-
15 July 2025 | Policy Analysis
Steps to reform emergency medical services in Slovakia -
01 May 2023 | Policy Analysis
Ageing in Slovak healthcare workforce: Not a threat to oral medicine -
30 December 2022 | Policy Analysis
Changes to workforce remuneration following the mass resignation threat of hospital-employed doctors -
10 October 2022 | Country Update
Increases to minimum wages for hospital sector employees -
01 October 2022 | Policy Analysis
Reform of education of doctors -
11 August 2019 | Policy Analysis
New projections on the shortage of doctors and nurses and measures taken by the MoH
4.2. Human resources
General overview
In March 2025, the Slovak Government approved the most significant reforms to the emergency medical services (EMS) system in over two decades. Although the initial implementation date was set for 1 January 2025, the new legislation will be introduced in phases, and commenced on 15 April 2025. It includes structural changes to ambulance services, the development of a new ambulance network and the introduction of a new professional role.
Structural changes to ambulance services
Several new types of ambulance crews will be deployed. One of the most notable is the hybrid rapid medical assistance (RLP)/rapid medical aid (RZP) model, whereby a physician-staffed RLP unit will operate during daytime hours, and an RZP crew without a physician at night. This measure is designed to optimize the use of physicians, whose availability in the Slovak health system is limited.
Another innovation is the RZP crew with extended-scope specialist paramedics. These paramedics will be authorized to perform advanced medical interventions previously reserved for physicians, with the intention of accelerating care delivery, particularly in remote or underserved areas.
The reform also introduces specialized ambulance types, including:
- Planned transport ambulances for non-emergency inter-hospital transfers and selected low-acuity primary calls, freeing doctors and paramedics for acute cases.
- Mobile paediatric intensive care unit ambulances, operated by tertiary paediatric healthcare facilities, to ensure critically ill children are transported by personnel trained in paediatric emergency medicine.
- Emergency medical assistance ambulances for repatriation (if a patient is abroad and needs transport back to Slovakia) and other non-insurance-covered transport needs, such as medical coverage at social, cultural and sporting events.
Development of a new ambulance network
The EMS network will be redesigned based on a mathematical optimization model that uses historical data on response times, call volumes, call types and geographic distribution of incidents. This model will propose optimal crew deployment to minimise response times and maximize coverage.
As a result, the number of ground ambulance service stations in Slovakia will increase from 321 to 344 from the next tendering period, beginning in Autumn 2025. Additionally, the reform specifies more precise regulations for the location of EMS stations in regional capitals to improve equitable access across urban areas and surrounding municipalities.
A commission within the Ministry of Health will monitor compliance with newly established quality indicators for both EMS providers and emergency dispatch centres. The first set of indicators was published in the Official Gazette in mid-2025, with systematic measurement scheduled to commence in 2026.
Introduction of a New Healthcare Professional Role
The legislation also creates a new category of healthcare worker: the transport assistant. Transport assistants, similar in status to nurses within the EMS system, will be formally registered with the Slovak Chamber of Emergency Medical Technicians. This ensures both professional representation and access to continuous professional development opportunities.
Another key feature of the reform is the planned introduction of a new emergency telephone number, 116117, in January 2026. This number will handle non-urgent medical inquiries, thereby alleviating the workload on the existing emergency number 155, which will continue to be reserved for urgent, life-threatening cases. The aim is to enable EMS teams to concentrate their resources on critical incidents requiring immediate intervention.
