-
09 October 2025 | Country Update
Visual aids for refractive conditions: Expansion of coverage scope for children in Spain -
01 July 2024 | Country Update
New benefits in the SNS portfolio
3.3. Overview of the statutory financing system
3.3.1. Coverage
Breadth: who is covered?
Between 2012 and 2017 the right to health care was linked to the legal and employment status of individuals (Bernal-Delgado et al., 2018). In 2018, the Spanish Parliament approved a reform whereby the basis for entitlement returned to the condition of residence, which had been the case before 2012 (Royal Decree-Law 7/2018). Under the new law, undocumented migrants regained eligibility to full coverage like any other Spanish national. Public insurance is compulsory (individuals cannot opt out).
Scope: what is covered?
Royal Decree-Law 16/2012 regulates the benefits package provided by the SNS with a view to define what benefits should be co-financed by patients. Two categories of services were defined: the common package with three subcategories – basic package, supplementary package and accessory services – common to the 17 RHSs composing the SNS, and the complementary package, decided under the rule of the ACs (see section 2.7.3 Regulation of services and goods).
The SNS basic benefits package includes all health care prevention, diagnosis, treatment and rehabilitation services, as well as emergency medical transportation. Hence, the basic package includes a comprehensive basket of PHC benefits (for example, acute and chronic care, health promotion and disease prevention activities, physiotherapy, mother and child care, mental health care, palliative care, medical counselling, basic dental health services, etc.) and specialized health care benefits (for example, any diagnostic and therapeutic procedure to be provided as outpatient specialized care, inpatient acute or long-term care, day care surgical or medical care, palliative care, acute or long-term mental health care, home care, organ transplants, emergency care, etc.). The supplementary package essentially includes pharmaceutical prescriptions and orthoses and orthopaedic devices (Ministry of Health, 2023h). The accessory package has been vaguely described in Royal Decree-Law 16/2012 as all activities, services or techniques, without benefit, that are not considered essential and/or are used as aid-devices for chronic care improvement (Royal Decree-Law 16/2012). This third package, born in times of austerity, was, arguably, a category for broader exclusions from public financing, which were not activated. To date (June 2024), no related regulations have been issued.
Finally, there is a complementary package: ACs may incorporate into their own benefits package any technique, technology or procedure not covered by the common package of the SNS. For an AC to cover these complementary services, it must ensure financial sufficiency and meeting budget stability criteria; it must also inform the CISNS (Article 2, Royal Decree Law 16/2012).
The draft Law on the Universality of the National Health System is currently being debated in Parliament (June 2024). This law seeks to restore the benefits package as a single portfolio (see section 6.2 Future developments).
Depth: how much of the cost is covered?
The benefits in the common basic package are not subject to any patient cost-sharing. Instead, pharmaceutical prescriptions and orthoprosthetic devices under the supplementary common package are subject to co-payments. Royal Decree-Law 16/2012 indicates that co-payments must be set on the final product price and be fixed according to annual household income and a maximum ceiling of monthly payments (see section 3.4 Out-of-pocket payments and Table3.3). The accessory services (when regulations are issued following approval of the new draft law on the benefits package) should be subject to the same cost-sharing scheme.
Table3.3

Finally, in the case of the complementary package of services, funding is decided at ACs level, but the effective adoption of those new benefits is conditional on ACs’ capacity to pay for them.
