-
24 January 2022 | Policy Analysis
The strategy to shift surgical interventions to outpatient settings has achieved its goals
7.5. Health system efficiency
In 2012, Switzerland spent 11.3% of its GDP on health, considerably more than the EU average (9.5%) (see section 3.1), although less than the Netherlands, France and Austria. Per capita expenditure in Switzerland were US$ PPP 6062, which was far above the EU15 average (US$ PPP 3852) and was exceeded in the European region only by Luxembourg. Above-average expenditure is not problematic if resources are spent efficiently and if expenditure reflects population preferences for more and better care. A 2010 OECD study (Joumard, André & Nicq, 2010) examined efficiency of different health care systems and found that Switzerland was among the most efficient countries, in terms of achieving high life expectancy for employed resources. However, a detailed analysis of allocative and technical efficiency of the Swiss health system reveals that inefficiencies are likely to exist in both.
An evaluation of the 2019 reform to shift interventions from hospital to outpatients settings has shown positive effects in terms of reduced numbers of inpatient treatments.
Since early 2019, the costs of
six groups of interventions are only reimbursed by the health insurance
funds if they are performed on an outpatient basis (see Analyses: https://eurohealthobservatory.who.int/monitors/health-systems-monitor/analyses/hspm/switzerland-2015/outpatient-care-takes-precedence-over-inpatient-care-six-groups-of-surgical-interventions-to-be-moved-to-outpatient-care).
Justified cases are exempt from this regulation, and in the case of
non-covered circumstances, inpatient treatment is only possible after
prior approval of costs by the insurer. The six groups of interventions
are:
- Unilateral varicose vein surgery of the legs
- Haemorrhoid procedures
- Unilateral inguinal hernia surgery
- Examinations/interventions on the cervix or uterus
- Knee arthroscopy, including arthroscopic surgery on the meniscus
- Tonsil and adenoid surgery
The 2019 reform has shown to be effective both in terms of volume and price.
On
behalf of the FOPH, the Swiss Health Observatory has been monitoring in
the first three years the actual effects of this regulation, in terms
of number of outpatient and inpatient interventions, costs, quality of
treatment and administrative processes
for billing and auditing. Results show that number of inpatient
surgeries compared to the population and the corresponding costs have
declined more sharply since 2019 than in previous years. Depending on
the group of procedures, this decline in volume
varied: it ranges from 17% for knee arthroscopies to 48% for
haemorrhoid procedures. Correspondingly, the rate of outpatient
operations has increased in most cases.
It is not possible to analyse the effects on the quality of treatment with the routinely collected statistical data. A final evaluation will be carried out based on the results from the monitoring and the study. Based on the results of this evaluation, a decision will be made as to whether and how the “outpatient before inpatient” regulation will be expanded or adapted.
Authors
References
Bundesamt für Gesundheit BAG. (2 December 2021). Ambulant vor Stationär. BAG. https://www.bag.admin.ch/bag/de/home/versicherungen/krankenversicherung/krankenversicherung-leistungen-tarife/Aerztliche-Leistungen-in-der-Krankenversicherung/ambulant-vor-stationaer.html (in German, last accessed 24 January 2022)
Federal Office of Public Health FOPH. (30 November 2020). Ambulant vor stationär: Ziele erreicht. BAG. https://www.bag.admin.ch/bag/de/home/das-bag/aktuell/medienmitteilungen.msg-id-81401.html (last accessed: 24 January 2022)
7.5.1. Allocative efficiency
The term “allocative efficiency” refers to the notion that society’s resources should be used in such a way that they best satisfy the population’s needs and wants. In the case of the health sector this is usually interpreted to mean that the allocation of resources between the various levels and types of care is consistent with health system objectives (e.g. maximization of health). In Switzerland, allocative efficiency can be assessed at three different levels: (1) the allocation of resources to different regions; (2) the allocation of resources to different types of provider; and (3) the allocation of resources to different types of service.
Resources allocated to health vary widely across cantons: public expenditure in 2012 differed almost twofold between the eight cantons with the lowest costs (Sw.fr.3000 to Sw.fr.3500) and the canton with the highest costs (Basel-Stadt with more than Sw.fr.5900) (see section 3.1). The reasons for these differences have been explored in numerous studies (Busato et al., 2010, 2012; Reich et al., 2012b; Camenzind, 2012a; Crivelli, Filippini & Mosca, 2006; Schleiniger, 2014), and a host of different factors, such as provider density, payment mechanisms, population demographics, urbanity and per capita income have been identified as explanatory factors. However, most researchers conclude that supplier-induced demand, resulting from flawed incentives of (unlimited) FFS reimbursement, subsidized hospital investments and fragmentation of provision, is an important factor leading to inappropriate (and inefficient) use of resources (Trageser et al., 2012).