References
Fekete, B. (2025) Vláda schválila najväčšiu reformu záchraniek za posledné roky. Čo nás čaká? (The government has approved the biggest reform of the emergency services in recent years. What can we expect?). MEDICINA Trend. Available online from: https://medicina.trend.sk/2025/03/12/vlada-schvalila-najvacsiu-reformu-zachraniek-za-posledne-roky-co-nas-caka
Jeseňák, Š., Gaston, I. and Majerský, F. (2025) František Majerský & Gaston Ivanov: Najväčšia reforma záchrannej zdravotnej služby za 20 rokov s cenovkou 1,2 miliardy € (František Majerský & Gaston Ivanov: The biggest reform of the emergency medical services in 20 years, with a price tag of €1.2 billion). Ozdravme.sk Available online from: https://www.ozdravme.sk/Dokument/101831/frantisek-majersky-gaston-ivanov-najvacsia-reforma-zachrannej-zdravotnej-sluzby-za-20-rokov.aspx
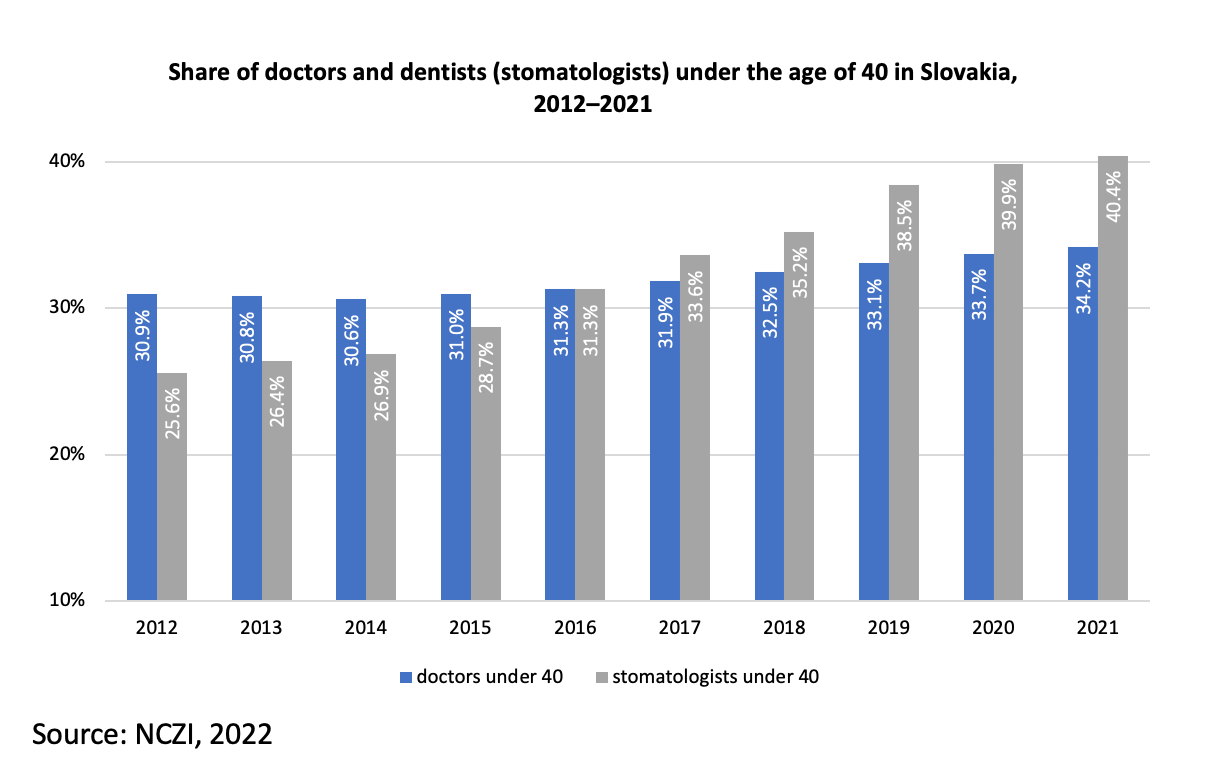
The share of young dentists has increased rapidly over the last ten years. According to National Health Information Centre (NCZI), in 2021, dentists under the age of 40 represented 40.4% of all dentists in Slovakia – this stood at just above a quarter of all dentists (25.6%) in 2012. This rising trend is much more dynamic than among doctors, where the share rose from just under 30.9% to 34.2% over the same time period (Fig 1).
Fig 1
One main reason behind this rapid growth of dentists is the financial benefits. According to profesia.sk [1], the largest HR portal in Slovakia, the monthly salary (in 2023) of a dentist is around 5 000 EUR (approximately four times the average salary of 1 304 EUR [2]), creating a huge gap between their salaries and the average Slovak wage.
