-
24 May 2025 | Country Update
Civil servant mutualities under scrutiny
7.6. Health system efficiency
Despite the efforts made to improve efficiency, academic and political actors recognize the lack of systematic and comprehensive studies evaluating the efficiency of the health system and public policies, and the need to create a dedicated and independent national agency for the evaluation of the health system (AES, 2014, 2020; Vida, Oliva & Lobo, 2023; Spanish Socialist Workers’ Party, 2023; Popular Party, 2023).
The Independent Authority for Fiscal Responsibility (AIReF), an autonomous public institution tasked with ensuring the sustainability of public finances and promoting transparency and fiscal discipline across all levels of government, has published a pioneering study on Spain’s civil servant mutual insurance system, evaluating its effectiveness, efficiency, and equity. The analysis draws on 400 million anonymized microdata and a survey of 16,000 mutualists, combining administrative records, hospital activity, pharmaceutical use, and healthcare data.
Spain stands out as a unique case among peer countries, as it is the only country with universal coverage and tax-funded healthcare that sustains a mutual insurance system. The report finds a strong link between mutualists’ care preferences and the complexity of the required treatment. While only 24% of mutualists chose public provision overall, this rises to 70% in severe hospital cases. In turn, private healthcare offers better accessibility but higher pharmaceutical costs. Mandatory affiliation under the current framework limits access – especially for those choosing the private model – to the universal features of public provision available to other citizens. AIReF proposes transitioning to voluntary enrollment and integrating new mutualists into the NHS.
7.6.1. Allocative efficiency
Macro level
There are three main policy instruments in Spain supporting allocative efficiency at the macro level: 1) the financing mechanism of the ACs whose main goal is the even financing of welfare state services (that is, health, education and social services) across the country; 2) a policy design towards UHC; and 3) guidance on the adoption of new technologies.
1. AC financing mechanism. Health services (as well as education and social services) are mainly funded with resources from the Fund for Basic Public Services (FBPS). This Fund represents 75% of ACs’ aggregated fiscal resources and seeks to evenly provide sufficient funding to the ACs according to a formula of “weighted need” (see section 3.3.3 Pooling and allocation of funds). This Fund is complemented with a general fund, the Fund for Global Sufficiency (FGS), which largely guarantees the financial status quo of the ACs according to the relative level of expenditure at the time of the decentralization of health care competences in 2001 (see García-Armesto et al., 2010). Unfortunately, this second mechanism has largely hampered the reallocation of funds across ACs, as it has de facto perpetuated financing imbalances across ACs, and is not driven by differences in need.
2. Policy design towards universal health coverage. Since 2018, several policies have been introduced to reduce gaps and aim for full UHC. The most important reforms have been: a) returning to residence status as the basis of entitlement (see section 3.3.1 Coverage and Chapter 6); b) expanding some benefits (see sections 2.7.5 Regulation of medical equipment, devices and aids and 7.2 Accessibility); and c) the extension of co-payment exemptions to people benefiting from the guaranteed minimum income scheme, to pensioners with low incomes, to moderately and severely disabled children and to households receiving child benefits (see section 3.4 Out-of-pocket payments). However, some gaps in the achievement of full UHC remain (see section 7.2 Accessibility).
3. Guidance for the adoption of new technologies. Although cost-effectiveness is required by law as a main point when making decisions on resource allocation, few steps have been taken to include efficiency in the decision-making equation. It is worth highlighting the role of the Spanish Network of Agencies for Health Technologies and Benefits Assessment that, within its current mandate, has reviewed the value of existing benefits, has designed and coordinated ad hoc evaluative studies for the adoption of new technologies (except for drugs that are a competence of AEMPS), and has standardized methodologies for HTA evaluation (RedETS, 2023).
This approach has indeed superseded the classical priority-setting mechanism based on health strategies or general plans – inspirational documents whose recommendations were not always based on effectiveness. In the case of pharmaceuticals, VALTERMED has become an instrument for the evaluation of health outcomes in drugs with a high economic impact (Ministry of Health, 2021a). These evaluations are used to inform decisions about pharmaceutical provision during the different stages of the drug cycle. In 2020, the SNS Drug Evaluation Network (REvalMed) was launched, heading to the inclusion of economic evaluation criteria in the so-called “therapeutic positioning reports (IPT)” aiming to inform decisions on drug pricing and reimbursement. Unfortunately, the economic evaluation in these reports was declared null by the National Court in July 2023 following a successful lawsuit filed by the Spanish Association of the Pharmaceutical Industry (see section 2.7.3 Regulation of services and goods).
Spanish independent bodies, such as the National Commission for Markets and Competition, highlighted in 2022 the inadequacies of economic evaluation in funding and pricing decisions, and recommended its incorporation into the IPT (CNMC, 2022). Along the same lines, AIReF, especially in its first review of public spending on medicines, recommended applying “binding” cost-effectiveness criteria “systematically” to decisions on the pricing and public financing of medicines (AIReF, 2019). These reports, among others, have led an academic debate on the actual impact of these instruments on achieving allocative efficiency; for example, the analysis of the governance of new technologies assessment instruments based on other countries’ experiences has backed the debate on the need for an independent assessment body (Vida, Oliva & Lobo, 2023).
