-
01 July 2024 | Country Update
New benefits in the SNS portfolio -
03 December 2018 | Country Update
The depth of coverage of the Spanish NHS has been updated -
04 October 2018 | Policy Analysis
New reform on the breadth of the Spanish Health System -
05 July 2018 | Country Update
New Ministry of Health in Spain revoking requirements for coverage entitlement
3.3. Overview of the statutory financing system
RDL 16/2012, a legal text that aimed at guaranteeing the sustainability of the SNS (and subsequent legislative developments in RD 1192/2012, specifying the condition of the SNS beneficiary, and RD 576/2013, establishing the procedure and tariffs for non-entitled individuals who wanted to purchase SNS public coverage) and was issued in the context of the 2010 Stability Programme for the Kingdom of Spain (Ministry of Finance, 2010b), has implied a change in the scope, depth and breadth of the SNS benefits.
In the last Interterritorial Council held in November 15th, the Ministry of Health and the regional health representatives approved a revision of the common health benefits package, which entailed the modification of Royal Decree 1030/2006 establishing the common benefits package for the Spanish National Health Service and updating procedures.
Among the new benefits, it is worth highlighting the inclusion of both areola and nipple micropigmentation techniques as part of breast reconstruction, and the screening programme for cervical cancer that now will become population-based.
Regarding prostheses, the catalogue of benefits will now include new models of external prosthesis for breast implant, facial restoration and eye readers for motor neurone diseases. Hearing aids for older people will now be included in the common health benefits package.
Finally, five patient groups with diabetes type I requiring more than 6 glycaemic controls per day will benefit from the use of flash glucose monitors. These groups are those diabetic patients visually or severe functionally impaired, patients with recurrent hypoglycaemia, pregnant women and patients with uncontrolled HbA1 (values above 7.5%).
More information (in Spanish): https://www.mscbs.gob.es/gabinete/notasPrensa.do?id=4430
Context
Until 2012, health care coverage in the Spanish National Health System (SNS) was almost universal (99.5%) and guaranteed quite a comprehensive package of benefits to all citizens (García-Armesto et al., 2010). Entitlement used to be independent of the labour status and personal wealth of the individual. With regard to foreign residents, the Organic Law 4/2000 (BOE, 2000) on the rights and freedoms of foreigners in Spain and their social integration established the coverage conditions allowing the same entitlements for those residing and working permanently, providing access according to their country insurance scheme for those nationals from countries with bilateral agreements, or providing full access to registered undocumented migrants with annual incomes equal to or lower than the minimum inter-professional wage.
Impetus for the reform
In the context of the 2010 Stability Programme for Spain and, in the aftermath of the economic and financial crisis that started in Spain in 2008, the Royal Decree-Law (RDL) 16/2012 was introduced to guarantee the sustainability of the SNS (BOE, 2012a). The RDL 16/2012 and subsequent legislation (BOE, 2012b) changed the basis for entitlement to health care by linking the right to the legal and working status of the individuals. In practical terms, only undocumented immigrants ended up excluded from health care coverage, with the exception of emergency, and obstetric and child care. The exclusion of this population subgroup from full coverage was seen to potentially increase health inequalities and to result in negative consequences in public health (Bernal-Delgado et al., 2018). Despite this national regulation, some regional Health Authorities did not exclude undocumented migrants from health care coverage.
Content of the reform
Following a non-confidence vote taking place 1st June 2018, the conservative Prime Minister until then (Mariano Rajoy) was ousted by the social-democrat candidate (Pedro Sánchez), who was sworn as Prime Minister one week later and named a new Cabinet (see Reform Log 5/07/2018).
During the first weeks of mandate, the new Health Minister started working to restore the status quo before the RDL 16/2012. The Minister met first representatives of the civil society known for their defence of universal health care, such as Amnesty International or Doctors of the World, as well as some Professional Associations on Family and Community Medicine and Public Health and some of the trade unions in the sector (Ministry of Health, 2018a). These meetings were followed by a specific Interterritorial Council, held on June 28th, where the Ministry and the regional Health Authorities set up the path to increase the coverage entitlement basis as it used to be before 2012 (Ministry of Health, 2018b).