With the strong financial security coming with being a dentist, the number of dental students in Slovekia has increased dramatically since 2010 (Table 1). According to Employment Institute (IZ) data [3], there were 514 dental students, across all grades, in 2010; this rose to 664 students in 2022 (an increase of nearly 30%). These figures only cover students with Slovak nationality and exclude foreign students (around 280–300 annually and stable at that level).
Table 1

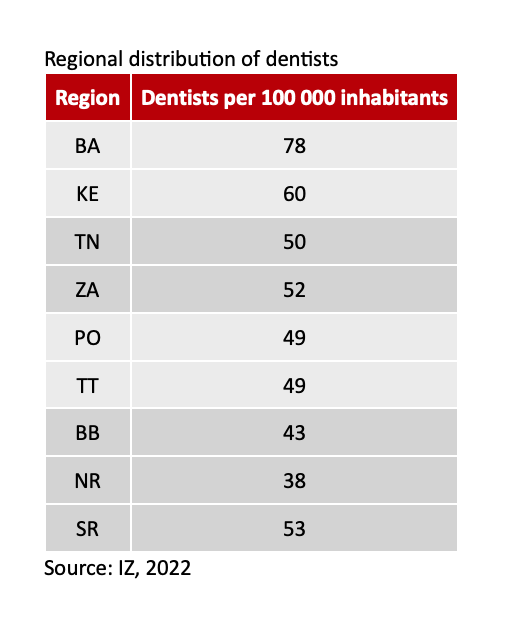
According to Igor Moravčík [4], the president of Slovak Dental Chamber, the problem in Slovakia is not the number of dentists, but their non-proportional geographical distribution. This is confirmed by IZ, as according to their analysis [5], there are 78 dentists per 100 000 inhabitants in the Bratislava (capital) region, which is much more than other regions (for example, there are 38 per 100 000 in the Nitra region) (Table 2).
Table 2
Authors
In response to the deteriorating state of health care in the country, highlighted by poor government response to four waves of COVID-19, the trade union of doctors in Slovakia (“LOZ”) declared an emergency in April 2022 and an intent to strike. LOZ announced that if conditions for doctors employed in Slovak hospitals had not improved by the end of summer 2022, they would consider the full-fledged strike via a mass resignation of doctors from hospital employment; LOZ claimed that up to 3 000 doctors declared an interest to participate in the strike (TASR, 2022).
Unions and chambers of other medical professions also joined the declaration, though not LOZ’s intent to strike and/or resign.
The four demands from LOZ in April were as follows:
- a systemic solution for the salaries of nurses and doctors employed in hospitals, reflecting the salary landscape across the Visegrád Four countries;
- a financing system for hospitals to avoid having to treat below cost;
- support for medical faculties so in producing more high-quality Slovak doctors and reforms to educating and training doctors; and
- proportional increases in personnel and available space in hospitals for departments that take on care provision from other decommissioned departments or hospitals via the “Optimization of the hospital network” project (LOZ, 2022).
Public opinion and that of professionals in Slovakia was initially supportive; even the Slovak President, Zuzana Čaputová, acknowledged demands from LOZ months before, that is, during winter 2021 (LOZ, 2021), as all Visegrád countries but Slovakia significantly increased health financing during the pandemic, including wages.
