the Swiss health system is the Obsan. Obsan carries out analyses of health-related data with the aim of informing health policy-makers and the wider public. It publishes reports on a wide range of issues, based on data collected by the above mentioned statistics.
The availability of data on health service provision has improved considerably since the late 1990s, when mandatory collection of structural and service provision data was introduced for hospitals, Spitex organizations and sociomedical institutions. A first step towards more transparency about resource utilization in hospitals was made with the introduction of the voluntary hospital (DRG) case costing statistics in 2005, which has been coordinated by SwissDRG SA since 2008. Also quality of care in hospitals has become more transparent since the introduction of the CH-IQI (see section 5.4.2).
However, information on service provision in the ambulatory sector remains rather limited (except for provider billing information). Currently, the FSO is preparing to improve data availability for ambulatory care: first, the hospital statistics (KS) will be extended to include information on ambulatory care provision structures in hospitals; second, additional hospital outpatient statistics (PSa) will be introduced in 2015; third, the introduction of statistics for structural data on other ambulatory providers (practices and health centres) is planned.
In October 2014, the Federal Council proposed a new Federal Law on Cancer Registration (KGR/LEMO). The law aims to improve the available epidemiological data on cancers, currently derived from cancer registries covering 20 cantons aggregated by the National Institute for Cancer Epidemiology and Registration (NICER). The law proposes to build on the existing cantonal infrastructure but to introduce mandatory notification of diagnosed cancers (with the option for patients to veto). In addition, it plans to give the Federal Council the right to provide financial support to other registries, e.g. for CVD and diabetes.
2.7.2. Health technology assessment
The FOPH is responsible for assessing whether new – and, if controversial, also existing – technologies comply with the principles of effectiveness, appropriateness and cost-effectiveness, as required by KVG/LAMal. The exact procedures required prior to inclusion in the benefits package differ depending on whether they concern a new service provided by physicians, a new laboratory test or medical device, or new pharmaceuticals (see section 2.8.1 for a description of the necessary steps required for inclusion of technologies in the benefits basket). There are two units of the FOPH involved in the assessment of new technologies: (1) the Medical Services Section (MSS), which is responsible for assessing health services, laboratory tests, devices and products for use by patients; and (2) the Pharmaceuticals Section, which is responsible for assessing (and reassessing) pharmaceuticals (for more details on assessments of pharmaceuticals, see section 2.8.4, and for medical devices and aids see section 2.8.5).
The assessments of the FOPH are inspired by international standards for health technology assessment (HTA) and follow these standards to a certain extent (Federal Council, 2014). However, assessments of new technologies are mostly carried out by the FOPH based on documents provided by applicants who aim to have a certain technology included in the MHI benefits basket (FOPH, 2011a). Detailed guidelines exist for applicants concerning the required documentation they have to submit as part of their proposal to support the assessments by the FOPH. The FOPH may request additional documents from applicants, can commission external evaluations, and may conduct its own research as part of its assessment. However, the ability of the FOPH to carry out its own research is limited because of resource constraints in the responsible units (FOPH, 2014g). Assessments are, therefore, mostly based on: existing (usually international) studies; commissioned external evaluations/reviews; or reports by HTA agencies of other countries. Formal cost-effectiveness analyses are very rarely conducted by the FOPH. Evaluations are not generally made publicly available. Subsequently, the relevant advisory commission (i.e. ELGK/CFPP, EAMGK/CFAMA or EAK/CFM) appraises the evidence produced as part of this assessment process (see section 2.8.1).
The procedures for the assessment of technologies were subject to inspections and criticism by the parliamentary control of the administration office in 2008 (Parlamentarische Verwaltungskontrolle, 2009) and there has been a vast amount of public discussion about the need to introduce a system of systematic horizon scanning, harmonizing procedures of HTA for different types of technologies and increasing transparency. Partially in response to this criticism, official criteria for the assessment of services provided by physicians were developed in 2011 (FOPH, 2011a) with the aim of operationalizing the principles of effectiveness, appropriateness and cost-effectiveness. However, similar formal criteria do not yet exist for laboratory tests, medical devices for home use by patients or pharmaceuticals, although there are plans to introduce such criteria (FOPH, 2014g). A handbook for the preparation of reimbursement applications of pharmaceutical companies to the FOPH (FOPH 2013g) provides a rough operationalization of the criteria of cost-effectiveness, which are based mostly on internal and external reference pricing approaches.
A Swiss Network for Health Technology Assessment (SNHTA) was set up as early as 1998 to bring together all HTA-related activities in Switzerland. Its members include the different units of the FOPH, the GDK/CDS, FMH, as well as several universities and hospitals. A development with potentially important consequences for HTA in Switzerland was the inclusion of measures aiming to improve HTA through a proposed Federal Law on the Centre for Quality in MHI (Federal Council, 2014). This would have supported the FOPH by: (1) introducing a system for horizon scanning in order to identify whether new services should undergo HTA; (2) introducing a system for re-evaluating currently covered technologies; (3) producing HTA reports; and (4) developing and updating a methodology for HTA in Switzerland. However, due to considerable opposition from different stakeholders, the proposed law was withdrawn and it remains to be seen how the HTA process will develop over the next few years (see section 6.2.1).
Another important actor, the Swiss Medical Board, is also actively campaigning for improving (or completely overhauling) the current system of technology assessment in Switzerland (Swiss Medical Board, 2015). This initiative originally started in 2008 as the Medical Board of Zurich. In 2011, the GDK/CDS, FMH, Swiss Academy of Medical Sciences (SAMW/ASSM) and the government of Liechtenstein joined the initiative. In 2015, santésuisse, curafutura and interpharma, which had originally set up another network called SwissHTA, also joined the Swiss Medical Board initiative with the aim of forming a common and more efficient HTA organization for Switzerland, partly because they felt that the FOPH had not fulfilled its role in this domain. The Swiss Medical Board has produced 14 HTA reports (up until September 2015), some of which have been highly controversial (in particular the report on systematic mammography in 2013 (Swiss Medical Board, 2013)).