-
02 July 2018 | Policy Analysis
Public-private partnerships in the Spanish National Health System: the reversion of the Alzira model
2.4. Regulation and planning
In general terms, the locus for planning and regulation resides essentially in the Ministry of Health when it comes to nationwide laws and plans, and lays on the Departments of Health of the 17 ACs when it comes to the local implementation of national laws or plans, or the development of regional regulation and policies, within their legally bound attributions. Since 2001, health system financing has been regulated under the general legal frame for the financing of the ACs, that is, under the responsibility of the Council for Fiscal Policy and Finance (Consejo de Política Fiscal y Financiera), a collegiate body composed of the Spanish and ACs’ ministers of finance, whose decisions turn into law under the responsibility of the Ministry of Finance.
See Box2.2 for the evaluation of priority-setting and planning.
Box2.2

In April 2018, the Regional Government of Valencia reversed the administrative concession to ‘RiberaSalud’, the emblematic public-private partnership (PPP) incepted in 1999 under the “Alzira’s model” trademark. This resulted in the regional health authority taking back responsibility for the governance and provision of hospital and primary care services delivered to 259,537 inhabitants in the area of La Ribera (Generalitat Valenciana, 2016). The decision of reversion reflects the electoral commitment of the current parties co-running the regional government, who assumed the profound controversy in the Valencian society related to the (so called) ‘privatization’ of public health services.
Context
The role of public provision in the statutory Spanish National Health System has been crucial since its inception and private providers used to play only a subsidiary role. Nonetheless, new regulation in the mid-1990s allowed health authorities to consider alternative governance and provision models (Bernal-Delgado et al., 2018). On this regard, the Autonomous Community (AC) of Valencia set up several PPPs as administrative concessions (del Llano et al., 2017). The first PPP established in 1999 was “Alzira”, where a private company, whose capital was owned by the Bank of Sabadell (50%) and Centene Corporation (50%), was in charge of providing hospital care, and, since 2003, primary care to all people living in the administrative healthcare area of La Ribera (García Armesto et al., 2010).
Impetus for the reform
Beyond the increasing societal discontent with the, so claimed, privatisation of public services, numerous flaws in the administrative concession process and its governance undermined the continuation of the contract. Among those failures: a) only one for-profit company (namely, RiberaSalud) presented an offer to the bidding process and hence, there was no real competition (Acerete et al., 2011); there was strong political influence on the decisions of regional savings banks (Acerete et al., 2011); c) the system showed high-potential of regulatory capture (NHS European Office, 2011); d) the intrinsic difficulties of a proper contract design resulted in high transaction and supervision costs; and, e) inappropriate incentives enabled cross-subsidization from public providers (Peiró-Moreno, 2017).
Content of the reform
Instrumentally, the reversion of the PPP entailed the termination (and non-renewal) of the contract between ‘RiberaSalud’ and the Health Authority of Valencia, and implied some changes in the purchasing and provision mechanisms; in the former case, the purchasing mechanism has evolved from an annual capitation procuring hospital and primary care services towards a yearly lump-sum budgeting mechanism; and, in the latter case, affecting the workforce, the personnel has been kept assuming its original labour conditions under private legislation, while the regular mechanism established to gain the condition of public servant is put in place.
Notably, in terms of coverage, the reversion has not implied any substantial modification in the scope, depth and breadth of the basket of benefits; nevertheless, the AC has highlighted its interest in enhancing primary care, developing home care services and increasing capital investments in high-technology.
As a final note, this reform is observed as a first step in the reversion of the remaining administrative concessions in the AC of Valencia, nowadays providing care to up to 655,000 inhabitants.
References
Acerete B, Stafford A, Stapleton P (2011). Spanish healthcare Public Private Partnerships: the Alzira model. Critical Perspectives on Accounting, 22: 533-549.
Bernal-Delgado E, García-Armesto S, Oliva J, Sánchez Martínez FI, Repullo JR, Peña-Longobardo LM, Ridao M, Hernández-Quevedo C (2018). Spain: Health system review. Health Systems in Transition, 20(2):1-192.