This process has come to an end, with the Spanish Parliament approving the RDL 7/2018 in September 6th, where the basis for entitlement returns to be linked to the condition of resident. In the new law undocumented migrants have recovered eligibility to full coverage as any other Spanish national. The RDL foresees exceptions related to having health coverage linked to bilateral agreements between countries or having a third party obliged to pay for the health services provided. Last but not least, under any circumstance, migrants are allowed to claim for the health coverage entitlement conditions of the country of origin.(BOE, 2018).
According to the new legislation, regional Health Authorities have to issue specific health insurance cards for those undocumented migrants accrediting more than 90 days in the country (otherwise, according to the Organic Law 4/2000, they are considered in temporal stay, that is, non-residents). In the eventual case that an individual requires health assistance within those 90 days, social services should first submit a favourable report.
Except for the case of pharmaceutical care, where the RDL also defines the pharmaceutical co-payment threshold for this population in a fixed 40% of the retailing price, irrespective of their income level (unlike the rest of the population), the remaining benefits are funded following the SNS general scheme – a tax-funded system which is free of charge at the point of care (Bernal-Delgado, et al., 2018). Finally, as a specific provision, the RDL establishes that the Interterritorial Council (the governing body for the SNS) will define access requirements for those migrants needing an organ transplant.
Final remarks
Although no formal procedure has been established to assess the impact of this new policy, the Interterritorial Council held in 28th June agreed with the creation of a joint committee, made up of representatives from the organizations defending universal insurance, whose aim will be to monitor the compliance of the new RDL (Ministry of Health, 2018b).
References
Bernal-Delgado E, García-Armesto S, Oliva J, et al. Spain: Health system review. Health Systems in Transition, 2018;20(2):1–17 (http://www.euro.who.int).
BOE (2000). Organic Law 4/2000, 11 January, on rights and freedoms of foreigners in Spain and their social integration (https://www.boe.es/buscar/pdf/2000/BOE-A-2000-544-consolidado.pdf, accessed 13 September 2018).
BOE (2012a). Royal Decree-Law 16/2012, 20 April, on urgent measures to guarantee the sustainability for the National Health System and to improve the quality and safety of their benefits (https://www.boe.es/boe/dias/2012/04/24/pdfs/BOE-A-2012-5403.pdf, accessed 13 September 2018).
BOE (2012b). Royal Decree-Law 1192/2012, 3 August, regulating the condition of insured and of beneficiary for the purpose of the health care services in Spain, out of public funds, through the National Health System (https://www.boe.es/boe/dias/2012/08/04/pdfs/BOE-A-2012-10477.pdf, accessed 13 September 2018).
BOE (2018). Royal Decree-Law 7/2018, 27 July, on National Health System universal access (https://boe.es/boe/dias/2018/07/30/pdfs/BOE-A-2018-10752.pdf, accessed 13 September 2018).
García-Armesto S, Abadía-Taira MB, Durán A, et al. Spain: Health system review. Health Systems in Transition, 2010, 12(4):1–295.
Ministry of Health (2018a). Press release, 20 June 2018 (http://www.mscbs.gob.es/gabinete/notasPrensa.do?id=4336, accessed 17 September 2018).
Ministry of Health (2018b). Press release, 28 June 2018 (http://www.mscbs.gob.es/gabinete/notasPrensa.do?id=4341, accessed 17 September 2018).
Following a non-confidence vote taking place 1st June 2018, the conservative Prime Minister until then (Mariano Rajoy) was ousted by the social-democrat candidate (Pedro Sánchez), who was sworn as Prime Minister one week later and named a new Cabinet. In this new government, the former Ministry of Health, Social Services and Equality has become the Ministry of Health, Consumers and Social Welfare.
One of the first measures of the new government, stemmed from a partisan commitment, has been to summon the regional health authorities and the civil society for an open debate aimed to re-establish the universality of the Spanish National Health System (until now, legislation had excluded undocumented migrants from coverage, with some exceptions – see RL 05/03/13).