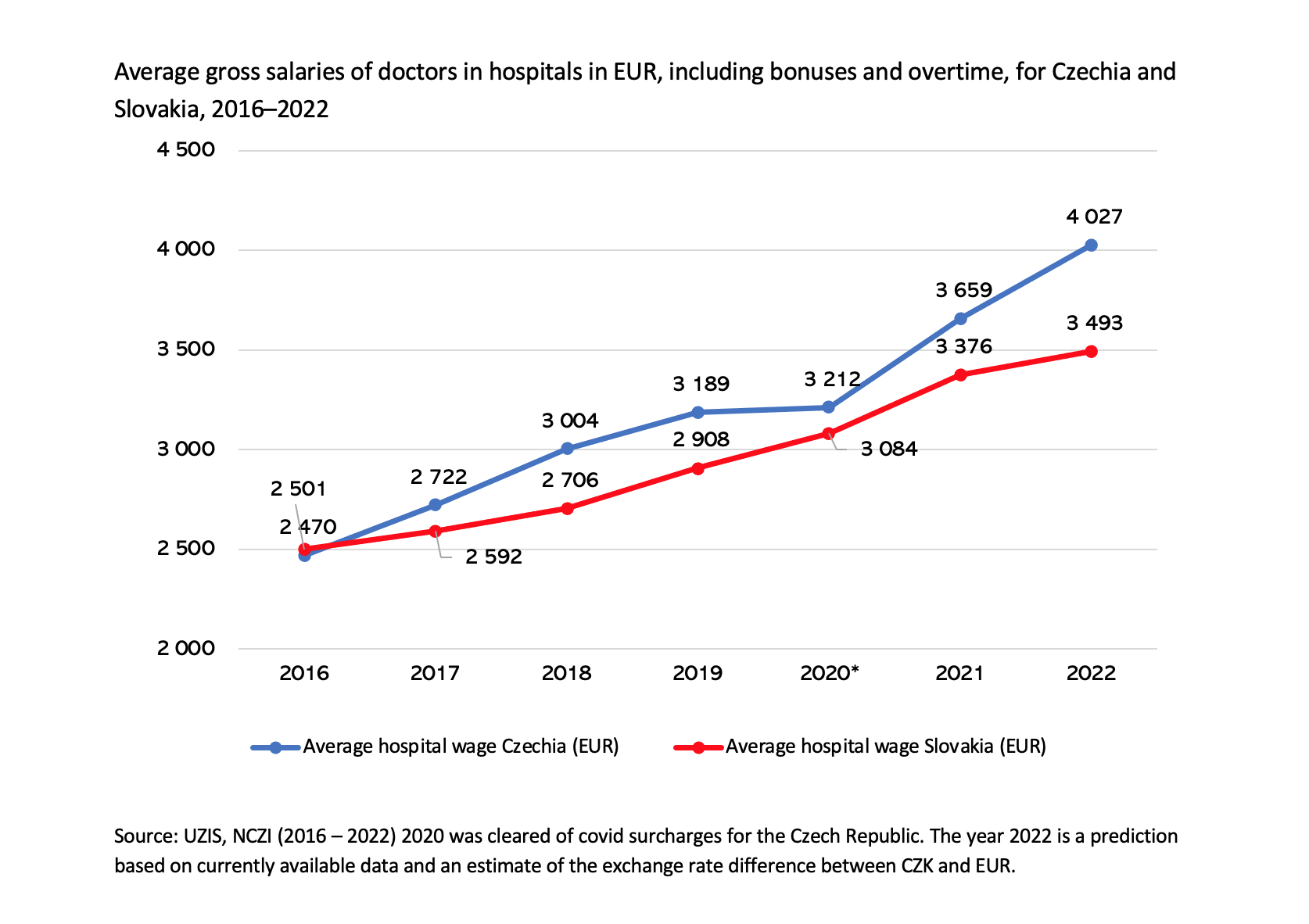
While the average gross salary of doctors in Slovak and Czech hospitals was at par in 2016, Czech salaries outpaced Slovak salaries beginning in 2017, due to the implementation of a plan increase salaries in Czech (public) hospitals (Fig.1). The biggest jump occurred during the pandemic, with the difference in 2022 growing to roughly €530 per month, on average. LOZ’s list of demands then grew to eight by the end of summer 2022 to include further changes in education, taxation and enforceability of legislation. However, the primary point of conflict between LOZ and the government remained compensation.
Fig.1
Slovak Parliament approved a wage increase for hospital workers, as prepared by the Ministries of Health and Finance, on 5 October 2022. LOZ was not satisfied with the increase, however, and it came days after more than 2 100 doctors had handed in their notices on 1 October, starting their two month resignation period.
The government’s increase comprised a two-fold change in the legislation governing hospital workforce remuneration: first, every hospital employee would receive a bonus based on every year of experience (up to 20) by a 0.01 multiple of average wage in Slovakia and second, every profession would see base salary increase based on a pre-defined multiple of the average wage in the industry. Thus, each profession received a profession-specific increase, depending on a relative wage comparison between Slovakia and Czechia; the aim was to ensure that relative wages (compared to the average industry wages of the respective countries) would be the same or better in Slovak hospitals.