Regional resource allocation in Switzerland is mostly determined by historic factors, reflecting past (political) planning and investment decisions of cantons, provider choices about their preferred place of practice, and patient choices of their preferred provider. Objective criteria, such as population demographics and epidemiology, only have an indirect effect if they are reflected in cantonal planning decisions or in differences of MHI premiums. Although recent reforms have attempted to improve cantonal inpatient planning (see section 6.1.2), and future reforms are focused on better planning of ambulatory care (see section 6.2.2), large unintentional differences in expenditure are likely to remain across regions. In addition, the restriction of the MHI risk-adjustment system to account only for differences within cantons (or within subcantonal premium regions) prevents the redistribution of resources across cantonal borders, even if demographic or epidemiological factors would demand that resources are allocated differently.
Concerning the second point, i.e. the allocation of resources to different types of provider, flawed financial incentives exist at different levels of the health system, potentially distorting the allocation of resources to different providers. First, the dual (cantons and MHI companies) system of financing of inpatient care (see section 3.7.1) means that MHI companies have no interest in promoting less costly (and more efficient) ambulatory care, where they would have to cover the full costs, rather than more expensive inpatient care, where more than 50% of costs are covered by cantons (Trageser et al., 2012). At the same time, cantonal hospitals might have an interest in increasing the provision of ambulatory care reimbursable by MHI in order to amortize their otherwise underutilized infrastructures (such as radiology departments, laboratories, etc.). Concerns exist that the flawed incentives of this dual financing lead to inappropriate use of inpatient care and parliamentary initiatives, as well as some MHI companies, have repeatedly asked to discontinue the dual system of financing to eliminate these incentives (FOPH, 2014e).
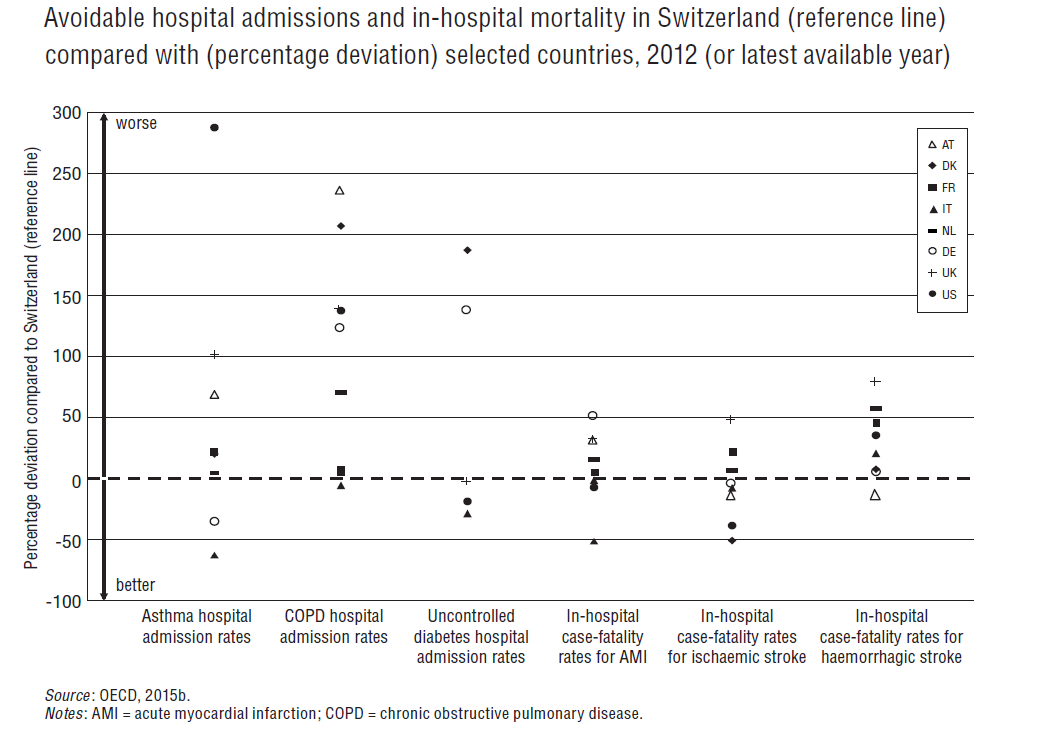
However, expenditure on acute inpatient care is at about the average level of other EU countries (OECD, 2014a); the number of beds per 1000 population has been considerably reduced and is below the EU average (see section 4.1.2); and avoidable hospital admissions are relatively low (see Fig7.9).
Fig7.9
Second, the ambulatory FFS schedule TARMED is outdated and financially awards technical services (mostly of ambulatory specialists) with more money than the non-technical services provided by primary care physicians. This has led to federal intervention amending the fee schedule in favour of primary care physicians (FOPH, 2014l). However, a more permanent solution has to be found by MHI companies and physicians, which are jointly responsible for reforming the fee schedule. Third, the recently introduced SwissDRG-based hospital payment system allows hospital-specific base rates to be negotiated. It is at least conceivable that high base rates are negotiated and approved by cantons for cantonal hospitals even if care could be provided more efficiently in other hospitals (e.g. in other cantons or in private hospitals).
The third point, i.e. the allocation of resources to different types of service, is a particular area of concern in Switzerland, which is reflected in current reform discussions (see section 6.2.1). The existing system of HTA (see section 2.7.1) is often regarded as insufficient, as most new medical services are automatically covered by MHI unless they are challenged by a relevant stakeholder (see section 2.8.1). There is no system of horizon scanning to identify potentially controversial technologies with a high financial impact. This may lead to public resources being spent on services that provide no or very little benefit (Trageser et al., 2012).