García-Armesto S, Abadía-Taira MB, Durán A, Hernández-Quevedo C, Bernal-Delgado E (2010). Spain: Health system review. Health Systems in Transition, 12(4):1-295.
Generalitat Valenciana (2016). Memoria de Gestión 2015 [Management Summary 2015]. Valencia, Conselleria de Sanitat Universal i Salut Publica (http://www.san.gva.es/es/web/comunicacion/memoria-2015, accessed 29 June 2018).
del Llano J (2017). Colaboraciones Público Privadas en Sanidad: ¿qué sabemos de ellas? En: López-Casasnovas G, del Llano-Señarís J (Eds.). Colaboración Público-Privada en Sanidad: el modelo Alzira. Fundación Gaspar Casal.
NHS European Office (2011). The search for low-cost integrated healthcare. The Alzira model – from the region of Valencia (http://www.nhsconfed.org).
Peiró-Moreno S (2017). Aspectos de Política Sanitaria. En: López-Casasnovas G, del Llano-Señarís J. (Eds.). Colaboración Público-Privada en Sanidad: el modelo Alzira. Fundación Gaspar Casal.
2.4.1. Regulation and governance of third-party payers
The role of third-party payers in the SNS is mainly assumed by the Health Departments in the 17 ACs (Fig2.1), although MFs for civil servants and mutualities for occupational diseases and accidents would also play a similar role (see section 2.1 Organization). Focusing on the Health Departments, they act, both, as public insurers (that is, warranting the access to the package of benefits covered by the public system) and services’ funders (that is, allocating the share of the regional public budget devoted to health, contracting services to public and private providers).
Fig2.1

In the last decade, the ACs’ Health Departments have preserved both responsibilities. However, their insurance role has been nuanced by the legal provisions in RDL 16/2012 with regard to decisions on the complementary and supplementary packages of benefits (see section 3.3.1 Coverage), and their funding role has been limited by the general economic and financial restrictions imposed by the Stability Programme. Since 2010, the budgetary discipline towards cost-containment on personnel, current expenditures and investment has framed the action of Health Departments – between 2009 and 2015, government expenditure on health reduced 0.9 points of the GDP, equivalent to a 5.3% reduction – €68 870 million in 2009 to €65 199 million in 2015 (MSSSI, 2015b) (see section 3.1 Health expenditure). As a consequence, the usual negotiation of contracts has turned into a simplistic cost-containment strategy, affecting both public and private contracts.
2.4.2. Regulation and governance of provision
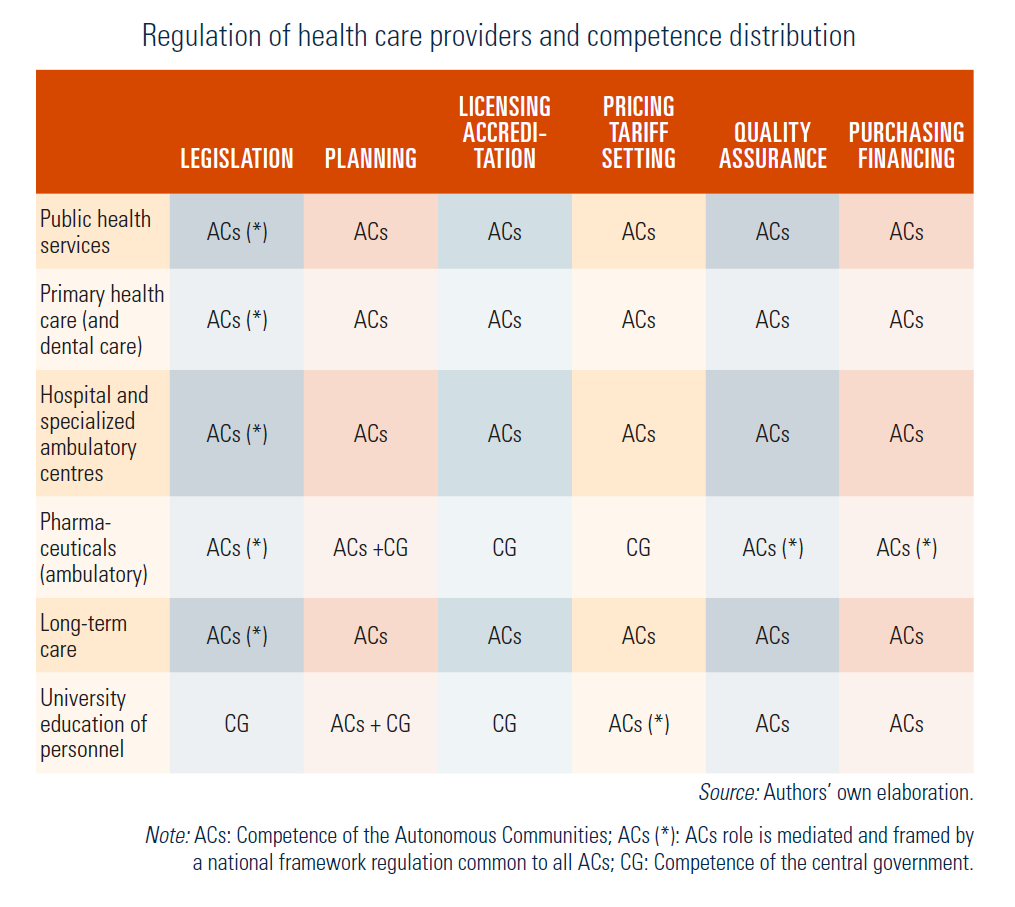
