-
23 March 2023 | Country Update
The government introduces performance-based payment to the regions to increase the number of care places
4.1. Physical resources
The number of care places per capita has decreased continuously in recent decades in Sweden, as well as in other high-income countries. Between 2010 and 2020, the number of care places decreased from 2.7 to 2.1 per 1000 inhabitants. In 2021, there were on average just over 17 500 disposable care places in Sweden, of which 80% were within somatic inpatient specialized care. At the same time, the number of overcrowding and displaced patients in somatic care has increased. In December 2022, there were an average of 8.8 overoccupancies and 2.9 relocations per 100 available care places in the country’s hospitals. However, the regional differences are large.
The government recognized the need to increase the number of care places within the health care system and decided on 17 February 2023 to give the National Board of Health and Welfare the task of distributing close to SEK 2 billion in performance-based payments to the regions to increase the number of care places. The National Board of Health and Welfare is also tasked with developing proposals for a national plan to reduce the shortage of available care places. The assignments aim to strengthen all hospital care and that more disposable care places should be created where they are most efficient in order to strengthen patient safety.
Authors
4.1.1. Capital stock and investments
There is a mix of publicly and privately owned health care facilities in Sweden, but they are generally publicly funded. Highly specialized care, requiring the most advanced technical equipment, is concentrated in seven (public) university hospitals located in Malmö/Lund, Gothenburg, Linkoping, Stockholm (Huddinge), Uppsala, Umeå and Örebro. There are also about 70 public hospitals at the county level, 6 private hospitals and over 1100 public and private primary care units throughout the country.
Capital investments are generally decided upon and funded by the local county councils. With a few exceptions, there have been no investments in new hospital buildings since 1980 until the past few years when several new hospital buildings have been planned and built. The rapid pace of capital investments in health care during the 1960s and 1970s declined in the 1980s. One explanation for this decline was that the expansion phase up to the 1970s led to mature health care infrastructure in the 1980s. Then, in the 1990s, the psychiatric and the ÄDEL reforms transferred the responsibility and provision of care for a large proportion of patients from the inpatient hospital setting to the outpatient care setting and the municipalities. Facilities are generally well maintained although the buildings in many cases are more than 20 years old.
Currently, instead of fixing poorly maintained buildings, hospital buildings are being planned and built to meet changes in health care demands and structures in the provision of health care, such as more outpatient care and day care. In several cases, it would be more expensive to keep rebuilding and renovating existing buildings to meet the demands for new forms of care than to build new ones (Lövtrup, 2011). The largest ongoing investment is the building of a new Karolinska hospital in Stockholm, estimated at SEK 14.1 billion (€1.6 billion), which should be finalized in 2016. The project is financed through a public–private partnership between the Stockholm county council and the company Swedish Hospital Partners AB, owned by the Swedish construction company Skanska Infrastructure Development and the British investment fund Innisfree.
4.1.2. Infrastructure
There were about 25 500 hospital beds in Swedish hospitals in 2009, with slightly more than 4400 in specialized psychiatric care and about 20 000 in specialized somatic care in public hospitals (Fig4.1) and about 1100 in private hospitals. At the end of the 1960s, there were about 120 000 hospital beds. There has been a continuous decrease in the number of hospital beds since the 1970s. Structural changes continued in the 1990s, with a shift from hospital inpatient care towards outpatient care and primary care, and when the municipalities took over the responsibility for long-term care in 1992 in connection with the ÄDEL reform. The number of hospital beds was 50 000 after the ÄDEL reform.
Fig4.1

The decrease in hospital beds has continued during the 2000s but at a slower pace. Structural changes in the 2000s have focused more on the concentration of highly specialized care and a division between emergency care and other care. The reduction in beds during the period 2005–2009 has primarily been in beds for somatic care, whereas the number of psychiatric beds has remained fairly stable and has even increased slightly since 2007 (SALAR, 2010a; National Board of Health and Welfare, 2010e).
The ALOS was 4.6 days per episode of care in 2008, which is a decrease of 0.4 days since 1998 (National Board of Health & Welfare, 2010b). Diseases of the circulatory system accounted for 18% of all episodes of care and are thereby the largest organ-specific group. The ALOS differs between county councils from 3.9 days in Dalarna to 5.7 days in Blekinge. In comparison with other countries the ALOS in acute care hospitals is lower in Sweden compared to the United Kingdom but higher than in Norway and Denmark (Fig4.2). The number of inpatient surgical procedures is also lower in Sweden than the EU average.