The approved increase would raise doctors’ wages in hospitals, on average, to €3 970 in 2023 (a 14% increase). LOZ demanded €5 510 (a 58% increase), knowing such a number would not be feasible, they wanted at least the same increase as nurses (whose increase on average was 28%) and hence gave notice. Increases for other professions ranged from 10% to nearly 30%.
The government and LOZ did reach an agreement in the hours just before 1 December, that is, the end of the notice period, and the average wage of a hospital doctor is set to be roughly €4 580 in 2023, i.e., 30% more than in 2022.
The government furthermore agreed on all other remaining conditions of LOZ and signed a memorandum that details all steps that the government will take over coming years (MoH, 2022). Doctors withdrew their resignation notices on 30 November.
The wage increases are likely to cause a series of issues, as the broad increases are set only for hospital workers and are not tied to any quality or efficiency parameters. The Finance Ministry has not provided funds for outpatient providers, for example, who have consequently requested a €600 million increase in the budget, i.e., 24% more than in the planned budget for 2023, which is set to rise by 6% (SITA, 2022).
Authors
References
LOZ (2021) TA3: Zdravotníci žiadajú zvýšenie platov. Prezidentka ich požiadavku podporuje (TA3: Health workers are asking for a salary increase. The President supports their request) Lekárske odborové združenie – LOZ. Available from: https://www.loz.sk/ta3-zdravotnici-ziadaju-zvysenie-platov-prezidentka-ich-poziadavku-podporuje/
LOZ (2022) Vláda svojou nečinnosťou nedáva lekárom na výber (By its inaction, the government does not give doctors a choice). Lekárske odborové združenie – LOZ. Available from: https://www.loz.sk/vlada-svojou-necinnostou-nedava-lekarom-na-vyber/
MoH (2022) Vláda podpísala memorandum s Lekárskym odborovým združením (The government signed a memorandum with the Medical Trade Union). Ministry of Health of the Slovak Republic. Available from: https://health.gov.sk/Clanok?memorandum-lekari-vlada
SITA (2022) Kríza je zažehnaná. Lekári hromadne stiahli výpovede a nastúpili do práce (The crisis is over. Doctors withdrew their resignations en masse and went to work). Slovenská infromačná a tlačová agentúra. Available from: https://spravy.pravda.sk/domace/clanok/649003-kriza-je-zazehnana-lekari-hromadne-stiahli-vypovede-a-nastupili-do-prace/
TASR (2022) Lekárski odborári vyhlásili štrajkovú pohotovosť (Medical trade unions declared a strike emergency). Aktuality. Available from: https://www.aktuality.sk/clanok/PLG69a1/lekarski-odborari-vyhlasili-strajkovu-pohotovost/)
The Ministry of Health has updated wage coefficients in legislation in order to achieve relative parity with the Czech Republic for hospital sector employees. This was done in response to labour unions representing health workers declaring a strike to force an increase in salaries. Before the amendment, the average gap in monthly salary between the Czech Republic and Slovakia for a doctor (in a hospital) was roughly EUR 550, while the gap for nurses was roughly EUR 600.
The wage coefficient updates were codified into law via an amendment to Act 578/2004, approved on 5 October 2022. The legislation comes into effect on 1 January 2023. Relative to the average wage in the health sector, wages of doctors and nurses are set to be on par with those in Czechia. In absolute terms, even after the increase, there will be a difference of EUR 250–350, depending on type of specialty and other factors, such as the exchange rate.
Authors
Medical Doctors
In 2018, there was a shortage of 3.338 medical doctors in both in-and outpatient care to fulfil the minimum staffing levels (MoH, 2018). In relative term, this translates into a shortage of 20 % of the total medical workforce in Slovakia. If accounted for those medical doctors, who already passed retirement age, the shortage would even further deteriorate to 5.515 missing medical doctors (or roughly 30% of the total medical doctor workforce in 2017).
In a projection that assumes no changes to overall health care delivery (e.g. heightened need due to an ageing population) and number of medical graduates, only a total of 3.141 doctors is missing by 2030 (expecting that retirement age will be 64 years). This decline is driven by a steady slow increase in the number of medical students and graduates, as well as improving demographics of medical doctors.