No major changes have been observed when it comes to regulation and governance of provision in the last decade. Table2.1 exhibits, at a glance, what are the main providers in place, the aspects that require regulation and what institution exerts governance or stewardship – central government or ACs. In general terms, care services – except pharmaceutical care – are fully governed by the ACs – planning, accreditation, quality assurance, financing and pricing. Legislation is shared by the central and ACs’ governments. In this case, the national regulation (basic legislation common to all the ACs) frames the ACs’ legislation. In the case of pharmaceutical care, except in the case of licensing and pricing, both of which are the full responsibility of the central government, the remaining roles are regulated by ACs taking into consideration the national regulatory frameworks. Lastly, the legislation and accreditation of health workforce higher education is the full responsibility of the central government (namely, the Ministry of Education).
Table2.1
When it comes to the formal relationship with care providers, ACs’ Health Authorities contract with both public and private providers, in terms of the number of services, quality and cost. In the case of public providers, although not legally bound, the contract is monitored and the performance results are taken into account in future negotiations. In the case of private providers, usually hospitals whose activity is subsidiary to public system needs (for example, waiting list programmes, beds for palliative care), a number of services are purchased and providers are paid according to public predefined tariffs and contract accomplishment. When it comes to pharmaceutical care, ACs reimburse pharmacies for drugs dispensation according to the pricing and co-payment mechanisms regulated by the corresponding central government bodies (see section 5.6 Pharmaceutical care).
Unlike this general scheme, the PFIs and the private–public partnerships (P–PPs) provision schemes, whose most internationally known example is the P–PP called Alzira Model (focus initially on the provision of hospital care expanding later on to primary care), were observed to deepen until 2011, particularly after the 2007 regional elections. Arguably, PFIs and P–PPs were seen as an eventual solution to the lack of efficiency of public providers and, later, to the increasing budget cutbacks, particularly on investments. Two ACs, Valencia and Madrid, championed the use of P–PPs in five and three hospitals, respectively. When it comes to PFIs, 13 hospitals were built and equipped in five ACs, seven of them in the AC of Madrid. The negative evolution of the crisis, and the strong public debate on PFIs and P–PPs as subterfuge for “public services privatization” exhausted their momentum. The current ACs’ governments of Madrid and Valencia have decided to directly run the PFI hospitals (Madrid) and to reverse the Alzira Model in April 2018, when the P–PP contract comes to an end (Valencia).