The Interterritorial Council held in June 28th set up the path to extend full coverage to undocumented migrants and a new Royal Decree Law (RDL) repealing RDL 16/2012 is expected in the short-term.
3.3.1. Coverage.
Who is covered?
Until 2012, the SNS coverage was almost universal (99.5%) and guaranteed quite a comprehensive package of benefits to all citizens. Entitlement used to be independent of the labour status and personal wealth and only a negligible 0.5% of the population remained out of coverage.
On the other hand, coverage of foreign residents was regulated by Law 4/2000 (and subsidiary legislation), on rights and freedoms for foreigners in Spain and their social integration. Hence, non-Spanish citizens residing in Spain could follow different entitlement paths, depending on their citizenship and administrative legal status. According to this Law: (a) people residing and working permanently in Spain received the same entitlement enjoyed by Spaniards; (b) EU citizens and people from countries with bilateral agreements were entitled to receive the benefits although remained insured according to their national insurance schemes; and (c) only registered undocumented immigrants with annual incomes equal to or lower than the minimum interprofessional wage enjoyed full entitlement.
RDL 16/2012 changed the basis for entitlement, linking the right to the legal and working status of the individuals. Hence, publicly funded health care was assured for (a) employees contributing to the social security system and their dependants (that is, spouse, dependent former spouse, descendants under 26 or with a significant disability), (b) retirees, (c) those receiving unemployment subsidies, and (d) unemployed who had exhausted the unemployment dole. Nonetheless, Spanish people not included in the aforementioned criteria and foreigners with legal residence in Spain remained entitled to public insurance. In practical terms, only undocumented immigrants ended up excluded from the coverage.
This new regulation implied the modification of entitlement of non-Spanish citizens. So, people from countries other than EU Member States or nationals from countries with bilateral agreements were only entitled to emergency care for serious illness or accidents until discharge (regardless of the cause), and to obstetric and child care (for people younger than 18 years).
At the time of writing (June 2018), the recently elected Spanish Government has started a dialogue process with the regions and the civil society to re-establish the universality of the SNS (MSSSI, 2018b). A new Royal Decree-Law repealing RDL 16/2012 is expected in approximately 6 weeks (La Moncloa, 2018). The new Ministry of Health, Carmen Montón, has summoned the ACs on 28th June for an Interterritorial Council, focused on universal coverage (Redacción Médica, 2018).
What is covered and how much of the cost is covered?
RDL 16/2012 also aimed at regulating the package of benefits provided by the statutory health system with a view to define what benefits should be co-financed by patients. The regulation did not explicitly exclude any benefit (those already out of coverage remain excluded: psychoanalysis and hypnosis, spa treatments, plastic surgery not related to accidents, or some pharmaceutical products) but established what benefits are subject to patients’ cost-sharing.
Hence, the new regulation has defined two categories of services: the common package with three subcategories – core package, supplementary package and accessory services – common to the 17 regional services composing the SNS; and, the complementary package, decided under the rule of the ACs (see section 2.4.2 Regulation and governance of provision).
The common core package of health care services of the SNS includes all health care prevention, diagnosis, treatment and rehabilitation services, as well as emergency medical transportation. Hence, the core package includes a comprehensive package of primary health care benefits (for example, acute and chronic care, health promotion and prevention activities, physiotherapy, mother and child care, mental health care, palliative care, medical counselling, basic dental health services), and specialized health care benefits (for example, any diagnostic and therapeutic procedure to be provided as outpatient specialized care, inpatient acute or long-term care, day-care surgical or medical care, palliative care, acute or long-term mental health care, home care, organ transplants, emergency care). These core benefits are not subject to any patients’ cost-sharing.
In turn, pharmaceutical prescriptions and orthoprosthetic devices under the supplementary common package are subject to users’ cost-sharing. RDL 16/2012 indicates that co-payments must be set on the final product price, and be fixed according to the annual household income and a maximum ceiling of monthly payment.
Finally, the accessory services, also subject to the same cost-sharing scheme, have been vaguely described as all activities, services or techniques, without character of benefit, that are not considered essential and/or are used as aid-devices for chronic care improvement. This third package has not yet been regulated.