Meso level
Once funds arrive at each AC, the corresponding regional parliament approves the budget for the Department of Health, with this resource allocation generally relying on previous expenditure. Then, the Department of Health and the RHSs allocate funds through the purchase of services to mostly public providers by using global budgeting. Global budgeting covers PCCs and hospitals providing primary, as well as hospital, emergency and pharmaceutical care for all residents in a health care area. Purchasing is operationalized through framework agreements that include the global budget for the year, estimated from actual expenditures incurred during the previous year, which are paid retrospectively. Framework agreements broadly specify the volume of services to be provided, as well as some quality and efficiency goals. Payroll costs, any reward to the centres or individuals (if it exists, it tends to be small), ancillary services and maintenance and investments are included in the global budget.
A variety of purchasing instruments in addition to global budgeting have had to be implemented to enhance allocative efficiency, while producing good health outcomes. Some notable examples include: the creation of governance bodies integrating the continuum of care, such as the integrated health organizations in the Basque Country (Organizaciones Sanitarias Integradas); the use of population or patient risk stratification estimates in the allocation of funds; the development and inclusion of new roles and skill shifting, effectively allowing case-management or disease-management approaches; and the purchase of normative care pathways, providing guidance about which services to purchase (that is, highly effective procedures) and from whom (that is, which care professional) (Bernal-Delgado & Angulo-Pueyo, 2023).
Unfortunately, there are no formal evaluations, either at macro or meso level, that could provide guidance on how to improve allocative efficiency.
7.6.2. Technical efficiency
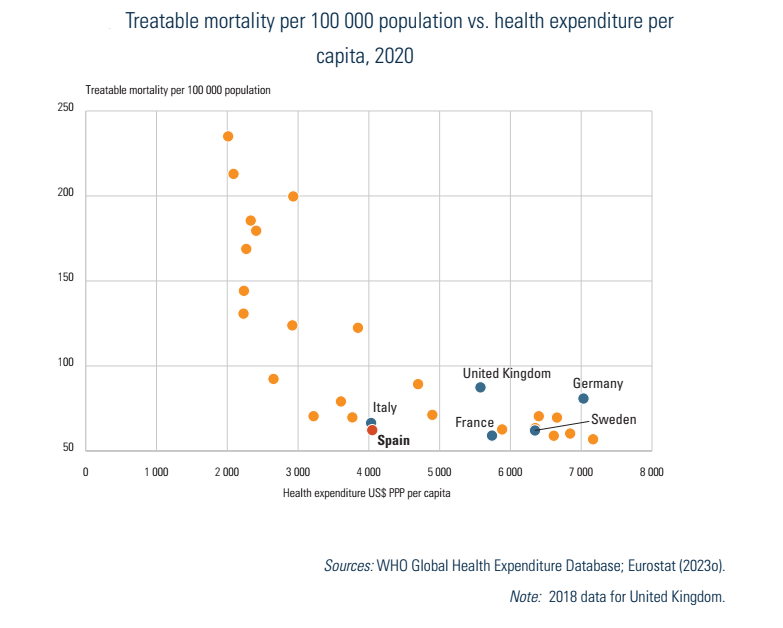
One way to provide a very cursory illustration of how the health system is performing in terms of input costs and outcomes is to plot current expenditure on health against the treatable mortality rate. Although we must be mindful that it is not possible to effectively disentangle the role of health behaviours and other determinants of the health care system in influencing the level of mortality due to treatable causes, Fig7.8 provides a useful entry point for discussion. As mentioned in section 7.5, Spain’s treatable mortality rate is among the lowest in the EU, at 63 per 100 000 inhabitants in 2020 – in line with France (60) and Sweden (62). Additionally, in 2020, health expenditure per capita was notably lower in Spain than in either France or Sweden, despite the exceptional increase of public funds dedicated to address the needs arising from the COVID-19 pandemic (see section 3.1 Health expenditure). These basic results suggest that given its expenditure levels, Spain has been able to secure very good and efficient outcomes on this metric.
Fig7.8
Moreover, in an OECD report analysing how the institutional design of health systems gets value for money (in other words, countries’ expenditure against health outcomes), Spain’s SNS achieves strong results for technical efficiency (Lorenzoni et al., 2018). Among the report findings, factors that could explain SNS technical efficiency are: a) the strong regulation of medical staff in hospitals, with a physician workforce that enters the health system through the national residency programme (see section 4.2 Human resources); b) the existence of a clear benefits package, regulated by law and with a clear governance mechanism for its update (see section 2.7.3 Regulation of services and goods); c) the strict regulation of salaries that translates into a restrained growth of the public budget (salaries represent 57% of hospital expenditure and 84% of primary care expenditure) (Ministry of Health, 2023f); d) effective access to the extensive benefits, equal to all citizens (see section 3.3.1 Coverage); and e) the high level of financial protection for health care users (see section 7.3 Financial protection).