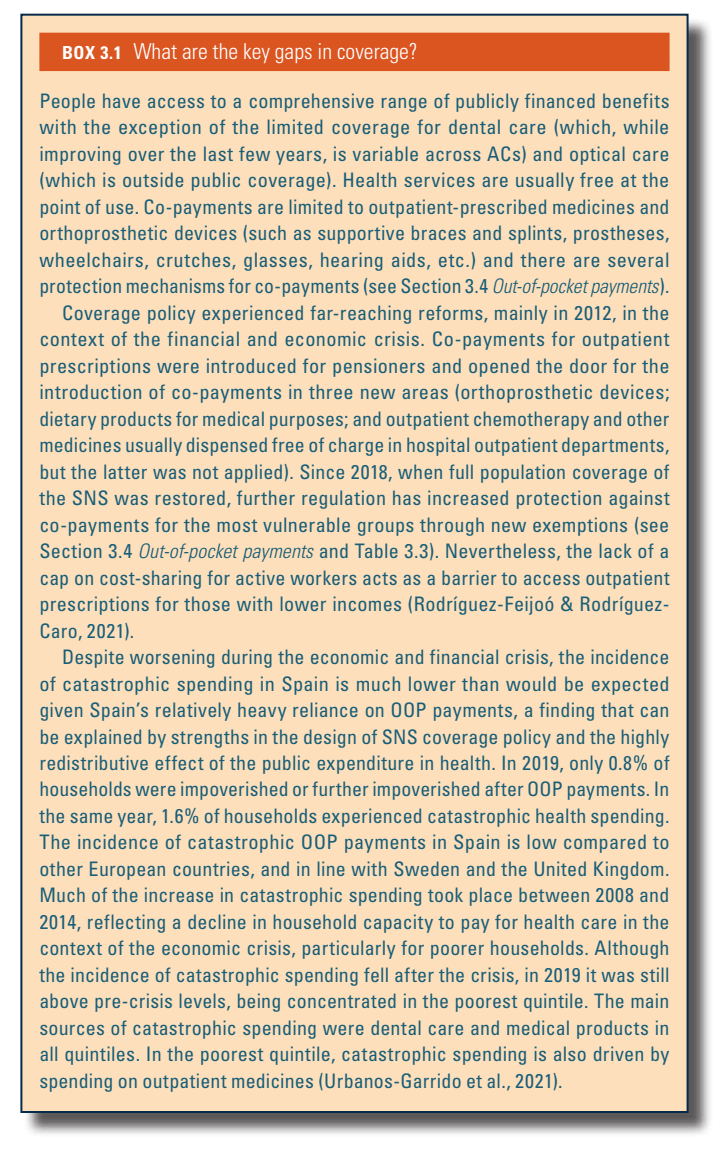
Box3.1 provides an overall assessment of what the key gaps are in the breadth, scope and depth of coverage of the statutory system in Spain.
Box3.1
References
3.3.2. Collection
General government budget
The vast majority of public expenditure on health in Spain is funded through general taxation (see section 3.2 Sources of revenue and financial flows). The Spanish tax system is highly decentralized. The current regional financial scheme came into force in 2011 after approval in 2009 (Organic Law 3/2009 and Law 22/2009), and it is based on a combination of own taxes, participation in general taxes and transfers for the majority of regions, ruled by the so-called “Common Regime model”,[10] where the responsibility for tax collection is shared by the Spanish Fiscal Revenue Agency (Agencia Estatal de Administración Tributaria, AEAT) and the regional financial authorities.
Leaving aside social security contributions (which are earmarked for pensions and other monetary benefits), the system tax revenues come both from taxes linked to production and imports (“indirect taxes”, such as VAT) and “direct taxes”, that is, taxes on income and wealth. ACs are also responsible for the collection of those taxes assigned to the regional level (inheritance taxes, wealth transfer taxes) and share tax collection for VAT, personal income tax and excise taxes. In the year 2022, tax revenues amounted to €255 463 million. Direct taxes amounted to €145 121 million (56.8% of the total), with income tax being the most relevant, with €109 485 million in revenue (75% of total direct taxes). Indirect taxes collected €108 480 million (42.5% of the total), with VAT being the most relevant figure (€82 595 million), followed by special taxes (€20 224 million) (AEAT, 2022).
Taxes, contributions or premiums pooled by a separate agency
The second statutory health care system, the Mutual Funds (MUFACE, MUGEJU and ISFAS) (see section 2.2 Organization), is partly funded by the contributions of their affiliates. The contribution rates are set by the central government in the general budget law each year. Currently, Mutual Funds public employees pay a monthly premium between €20 and €50 (note that this amount is for the policyholder, irrespective of the beneficiaries), according to their professional category (a total of six groups or levels exist among the civil servants), which covers up to 15% of the overall expenditure; the remaining 85% is covered from the budget of the Ministry of Finance, which collects funds from income tax revenues, mainly (Ministry of Defence, 2023; Ministry of Justice, 2022; Ministry of Treasury, 2023).