In the case of the complementary package of services, ACs may incorporate into their own package of benefits any technique, technology or procedure not covered by the common core package of the SNS, if they provide the resources needed for their financing.
The content of the common benefits package is defined by the highest governing body of the SNS (namely, the Interterritorial Council), upon the proposals submitted by the Commission on Benefits, Insurance and Financing and the technical advice of the Spanish Network of Agencies for HTBA. The decision of any inclusion should be reported in advance to the Governing Body of the SNS, and is conditioned on the AC’s financial sufficiency.[10]
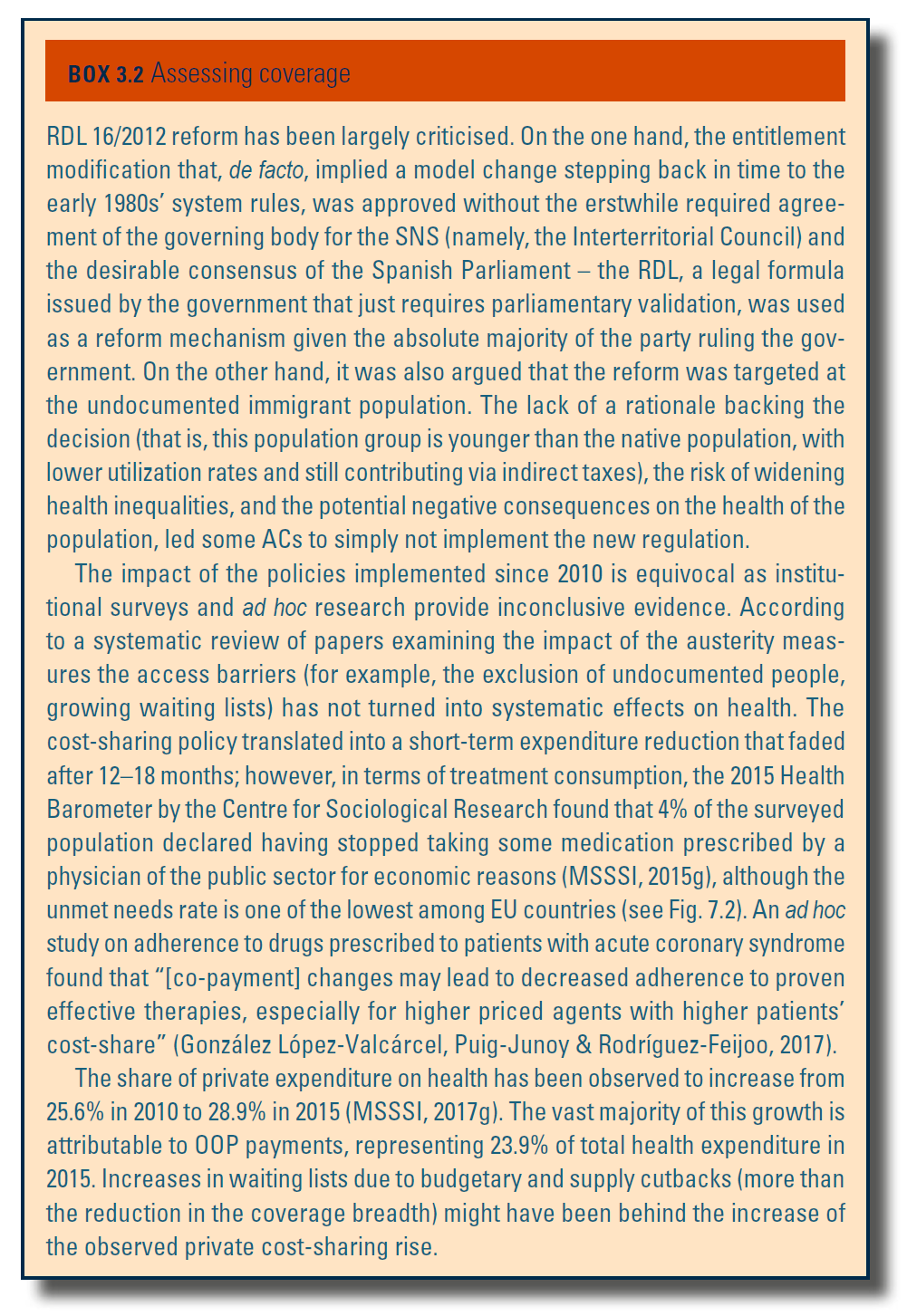
See Box3.2 for the assessment of coverage.