Fig4.2
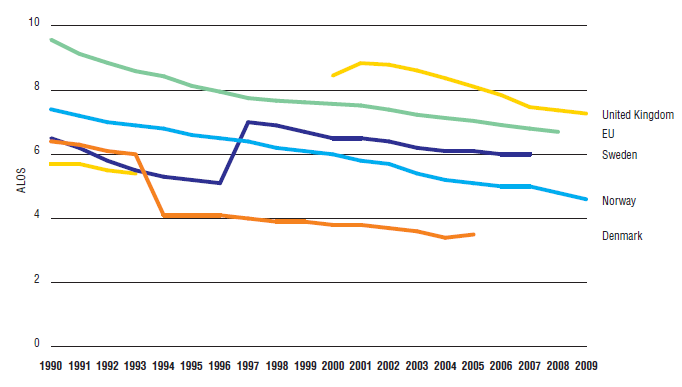
Since an increasingly large proportion of care is provided in the outpatient setting, it is not anticipated that the ALOS for care episodes in the inpatient setting will continue to decrease. Approximately 560 000 day cases of surgery were produced in 2008. The number of day cases as a percentage of all care episodes (inpatient and outpatient) was almost 30% in 2008. Most day cases of surgery involve surgery of the skin and cataract surgery. Cataract surgeries are almost exclusively performed in the outpatient setting (day surgery). Also, this proportion differs between county councils. The highest proportion of day cases can be found in Blekinge, Halland, Skåne and Stockholm, in that order (National Board of Health and Welfare, 2010b).
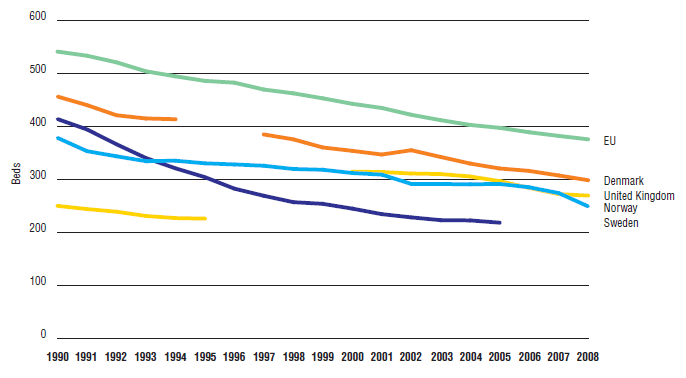
The number of beds in acute hospitals per inhabitant has decreased since the early 1900s in Sweden. The total number of beds in acute hospitals was reduced by almost 50% between 1990 and 2005 (Fig4.3). There have also been similar structural changes in the other Nordic countries, but the reduction has been more prominent in Sweden and the number of beds in acute hospitals in Sweden is lower than in Denmark and Norway and compared to the EU average.
Fig4.3
4.1.3. Medical equipment
There are no national up-to-date statistics available regarding items of functioning diagnostic imaging technologies (e.g. MRI, CT, PET) per 1000 population. Nonetheless, the adoption and use of medical technologies, including new medical equipment, is high in Sweden. According to a report by the Swedish Council on Technology Assessment in Health Care (2001) all university hospitals, most county council hospitals and several primary care facilities had MRI equipment in 2001.
4.1.4. Information technology
Access to, and use of computers and the Internet is high amongst the Swedish population. More than 90% of the population had access to the Internet in their home in 2010. Among companies, almost 100% of those employing at least 10 people have access to the Internet.
Regarding health information, all county councils and most hospitals and primary care facilities have web pages where information (publicly and privately provided) about health care services can be found (see sections 2.7.1 Information systems and 2.9.1 Patient information). These pages contain information about where to seek care in the event of ill health or injury, and about the different hospitals and health care facilities that are available. There is also a national publicly initiated collaborative project led by the SALAR (www.1177.se) and a privately initiated project led by the Confederation of Swedish Enterprise (www.omvard.se) where comparative information about health care providers is disseminated through the Internet (see section 2.9.1 Patient information).
Several different IT systems operate in the Swedish health care sector (see section 2.7.1 Information systems). Generally, both the quality of such systems and their levels of use in hospitals and primary health care facilities are high. Usually patients’ records are kept electronically. More than 90% of primary care providers use electronic patient records for diagnostic data (Health Consumer Powerhouse, 2009). Also, the use of e-prescriptions is becoming increasingly common and in 2009 more than half of all Swedish prescriptions were e-prescriptions (Health Consumer Powerhouse, 2009).
It is up to every hospital to select and procure its own preferred IT system. In several county councils, efforts are made towards harmonizing patients’ records across all hospitals in the county. There are also ongoing projects at the national level, aimed at integrating (and making compatible) the various information systems used, with the purpose of increasing the security and effectiveness within the systems. These projects have been initiated as a result of concern about the fragmentation of IT systems in Swedish health care (see chapter 6).