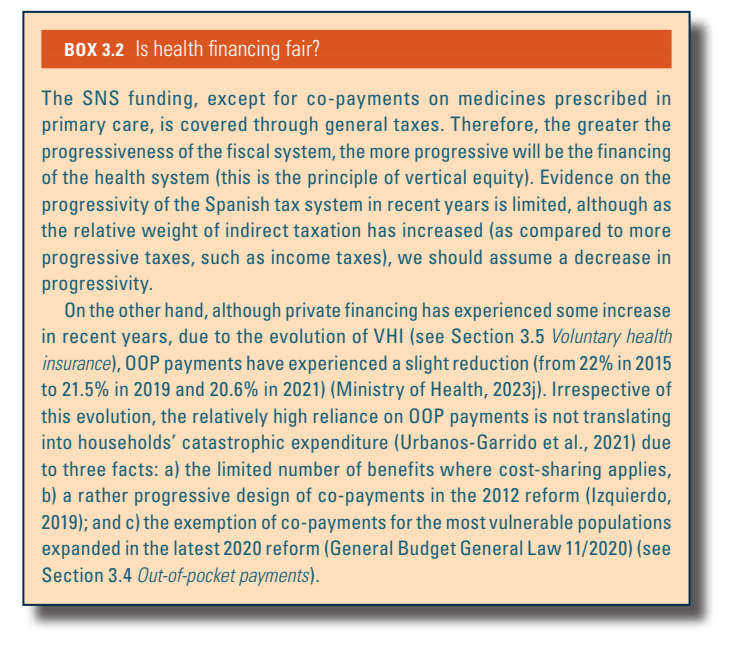
See Box3.2 on the fairness of health financing in Spain.
Box3.2
- 10. Two ACs, the Basque Country and Navarre, enjoy a special financial regime based on particular legislation (namely, “derechos forales”), acknowledged in the Spanish Constitution. By virtue of this specific legislation, regional authorities collect all the taxes levied in their corresponding territories, and then reimburse the central government for the services that the latter provides to the citizens of those regions (that is, non-devolved services, as for example, national defence). ↰
3.3.3. Pooling and allocation of funds
Allocation from collection agencies to pooling agencies
[11]
Regional public services including health care are funded after fiscal revenues collection using a complex system of transfers seeking the reduction of funding imbalances across ACs (see section 3.2 Sources of revenue and financial flows). Thus, three main allocation mechanisms coexist; a) the Guarantee of Basic Public Services Fund (Fondo de Garantía de Servicios Públicos Fundamentales, FGSPF), intended to ensure equal funding for equal needs for basic services (health, education and social services); b) the Global Sufficiency Fund, covering the gap between expenditure needs for each AC and the resources provided by the FGSPF and regional fiscal capacity; and c) the so-called “convergence” funds (namely, Competitiveness, Cooperation and Inter-territorial Compensation funds), which try to reduce economic imbalances across ACs.
The FGSPF is allocated to the ACs according to a needs-based weighted formula. This formula includes the size of the population to be served (weighting 30% in the formula), the age-weighted population covered by the SNS (38%), the population aged 16 and younger (20.5%) and the population aged 65 and over (8.5%), and several structural factors such as geographical extension (1.8%), population density (1.6%) and insularity (0.6%). It is funded with 75% of the tax revenues corresponding to the ACs and a contribution from the central government (Treasury Department, 2024).
The Fund for Global Sufficiency covers public spending needs (including health care) when the sum of the ACs’ own fiscal revenues and the FGSPF fall short. This Fund is calculated according to the actual health expenditure of the AC and will be negative in those ACs (typically, high-income regions) where transfers from the FGSPF and regional tax revenues exceed the financial needs for the AC. The negative amount will be deducted from the regional participation in central taxes the following year.