Box3.2
- 10. Financial sufficiency is defined according to the objectives of stability included in the Stability Programme for the Kingdom of Spain (Ministry of Finance, 2010a). ↰
3.3.2. Collection
General government budget
The vast majority of public health expenditure in Spain is funded through general taxation (see section 3.2 Sources of revenue and financial flows).
The Spanish tax system is highly decentralized. The current regional financial scheme was agreed in July 2009 by the Economic and Fiscal Policy Council (in Spanish, Consejo de Política Fiscal y Financiera), a public body composed of representatives of the central and regional governments that are responsible for the fiscal and financial coordination between ACs and the central government. The corresponding legislation (Organic Law 3/2009 and Law 22/2009) was passed in December 2009, although the system was not enforced until the 2011 Spain’s General Budget Law was approved. Leaving aside social security contributions (which are earmarked for pensions and other monetary benefits), tax revenues can be grouped into two main categories: taxes linked to production and imports (“indirect taxes”, such as value added tax, VAT); and “direct taxes” (that is, taxes on income and wealth). More than half of tax revenues (52.2% in 2015) come from indirect taxes, VAT being the main source of funds within this category (28.7% of total resources). Taxes on income and wealth provide 45.2%, with capital taxes adding the remaining 2.6% (direct taxes amount to 47.8%) (Ministry of Finance, 2017b). The aforementioned figures only applied to the so-called “common regimen of ACs” (that is, all the regions but Navarre and the Basque Country[11]), where the responsibility on tax collection is shared by the regional authorities and the Spanish Fiscal Revenue Agency (Agencia Estatal de Administración Tributaria). ACs are also responsible for the collection of those taxes assigned to the regional level (inheritance taxes, wealth transfer taxes) and share tax collection for VAT, personal income tax and excise taxes.
As a consequence of this joint responsibility for revenue collection, regional governments (ACs) have 50% of the personal income tax available (with limited tax-raising ability), as well as 50% of the revenues generated within their territories by VAT and 58% of those yielded by selected excise taxes (on alcohol, tobacco and hydrocarbons). These sources, together with the revenues obtained by means of other fiscal instruments with less revenue-raising capacity (for example, wealth and inheritance taxes, car registration taxes) give ACs a significant fiscal autonomy. However, none of those taxes is earmarked for health expenditure but for the financing of all the welfare services in the ACs.[12]
Taxes, contributions or premiums pooled by a separate agency
The second statutory system (the mutual funds MUFACE, MUGEJU and ISFAS) aims to provide services for a group of civil servants and public servants that include health care services as part of the benefits granted in exchange for the contributions paid by their members (see section 2.1 Organization). The contribution rates are set by the central government in the general budget law each year. Currently, public employees belonging to the aforementioned mutual funds pay a monthly premium between €20 and €50, according to their professional category (a total of six groups or levels exist among the civil servants) that covers up to 15% of the overall insurees’ expenditure in health care services; the remaining 85% is covered from the budget of the Ministry of Finance (through income tax revenues, essentially).