As a reaction to this serious shortage, the MoH jointly with the Ministry of Education expanded universities capacities to accept additional 200 medical students as of the academic year 2018 / 2019. This measure is based on the evaluation that a majority of medical graduates pursue their medical career in Slovakia. Based on the long-term statistics, 82% of graduates who have completed their medical degree enrol in the medical profession in Slovakia.
Nurses
Similarly, there was a shortage of 3.550 nurses in 2018 (or 11 % of the total nursing workforce), with an expected increase to a total of 9.934 by 2030 (or roughly a third of 2017 nurse workforce). This increase is due to the demographics of the nursing workforce, which means a lot of nurses are expected to retire by 2022. Additionally, there is a significant outflow of 56 % of nursing graduates, because they either change their profession or leave to work abroad. According to the Chamber of Nurses (2017) the difference in salaries between Slovakia and neighbouring countries, insufficient competencies and the as unattractive perceived position of nurses in the system and their high workload of nurses are key reason to this outflow.
As for now, the MoH focussed on the monetary side of this outflow to reverse the trend:
- In 2019, the minimal coefficient was increased by 10 % for all non-medical professions. This translated into an additional budget of 58.9 million EUR for in-patient and 17.8 mil. EUR for outpatient care in 2019.
- Furthermore, there was a conditional scholarship introduced which is worth EUR 2.000 a year for students of bachelor's degree in nursing if the student work for at least 5 years in the Slovak nursing workforce.
Other measures