In the context of a growing external intervention of the financial authorities, public health care provision remains widely anchored in the inflexibility of bureaucratic models both at national and regional levels. Along with these constraints, the increasing partisan interference in the management decisions, and a widespread claim for transparency and accountability have led to a public debate on the good governance of health services. In some ACs, the debate has translated into specific actions; as outstanding examples, the recommendations by the Basque Country Advisory Council for Public Health Services Good Governance (Osakidetza, 2011), or the most recent legal initiative approved in the Regional Parliament of Madrid (BOAM, 2017) aimed at creating collegiate governing bodies, encouraging professionalism in management, and fostering accountability, transparency and participation.
2.4.3. Regulation of services and goods
Main innovations in services and goods’ regulation are enacted in the aforementioned RDL 16/2012. Until 2012, the Spanish SNS had a comprehensive common package of benefits, free of co-payment, except the flat 40% for retail price in prescribed drugs (exemption made for pensioners and certain chronic conditions), and some specific products and prostheses. ACs were able to complement the SNS common package within their territory with additional services. The new 2012 regulation categorized the SNS common package in three different benefit packages: (a) the basic package for all those insured and their dependants, which includes “essential” activities, including medical visits and hospitalizations; (b) a “supplementary” package, cost-shared by the patients, including pharmaceutical benefits (in practice, co-payment affects mainly outpatient pharmaceutical prescriptions and specific orthesis and orthopaedic prosthesis) (see section 3.3.1 Coverage and section 6.1 Analysis of recent reforms); and, (c) an “accessory” package, which includes “non-essential” activities, still vaguely defined (see section 3.3.1 Coverage and section 6.1 Analysis of recent reforms).
In this context, RDL 16/2012 stressed the need for evaluation, paving the way for the reinforcement and empowerment of the network of health technology assessment agencies (that is, agencies in Catalonia, Basque Country, Galicia, Aragon, Andalusia, Canary Islands and Madrid). Within their current mandate, health technology assessment agencies review subsets of existing benefits, coordinate and design ad hoc evaluative studies for the adoption of new technologies and standardize methodologies for evaluation (REDETS, 2017) (see section 6.1 Analysis of recent reforms).
2.4.4. Registration and planning of human resources
The statutory Spanish SNS is a strongly regulated system, affecting both goods and prices. When it comes to human resources, the SNS is populated by civil servants and, except partially in the case of emergency care and temporary positions, which were rather infrequent in the aftermath of the crisis, the traditional supply and demand levers do not generally operate. The main workforce planning drivers for the SNS are the “numerus clausus” that limit the entrance to undergraduate education, and the access barriers to the residency (doctors) and specialization (nurses) programmes. Noticeably, these two planning measures are rarely aligned, as the former is run by the education system and the latter by the health system, each with different contextual and institutional incentives.
The SNS workforce-planning concerns, such as the forecasted shortage of professionals due to numerous retirements in 15 years attributable to the demographic changes, have usually been present in the discussions of the Interterritorial Council, particularly after the start of the crisis. In the plenary meeting of the Interterritorial Council of 18 March 2010, an agreement was reached with regard to the need to “establish a common planning mechanism for all health professions, and for the whole SNS, according to need” (MSSSI, 2010). Upon this agreement, and the conclusions of some technical reports, notably the White Report for the SNS Human Resources (MSSSI, 2013), the main action implemented so far has been the development of a National Registry of Health Care Professions (RD 640/2014).
The Registry, managed by the Ministry of Health, aims to collect relevant information from health professionals (in the public and private sectors) coordinating in a single registry the different workforce registries developed by the ACs. Besides its potential use in human resources planning and policy-making, the Registry has been designed to also respond to the provision on patients’ information rights prescribed in the Law 3/2014 and to the requirements of the Cross-Border Directive (RD 81/2014). The Registry will contain information on professionals’ qualification, specialization, additional training, current position, and administrative or legal circumstances worth knowing (for example, disciplinary measures). In the Interterritorial Council plenary session of 21 June 2017, the Ministry of Health presented for consultation the executive order that regulates the implementation of the Registry.