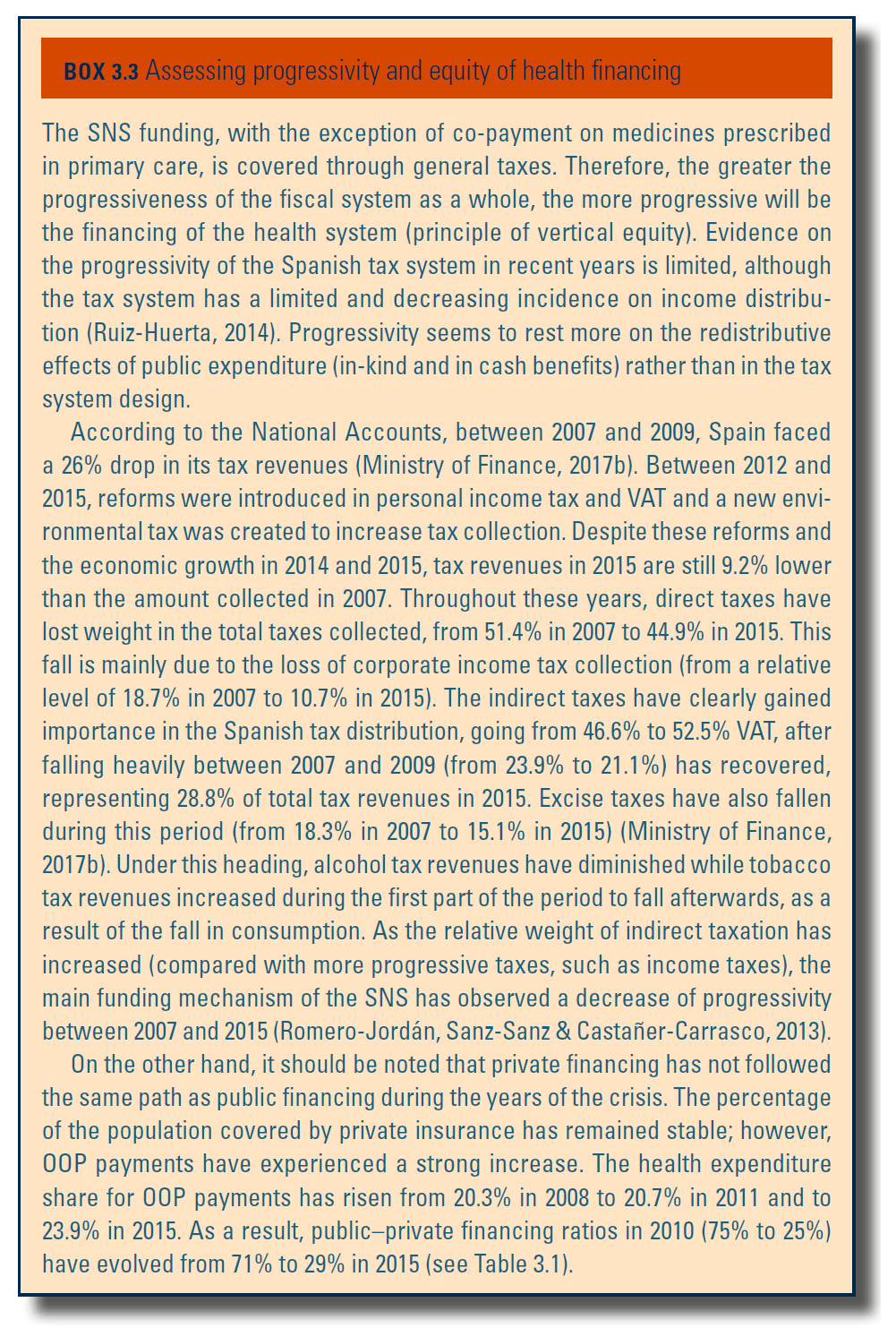
Box3.3 provides the assessment of progressivity and equity of health financing.
Box3.3
- 11. In turn, Navarre and the Basque Country enjoy a special financial regimen based on a particular legislation (namely, derechos forales), acknowledged in the Spanish Constitution. By virtue of this specific legislation, regional authorities collect all the taxes levied in their corresponding territories, and then transfer a certain amount of revenues to the central government for the services that the latter provides to the citizens of those regions (i.e., non-devolved services, for example, national defence). ↰
- 12. The only exception in this regard is a specific tax on hydrocarbon sales levied by ACs from 2002 to 2012, when the Court of Justice of the EU passed judgement that the tax was against EU legislation (92/12/CEE Directive). The tax was deemed null and void. ↰
3.3.3. Pooling and allocation of funds
Allocation from collection agencies to pooling agencies[13]
Although the Spanish tax system is highly decentralized (see section 2.2 Decentralization and centralization), there is a complex system of “compensation funds” that aims at reducing funding imbalance across ACs. Hence, upon the ACs’ own fiscal revenues and the so-called Fund for Basic Public Services, health services are also funded by the Fund for Global Sufficiency, the Healthcare Guarantee Fund and various “convergence” funds (namely, Competitiveness, Cooperation and Interterritorial Compensation funds).