In particular, the high availability of medical technology in Switzerland (see section 4.1.3), coupled with the limited development and use of medical guidelines in the country, carries the danger that (supplier-induced) high-technology services are provided when the same result could have been achieved in a more efficient way using less complex services. A systematic analysis of cost-effectiveness of services in the MHI benefits package could potentially improve efficiency in the allocation of resources to different types of services.
7.5.2. Technical efficiency
A recent OECD study shows that Switzerland has the highest prices of health services in Europe (Koechlin et al., 2014). Health services cost more than twice the average price of comparable services in EU countries and hospital services are almost 2.5 times more expensive than the average in the EU (compared to 1.5 times higher prices in the general economy). However, higher prices are not necessarily an indication of technical inefficiencies in the production of health system outputs as they may also reflect differences in input prices and differences in quality. A range of other indicators of technical efficiency are also available for different sectors.
As regards acute hospital care, indicators point in different directions. Average length of stay in Swiss hospitals decreased considerably from 9.3 days in 2000 to 6.5 days in 2011, indicating increased technical efficiency (see section 4.1.2). However, ALOS is still slightly above the average of countries in the EU (6.4 days) and considerably higher than in France (5.1 days) or the Netherlands (5.8 days). The national introduction of DRG-based hospital payment in 2012 puts pressure on hospitals to reduce costs and is expected to contribute to a further reduction of ALOS. Bed occupancy rate in Switzerland (89.1% in 2010) is far above the EU average (75.9% in 2011) and is in fact amongst the highest in Europe, showing that available beds are used efficiently. The number of physicians per 100 discharges is considerably higher in Switzerland (1.5 FTE physicians (FOPH, 2015f)) than, for example, in Germany (0.8 FTE physicians (Destatis, 2013)), which might indicate that human resources could be used more efficiently.
Several other studies have explored potential sources of inefficiencies in the hospital sector (Trageser et al., 2012). In particular, the small size of hospitals in Switzerland has been found to imply considerable room for efficiency improvement as a result of the existence of economies of scale (Farsi & Filippini, 2008). In summary, technical efficiency appears to have improved since the year 2000 but certain (rather rough) indicators suggest there might be further room for improvement.
In ambulatory care, the number of consultations per doctor has been reported to be relatively low in Switzerland (slightly above 1000 in 2007) when compared with other OECD countries (OECD, 2011), such as Germany, the Netherlands and France (all with above 2000 consultations per doctor), although this might, of course, also reflect differences in quality.
A number of Swiss studies have assessed efficiency in ambulatory care by comparing traditional forms of insurance with patients insured under managed care contracts (Trageser et al., 2012; Beck et al., 2011; Reich, Rapold & Flatscher-Thöni, 2012a), where patients are cared for by HMOs or networks of physicians (see also section 5.2.2). Patients insured under managed care contracts were found to have lower costs than patients in traditional insurance. Although earlier studies often did not sufficiently control for the self-selection effect that healthier individuals are more likely to opt for managed care type contracts (Trageser et al., 2012), more recent studies confirmed on the basis of panel data using comprehensive methods of risk adjustment that costs are still lower in managed care type contracts after controlling for the self-selection effect (Beck et al., 2011; Reich, Rapold & Flatscher-Thöni, 2012a). The size of the reduction in costs depends on the type of contract (Reich, Rapold & Flatscher-Thöni, 2012a): patients cared for by a network of physicians who coordinated their care had 15.5% lower costs, while patients insured by networks carrying budget responsibility (e.g. HMOs) had 21.2% lower costs than patients in traditional insurance. This suggests that better coordination of ambulatory care providers could considerably increase efficiency (Trageser et al., 2012).
Prices of pharmaceuticals have reduced considerably in Switzerland since the year 2000, although they remain higher than in Austria, the Netherlands or France (Interpharma, 2014). Several reforms since 2000 have aimed to lower prices of pharmaceuticals (see sections 5.6.4 and 6.1.4). Nevertheless, pharmaceutical spending in Switzerland is considerably above the EU average (OECD, 2014a), and it is increasing (see section 5.6.4). Prices of pharmaceuticals in Switzerland have increased automatically and relatively strongly in international comparison in recent years as a result of devaluation of the euro in relation to the Swiss franc. The current practice of price adjustments after three years means that producers have the chance to benefit from the devaluation for three years before prices in Switzerland are realigned with comparator countries.
In addition, the share of generics in the Swiss pharmaceutical market is relatively small, i.e. 23.9% of the total volume and 18.4% of the total value of reimbursed pharmaceuticals in 2013 (OECD, 2015b). A recent reform in 2012 has attempted to make it more attractive for generic producers to enter the small Swiss pharmaceuticals market. In summary, efficiency in the use of pharmaceuticals has improved considerably but other countries appear to have been even more successful at reducing prices and making more rational use of pharmaceuticals by shifting a larger share of the market to generics.