In the meantime, also medical personnel from other (Eastern) European countries is important. Although a majority of immigrated health personnel is from bordering countries e.g. the Czech Republic, there are also initiatives to help the migration from the Ukraine and Serbia. To further support their integration and to heighten their chances to pass the required language and professional examination, foreign-trained personnel can be placed for a year in Slovak hospitals as of September 2019. The recruitment of personnel started in summer 2019 and is welcomed by most hospitals (TASR, 2019).
Authors
References
Chamber of Nurses (2017) Vyjadrenie pre TREND [Announcement for TREND magazine]. [Online] Available at: https://www.sksapa.sk/z-cinnosti-komory/vyjadrenie-pre-trend.html (accessed 28 July 2019).
MoH (2018) Informácia o stave zdravotníckeho personálu v Slovenskej republike - nové znenie [Information on the state of medical personnel in the Slovak Republic - new version]. [Online] Available at: https://rokovania.gov.sk/RVL/Material/23194/1 (accessed 28 July 2019).
TASR (2019) Slovenské nemocnice majú záujem o lekárov z tretích krajín [Slovak hospitals are interested in doctors from other countries] [Online] Available at: https://mediweb.hnonline.sk.
4.2.1. Health workforce trends
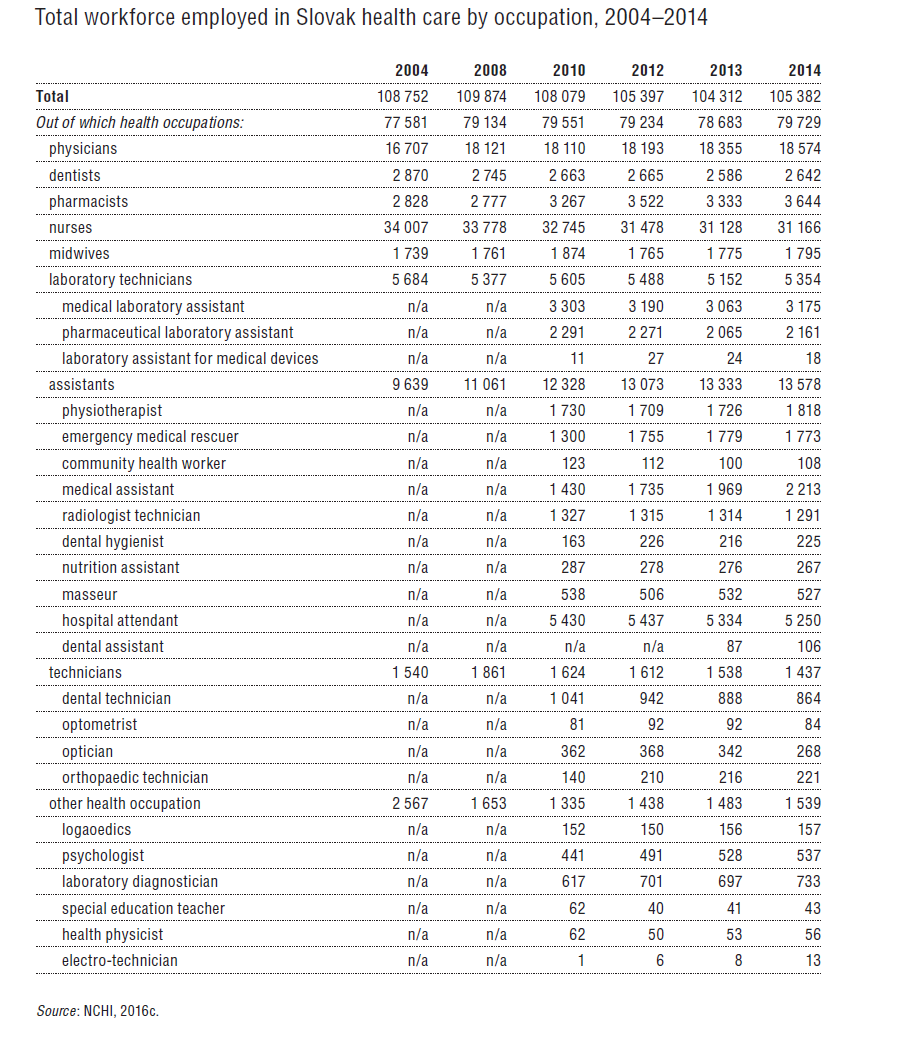
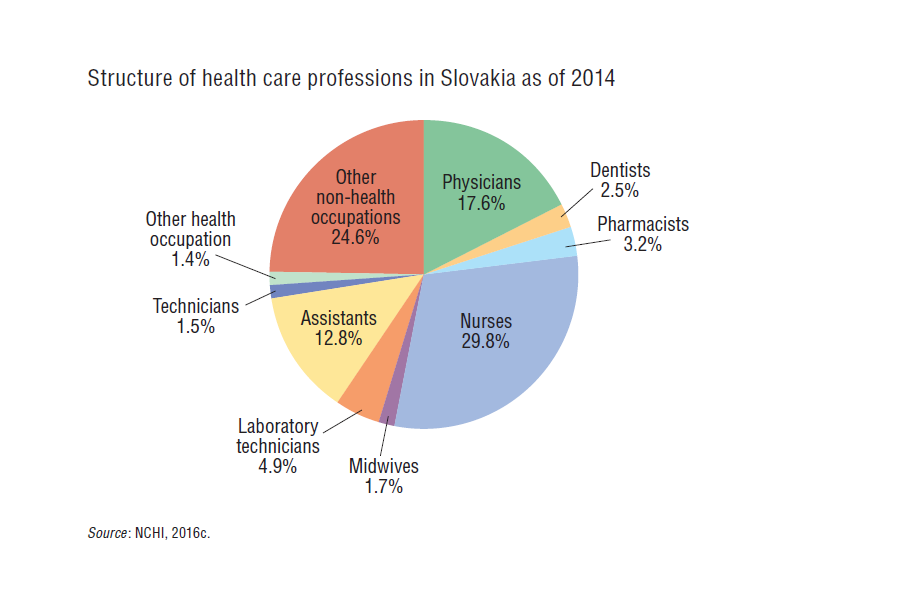
As of 2015, 105 382 people were employed in the health care sector, representing 4.5% of the Slovak workforce. Of the total employed health personnel 75.7% were medical staff, and the rest were non-health related, i.e. technical, educational and administrative staff. A detailed breakdown of the health workforce is shown in Table4.8, while an overview of the proportions is provided in Fig4.6. The workforce remains dominated by women, with females accounting for 78% of all health care employees and nurses are almost exclusively women (98%). Females accounted for 57% of physicians and dentists.
| Table 4.8 | Fig 4.6 |
 |  |
Only 47.8% of health workers are employed by non-state providers. After reclassification of health care facilities in 2008 and the gradual expansion of publicly owned hospitals, the proportion of state-employed health personnel increased to 52.2% in 2014.