Additionally, some regions still receive transfers from the ACs’ Financing Fund, established in 2014 and comprising the Liquidity Funds which were set up in 2012 as extraordinary funding instruments during the economic and financial crisis. The Financing Fund currently includes: a) the Autonomous Liquidity Fund (Fondo de Liquidez Autonómico), consisting of loans from the central government to prevent regions from resorting to debt markets; b) the Financial Facility Fund, aimed at refinancing regional debt; and c) the REACT-EU Liquidity Fund, which channels aid from the Next Generation funds and was implemented in 2020 in the context of the governmental response to the COVID-19 pandemic, with a view to protect public services and reactivate the economy (Ministry of Finance, 2020).
Finally, the compensation funds are mainly a) the Healthcare Guarantee Fund, managed by the Ministry of Health, aiming at covering assistance provided in a particular AC to those citizens residing in a different AC; this Fund is extra-budgetary, and has partially compensated expenses in primary care and pharmaceutical expenses in prescriptions (Resolution of 17 November 2020); and b) the Healthcare Cohesion Fund, funded by the Ministry of Health, with a similar aim but restricted to the so-called Reference Centres, Services and Units, in charge of providing highly specialized care or rare diseases care for patients from any AC, and then requiring the concentration of a minimum number of patients (Royal Decree 1302/2006); this fund is no longer extra-budgetary since 2021.
Allocating resources to purchasers
In the case of ACs, once the regional budget allocation is endorsed by the regional parliament, the third-party budget-setting and split-purchasing role is played by the health departments in the 17 ACs (and INGESA for the autonomous cities of Ceuta and Melilla; see section 2.2 Organization) which “purchase” services from either public or private providers for all the residents in the AC. In the case of civil servants, the Mutual Funds, which receive the corresponding share of the budget (as well as the affiliates’ contributions), purchase services from both private and public providers, depending on the decision of their affiliates, who generally opt for either type of provider on a yearly basis.
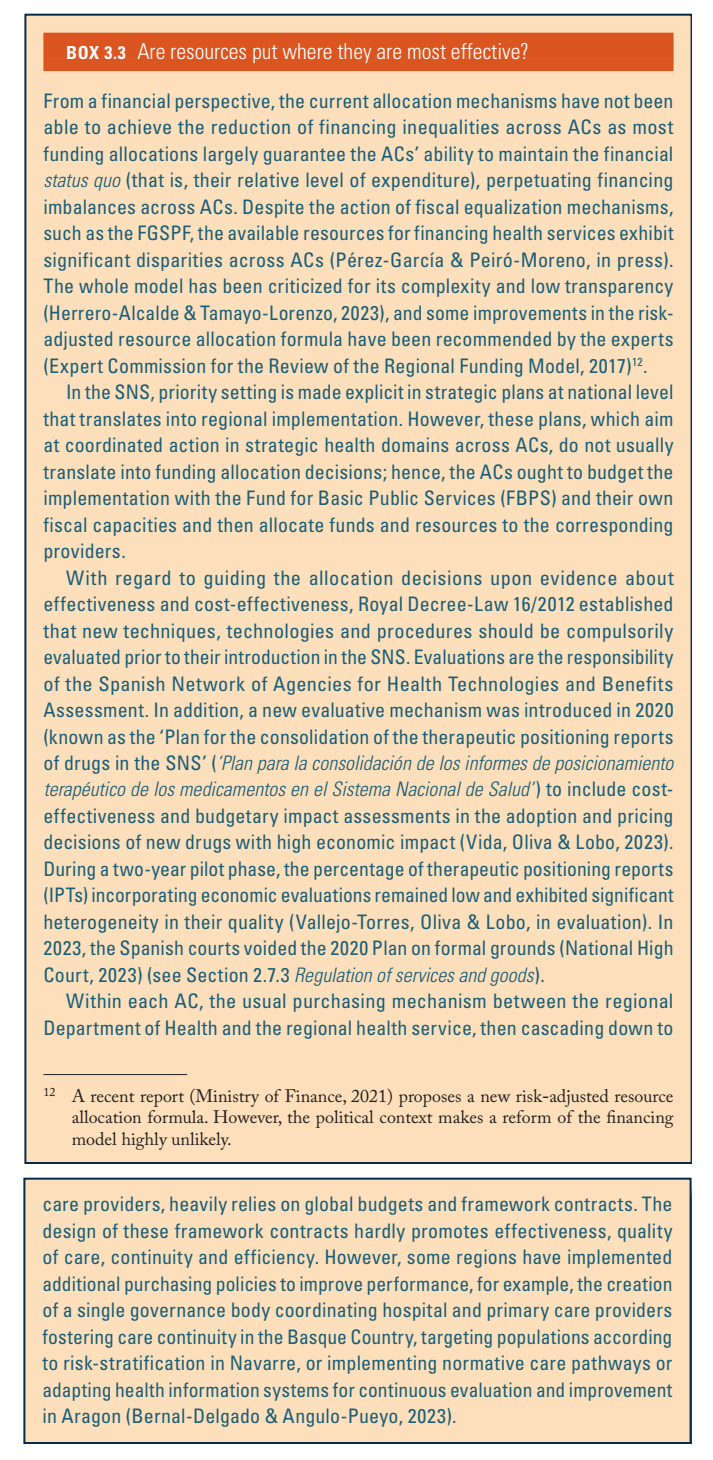
See Box3.3 on the Spanish health system’s allocative efficiency.
Box3.3
- 11. Note that this allocation to pooling agencies section refers to the “Common Regime of the ACs”, which includes all ACs except the Basque Country and Navarre, as they enjoy a different financial regime in which they collect all the taxes levied in their corresponding territory and make their allocation decisions in the corresponding regional parliament. This section also does not address the Mutual Funds for civil servants for which funding is allocated as part of the central government budgeting decisions. ↰