The Fund for Basic Public Services represents 75% of the aggregate fiscal capacity. This pooled fund is distributed to the ACs in accordance with a needs-based weighted formula. This formula includes the magnitude of the population to be served (weighting 30% in the formula), the population actually covered by the SNS (38%), the population aged 16 and younger (20.5%), the population aged 65 and over (8.5%), the geographical extension (1.8%), the population density (1.6%) and the insularity (0.6%). The purpose of this Fund is to allow regions with similar needs to provide similar levels of welfare services (that is, health, education and social services).
It might be the case that health care expenditure needs are not fully covered with the ACs’ own fiscal revenues[14] and the Fund for Basic Public Services. This potential contingency is addressed with the Fund for Global Sufficiency. The Fund for Global Sufficiency is calculated according to the actual health expenditure and may be negative for certain ACs (typically, high-income regions) if tax revenues and the amount of the Fund for Basic Public Services exceed the financial needs for the AC. Finally, the allocation of funds through the Fund for Global Sufficiency also depends on the financing that the ACs receive from another fund, the Healthcare Guarantee Fund, which aims to cover the assistance provided in a particular AC to an insuree with residence in a different AC. This Healthcare Guarantee Fund has been regulated in the aforementioned RDL 16/2012.[15]
In addition to these funding mechanisms, there are three “convergence” funds aimed at providing additional funding to the regions with a low level of per capita resources – the Competitiveness Fund, and those worse-off in terms of households incomes – the Cooperation Fund. Upon these two health-care-specific funds, ACs have access to the Interterritorial Compensating Fund, which aims to finance investment costs in those low-income ACs.
Funding priorities have focused on addressing the financial constraints (cash flow tensions) that regional governments suffered as a direct consequence of the economic crisis. Hence, the central government has devoted additional funding through: (a) the Liquidity Fund (in Spanish, FLA) created as a temporary and voluntary mechanism to support ACs’ debt maturities, through RDL 21/2012; and (b) the Fund for the Financing of Provider Payments (created through RDL 7/2012), which allows ACs to cancel outstanding liabilities to suppliers, many of them serving the ACs’ health care premises. The access to this funding scheme is conditioned on the accomplishment of fiscal and expenditure AC liabilities, and the approval of the Ministry of Finance and Public Administrations.
Since 2015, the access to additional credit allowances has been linked to the measures adopted by the ACs to control health care expenditure, in particular, pharmaceutical expenditure growth (Organic Law 6/2015). Although adherence to this measure is voluntary, ACs have powerful incentives to join the programme as those compliant are eligible for additional funding.
Allocating resources to purchasers
Previous paragraphs have already provided an overview on how funding is collected and allocated to the ACs (that is, regional departments of finance and treasury who are responsible for budget allocation across regional government departments), or to the Ministry of Public Administration, in the case of the statutory system for civil servants.
In the case of ACs, once the regional budget allocation is endorsed by the regional parliament, the third-party budget-setting and split-purchasing role are played by the health departments in the 17 ACs (and INGESA for the Autonomous Cities of Ceuta and Melilla) which “purchase” services from either public or private providers for all the insurees living in the AC. In the case of civil servants, the MFs, which receive the corresponding share of the budget (as well as the beneficiaries’ contributions), purchase services for their beneficiaries. MFs are expected to purchase both private and public providers depending on the decision of their beneficiaries, who in a yearly basis opt for either type of providers.