Other factors that may explain technical efficiency in the SNS are: a) the strong gatekeeping system (except in the case of access to hospital emergency wards and Mutuality Funds whose beneficiaries may opt for direct access to specialized care) that translates into a truly principal-agent relationship, where a highly qualified family doctor makes decisions on the best course of action for a particular patient; b) the administrative distribution of the population into health care areas, along with a strongly hierarchical organization mainly based on public providers, which greatly reduces coordination costs; and, c) although with some flaws, the strong centralized regulation of drug pricing, as well as some long-standing policies on reference prices, prescription by active ingredient and dispensation of generic drugs (Bernal-Delgado et al., 2018), which has dragged down unit prices of pharmaceuticals to be among the lowest in the EU.
7.6.3. Gaps in technical efficiency
Despite these good indications of technical efficiency, decisive improvements could be made in a number of areas, notably in human resources and the adequate use of treatments.
Human resources
In addition to the already mentioned imbalance between the numbers of doctors and staff nurses (see section 4.2 Human resources), there is a need for professions that are better equipped to meet population needs in the upcoming decades. Notably, the current deficit of specialists in family and community medicine, which is expected to worsen in the upcoming years (Barber-Pérez & González López-Valcárcel, 2022), may put at stake the SNS approach to care continuity. Moreover, there is a need for new roles, such as disease consultants, hospital-liaison nurses, case-management nurses in primary care, community-liaison nurses and health counsellor nurses, while the inclusion of physiotherapists and social workers in primary care has been shown to be a clear asset to improve quality in the provision of chronic care (Bernal-Delgado & Angulo-Pueyo, 2023). Physiotherapists are notably underrepresented within the SNS; although in general terms the number of registered physiotherapists per 100 000 population is close to the EU average (Eurostat, 2023v), just 10% of physiotherapists in Spain have a position in the public system (Europapress, 2023). The sectoral trade union of nurses, SATSE and the College of Physiotherapists has recurrently highlighted the need for the inclusion of more physiotherapists in the SNS, alleging important cost savings (€4800 million annually) in terms of preventing the use of more complex specialized services and sick leave days (Europapress, 2023).
On a different note, the development of subspecialties and clinical units focused on specific technologies and procedures, which some argue are key to obtaining the required expertise, may in turn hinder technical efficiency in the absence of population planning for highly specialized services; indeed, the growth of medical staff in hospitals can be inefficient if it does not fully match the appropriate population demand for these subspecialties.
There is one specific case worth differentiating: mental health care. In a nutshell, in Spain more than one in six people had a mental health issue in 2019. The most common mental health issues in Spain are depression and anxiety, and Spain was the second largest consumer of prescribed anxiolytics in the EU in 2021 (OECD/European Observatory on Health Systems and Policies, 2023). The estimated societal cost of depressive disorders in the Spanish adult population was calculated to be as high as €6145 million, with indirect costs related to long-term sick leave and permanent disabilities accounting for 60.5% (Vieta et al., 2021). In contrast, mental health services are underutilized in Spain, possibly indicating problems with access to such services (Lazarus et al., 2022). Prompted by the impact of the COVID-19 pandemic on mental health, the National Strategy for Mental Health 2022–2026 aims to improve services and support for families promoting a comprehensive community care model. The Strategy emphasizes the need for specialized human resources – psychologists, psychotherapists, mental health nurses and occupational workers – at community level, explicitly recognizing the weaknesses of the current hospital-centric SNS mental health system (Ministry of Health, 2022g).
Inappropriate use of resources
The presence of systematic differences in standardized population utilization rates of treatments may reflect underuse of treatments that have been proven effective, overuse of treatments in non-eligible patients, overuse of treatments when a more cost-effective alternative exists, the overuse of treatments that have been shown to be ineffective for most of the population treated, or the provision of low quality and unsafe services. Large variations in the rates of these treatments would represent failures in technical efficiency that, given the institutional design of the SNS, could also turn into a deficit of allocative efficiency. The Atlas VPM project provides a systematic assessment of the SNS, nationwide and region-wide, on multiple conditions and treatments and has found gaps in the effectiveness and efficiency of the health system that would require corrective policies (Angulo-Pueyo et al., 2022). Recently, the project has provided evidence on unwarranted and systematic variations in orthopaedic surgery (Ridao-López et al., 2020), low value care (Angulo-Pueyo et al., 2020), hospital quality (Comendeiro-Maaløe et al., 2022), quality of diabetes care, including suboptimal and unsafe prescriptions in diabetes (Angulo-Pueyo et al., 2023), and the uneven dispensation of antibiotics or opioids (Angulo-Pueyo et al., 2024).