3.3.4. Purchasing and purchaser–provider relations
Public provision in the SNS plays a prominent role and, in general, the public bodies in charge of purchasing (that is, the ACs’ health departments) purchase the services from another public body, hierarchically linked to the former, the so-called RHS. The latter runs all inpatient and outpatient health care centres. Generally, the health department annually “contracts” (and budgets) the services with the RHS that, in turn, negotiates global annual contracts with its providers. Additionally, either the ACs’ health departments or the RHSs may contract services from private providers, usually from hospitals or diagnostic laboratories.
Within this general scheme, RHSs contract hospital care, primary care, preventive activities and long-term care services. Public hospitals are financed through global budgets, mainly considering the actual expenditure in the previous year, although some adjustment to quality and new services may be used. In turn, primary care services are contracted upon a global budget for acute, chronic and preventive care services, slightly nuanced according to population demographics and dispersion. The primary care “contract” reflects specific objectives prioritizing certain care or preventive programmes, and includes some incentives linked to the achievement of certain prescription targets aimed at increasing the appropriate use of drugs. There are a few exceptions to this model: a) the externalization of primary care by way of the so-called EBAS (Entidades de Base Asociativa) in the AC of Catalonia, which are limited societies of primary care practitioners that provide care to a defined population according to a contract with the Health Department (since 1996, only 11 EBAS have been created in Catalonia, a model that seems self-limited in its ability to generalize); and b) primary care provided in the context of a P-PP in the region of Valencia (see section 2.7.2 Regulation and governance of provision).
In addition to public providers, a certain amount of activity is contracted out to private providers, typically aimed at reducing waiting lists for surgical procedures or high-technology diagnostic tests, but also to complement long-term care services and palliative care, among others. These are generally prospective volume-contracts with some ex-post correction clauses. Depending on the nature of the activity, the public purchaser determines the basis for payment; hence, long-term care activity is usually financed in terms of stays, whereas surgical interventions and diagnostic tests follow a fee-for-service (FFS) scheme based on a public tariff. Contracts with private providers have been observed to increase since the mid-1990s; in 2020, they accounted for 10% of the total public health expenditure (Ministry of Health, 2023i).
References
More information (in Spanish):
Order SND/606/2024 https://www.boe.es/diario_boe/txt.php?id=BOE-A-2024-12290