- 13. Note that this allocation to pooling agencies section refers to the “common regimen of the ACs”, which includes all ACs except the Basque Country and Navarre, as they enjoy a different financial regimen in which they collect all the taxes levied in their corresponding territory and make their allocation decisions in the corresponding regional parliament. This section also does not address the MFs for civil servants, for which funding is allocated as part of the central government budgeting decisions. ↰
- 14. According to the still current 2009 agreement for the funding of the ACs, the regional governments retain 25% of their fiscal capacity via 50% of income taxes, 58% of VAT and excise taxes collected in their territories, and 100% of taxes on inheritances, car registration, wealth transfers and stamps. ↰
- 15. The Healthcare Guarantee Fund plays a similar role to the one played by the Health Cohesion Fund, which was intended as a tool for the Ministry of Health to implement policies guaranteeing cohesion and equity in the SNS. The resources assigned to this fund in the central general budget have been progressively reduced over the years, to the point of disappearing in 2016. ↰
3.3.4. Purchasing and purchaser–provider relations
Public provision in the SNS plays a prominent role and, in general, the public bodies in charge of the purchasing (for example, the ACs’ health departments) purchase the services from another public body, closely linked to the former, so called regional health service. The latter is the administrative structure organically linked to the AC health department that runs all inpatient and outpatient health care centres. Generally, the health department contracts (and budgets) annually the services with the regional service which, in turn, negotiates global annual contracts with its providers. Additionally, either the ACs’ health departments or the regional health services contract services from private providers, usually hospitals.
There are some specificities worth mentioning. Unlike the general scheme in which private providers play a subsidiary role, in Catalonia, the regional health service contracts out with a collection of not-for-profit private providers integrated within the network of public providers, composing the so-called Hospital Network for Public Utilization (see section 5.4 Specialized ambulatory care/inpatient care). It is also worth highlighting a particular experience in Valencia, where the department of health moved in 1999 out of the general scheme by purchasing integrated health care services from private providers, based on an annual capitation payment. This singular P–PP started with the Hospital de La Ribera in Alzira, and the model has been extended to four more health care areas within the AC – 18.7% of the overall population.
Within the general scheme, regional health services contract hospital care, primary care, preventive activities and long-term services with public and private providers. Hospital services by public providers are financed prospectively according to volume and quality. The regional health service monitors contracts at intervals agreed between the signing parties (usually on an annual basis). Although some improvement has been made in terms of setting budgets in a prospective way, the method still has certain deficiencies, as the economic incentives for the accomplishment of the annual contract are too weak, the transfer of risk to professionals is not credible and the monitoring is rather loose. A flaw in the design of these contracts is the lack of incentives for coordination with primary care or linkage with existing public health activities.
In addition to public providers, a certain amount of activity is contracted out to private providers, typically aimed at reducing waiting lists for surgical procedures or high-technology diagnostic tests, but also to complement long-term care services and palliative care. These are generally prospective volume contracts with some ex post correction clauses. Depending on the nature of the specific activity, the contractor determines the basis for payment; hence, long-term care activity is usually measured in terms of stays, whereas surgical interventions and diagnostic tests follow a fee-for-service (FFS) scheme. Contracts with private providers have tended to increase since the mid-1990s, and in 2014 amounted to 12% of total public health expenditure (González López-Valcárcel, Puig-Junoy & Rodríguez-Feijoo, 2017).
Finally, primary health care services are contracted, with very few exceptions, with public providers. Hence, the dominant practice entails a contract of acute, chronic and preventive care services, funded according to block grants normally nuanced by population demographics. The contract reflects specific objectives prioritizing certain care or preventive programmes, and also some incentives linked to the achievement of certain prescription targets aimed at increasing the rational and appropriate use of drugs. Among the few exceptions are: the externalization of primary care by way of the so-called Entidades de Base Asociativa in Catalonia, which are ‘limited partnerships’ of primary care practitioners that provide care to a defined population according to a contract with the Health Department (resembling to a certain extent Clinical Commissioning Groups in the United Kingdom); and primary health care as part of the aforementioned P–PP in Valencia.
References
More information (in Spanish):
Order SND/606/2024 https://www.boe.es/diario_boe/txt.php?id=BOE-A-2024-12290