2.4.5. Regulation and governance of pharmaceuticals
The Spanish pharmaceutical sector is one of the most regulated sectors of the Spanish economy. In addition to the centralized approval mechanism provided by the European Medicines Agency, the Spanish Agency for Medicines has to approve the effective commercialization of any drug, as well as the regulation for drugs pricing and public reimbursement. Once commercialization is approved, companies might seek public reimbursement. This decision will be made by the Inter-ministerial Commission on Prices of Medicines, an administrative advisory body of the Ministry of Health, according to a number of criteria:
- severity, duration and consequences of the disease for which the drug is indicated;
- specific needs of certain groups;
- therapeutic and social value and incremental clinical benefit in terms of cost-effectiveness;
- budgetary impact;
- existence of drugs or other therapeutic alternatives at a lower price or lower cost of treatment; and,
- the degree of innovation of the drug under evaluation.
The regulation scheme issued in the Act for Guarantees and Rational Use of Pharmaceuticals and Health Products (Law 29/2006) has not significantly changed in terms of actors and responsibilities (see table 6.9 in García-Armesto et al., 2010). The new regulation issued since 2010 by the central government has aimed at deepening the regulation issued in the aforementioned law, in a new context of fiscal revenues reduction and growing public debt. Thus,
- RDL 4/2010 ruled, among other elements, the reduction of drug prices in both drugs already under the reference pricing scheme and those not included yet;
- RDL 9/2011, among other measures, deepened the reference pricing policy guaranteeing homogeneity across the country, prompted generic prescription through the prohibition of brand-name prescription, and created the Committee on the Cost-Effectiveness of Pharmaceuticals and Health Products, who will report on the price policies developed by the Inter-ministerial Commission on Drugs Pricing;
- RD 177/2014, developed in the context of RDL 16/2012, that deepened in the regulation of reference prices and groups of homogeneous drugs, also aimed at regulating the information system required for drugs pricing and ACs financing; and
- Law 10/2013, modifying technical aspects of Law 29/2006; among the measures the text emphasized the need for the ACs to avoid policies that could lead to differences in pharmaceutical benefits and prices, distorting the in-country ‘single market’ principle and increasing inequalities.
Notably, the secular tension between the Ministry of Health and the ACs’ Health Authorities with regard to drugs approval and pricing (decisions on drugs approval and pricing lay on the Ministry of Health while pharmaceutical care expenditure is entirely assumed by the ACs) has been seen during this period. The epitome of this tension was the negotiation of the funding method for direct acting antiviral drugs for hepatitis C, where an unprecedented earmarked fund was set up according to a price–volume scheme, to be charged to ACs and paid back in 10 years – without interests and with a 2-year grace period (Campillo-Artero, García-Armesto & Bernal-Delgado, 2016; MSSSI, 2016e).
2.4.6. Regulation of medical equipment, devices and aids
Since RD 1030/2006, legislation that defined the common package of benefits and the updating procedure (see García-Armesto et al., 2010 for more information), the first substantial reform was issued in RD 16/2012 (and subsequent legislation), which aimed at implementing urgent measures to guarantee the SNS sustainability. It is worth highlighting the Ministerial Executive Order SSI/1356/2015 that regulated the authorization and inclusion of “medical devices and aids” as part of the common package of benefits, as well as the methodology for its evaluation.[9] Order SSI/1356/2015 specifically updated the list of orthoprosthesis and medical aids to be included in the common package, with a view to be the basis for a coherent and homogeneous set up of co-financing caps.
In turn, the procedure of inclusion of new medical devices and aids follows the same path as any other benefit; hence, the decision is made by the Interterritorial Council upon the proposals submitted by the Commission on Benefits, Insurance and Financing and the (mandatory) technical advice of the Spanish Network of Agencies for the Evaluation of Health Technologies and Benefits Assessment (HTBA) (see section 6.1.8 A new status for Health Technologies and Benefits Assessment).
- 9. Previous to this one, a specific Ministerial Executive Order (Order SSI/1640/2012), had updated breast prostheses and devices to prevent pressure ulcers. ↰