-
24 March 2025 | Country Update
National dementia strategy: A new approach to care and support
5.1. Public health
At the national level, PHA has overall responsibility for public health. Regions are responsible for primary care, child and maternal care, and youth clinics. Municipalities are responsible for social services and school health services, which are focused on preventive health care and support to students with social and mental health problems. Municipalities also have significant responsibilities in public health outside the health services, such as food control, water and sanitation. In many areas of public health, responsibilities fall within both regional and municipal health care, such as parental support and child rights issues. The regional administrative boards (länsstyrelsen) are the government’s representatives in the regions, ensuring that national goals have an impact in the regions while taking regional conditions into account. These administrative boards are mainly involved in areas concerning social sustainability, such as living habits (see also section 2.5 Intersectorality).
More specifically, PHA is responsible for surveillance and analysis of communicable diseases and the epidemiological situation, as well as contingency planning for outbreaks of infectious diseases. The agency coordinates and monitors the situation nationally, in close collaboration with the Regional Medical Officers of Communicable Disease Control. The 21 infectious control units conduct the operational infection control interventions in the regions by providing support and advice to professionals and the public, and by conducting contact tracing. The basis for surveillance is the registration of around 70 notifiable diseases specified in the Communicable Diseases Act. These pathogens are notifiable to PHA and the Regional Medical Officers by both clinicians and laboratories. Diseases are categorized as generally notifiable (such as malaria and influenza), generally dangerous (for example, diphtheria, hepatitis, gonorrhoea, cholera and HIV infection) and dangerous to the community (ebolavirus, smallpox and severe acute respiratory syndrome). Some diseases are subject to mandatory contact tracing (PHA, 2022b).
The regions organize the screening programmes and are free to decide which screening programmes to implement based on recommendations from NBHW. Screening programmes may therefore differ between regions. Regarding cancer, the recommendation is general screening for breast cancer, cervical cancer and colorectal cancer. All women aged 40–74 years and 23–64 years, respectively, are offered the opportunity to take part in the screening programmes for breast and cervical cancer. A screening programme against colorectal cancer for men and women aged 60–74 years was implemented gradually in all regions during 2021–2022 and full implementation is expected in 2026 (RCC, 2022).
Preventive health care that does not require specialized medical and technical resources is the responsibility of primary care. In most regions, the general vaccination programme, child and maternal health care, and health examinations for asylum seekers are included in primary care. All regions state that the PCCs must work with health promotion and disease prevention initiatives, but some specify services that must be available such as the prescription of physical activity and support to quit smoking (NBHW, 2016). They often refer to NBHW national guidelines (NBHW, 2018a) for prevention and treatment of unhealthy living habits, with guidelines including tobacco use, risky use of alcohol, insufficient physical activity and unhealthy eating habits. However, evaluations have shown large regional differences and that preventive work by PCCs is often not sufficiently prioritized (SOU, 2018:39). Further, the regions have a network supporting their integration of health promotion in regular health services, especially in primary care. It is a part of the International Network of Health Promoting Hospitals and Health Services (HPH).
Various nongovernmental organizations also contribute to important public health work. The sports movement has an important role and is to some extent financed by targeted grants from the national government budget, but mostly dependent on voluntary contributions and participation from hundreds of thousands of citizens.
Employers have an obligation to ensure that occupational health care is available in terms of both physical and mental services to employees. Occupational health covers approximately 60% of all employees and is financed by the employer (Swedish Work Environment Authority, 2020). The most common arrangement is that occupational health supports in health promotion, preventive work and work-oriented rehabilitation.
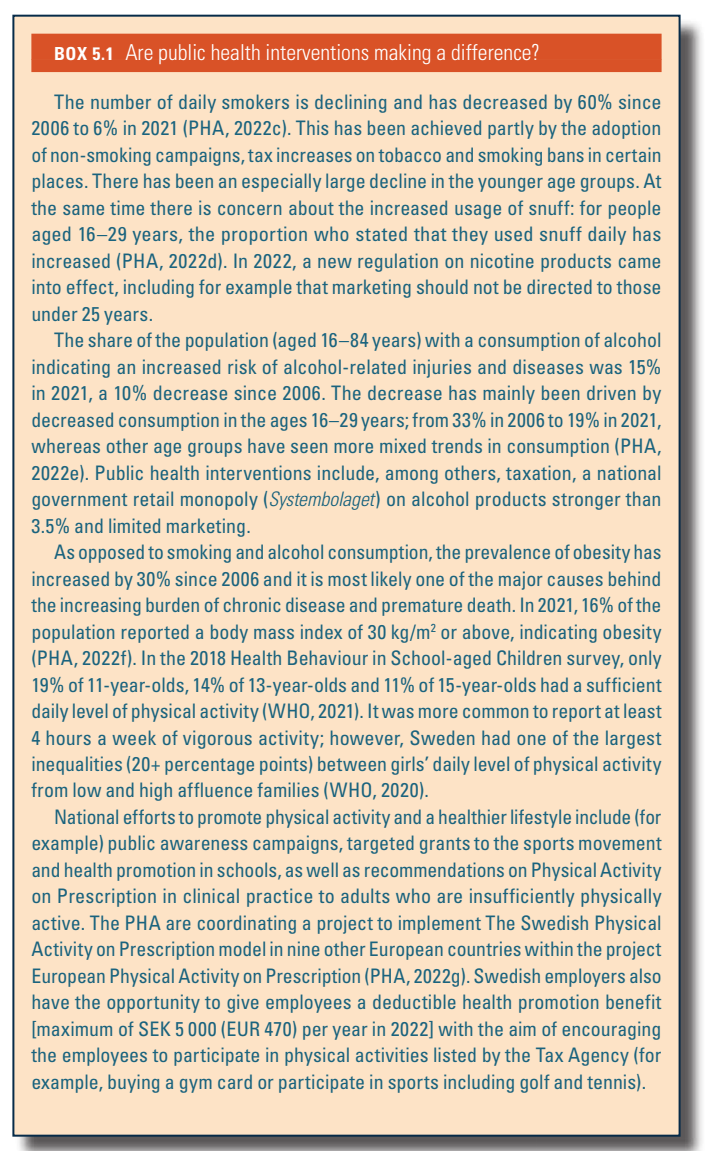
Box5.1 provides the assessment of the effectiveness of public health interventions in Sweden.
Box5.1
Dementia is a major public health challenge. The number of people in Sweden living with the condition is steadily rising, putting pressure on healthcare systems. At the same time, research on dementia diagnosis and risk reduction is advancing rapidly.
In response, the Swedish government announced an updated national dementia strategy on 23 January 2025, covering healthcare, dental care and social services. The strategy is based on two key principles:
- Dementia is not a normal part of ageing; young people are also affected, and new knowledge must be integrated into healthcare.
- People with dementia should be able to live dignified, meaningful lives, with access to proper support and care.
The strategy introduces four healthcare goals:
- Interventions should be tailored to individuals’ needs.
- Efforts must be coordinated, promote health and prevent illness.
- Care should be evidence-based.
- Relatives must receive adequate support for sustainable family caregiving.