In total, the health care workforce has decreased by 3.1% since 2004 (see Fig4.7) for various reasons. Changes to legislation by the Labour Code in 2007[7] restricted the number of hours that health employees can work per shift, partially resulting in an increase in total workforce in 2007 and 2008. On the other hand, contrary to the expectations, the decree defining minimum staffing levels in health facilities in 2008 led to a shift in personnel structure towards meeting the minimum ceiling. However, for a majority of providers this level was not sufficient to meet health care demands. Additional hiring led to an increase in workforce in 2010.
Fig4.7
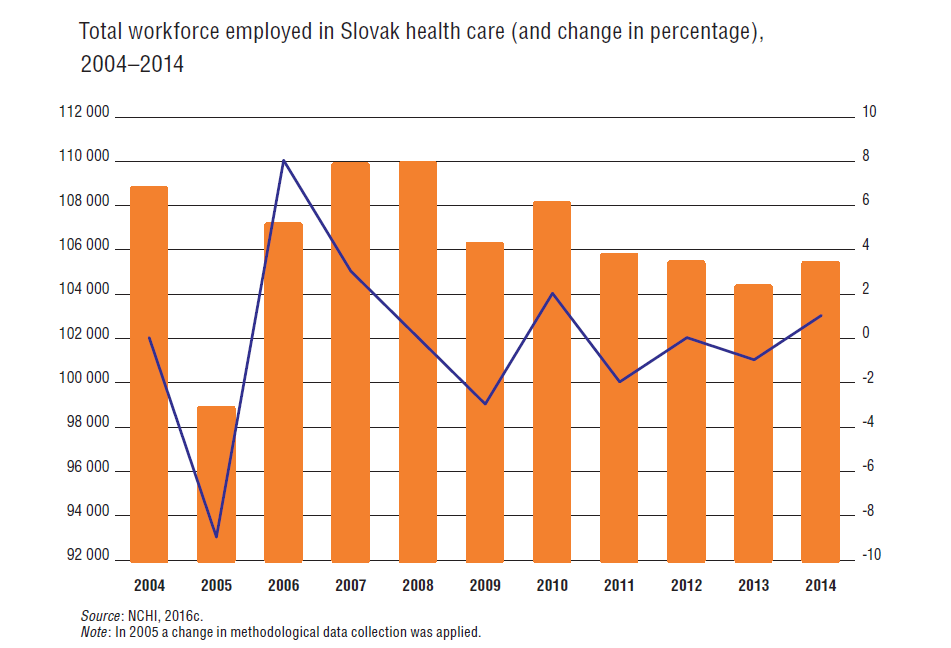
The total number of physicians has been gradually rising, whereas the number of nurses and other health personnel has been decreasing. Due to the introduction of minimum wages for hospital doctors, the profession is growing more attractive. Complying with the new legislation, general and specialized doctors’ wages increased by stages from January 2012 to January 2015 (see section 3.7.3). The average monthly salaries of doctors increased by 34.2% in 2011–2014 (compared to 7.8% for 2008–2011) (MoH, 2015).
Some indicators hint towards a positive impact of the minimum salary on the future health personnel of Slovakia, as the number of applicants to study medicine increased (see section 4.2.3). Secondly, the outflow of physicians from Slovakia has slowed down (see section 4.2.2). Thirdly, the minimum wage will help to counteract the ageing of the health workforce in Slovakia. The proportion of young doctors below 35 years increased from 19.8% in 2010 to 21.6% in 2014. Additionally, the rising attractiveness of medicine as a career choice in Slovakia may help to ameliorate the 970 vacant positions for physicians throughout the health care system (as of 2013 and estimated by the Ministry of Health) (NCHI, 2014a).
After nurses organized a petition entitled “When we will not take care of ourselves, who will take care of you?” the National Council adopted a resolution that required the government to prepare equivalent legislation on minimum wages for nurses and midwives. In March 2012 the policy was presented to the Ministry of Health, but only four months later it was reversed. A majority of providers raised the wages of nurses and midwives to comply with the legislation despite its short-lived nature, which resulted in an increase of 18.8% between 2010 and 2012 (SOZZAS, 2013). Even if this proved beneficial for nurses, it led towards the substitution of nurses with auxiliary staff, such as hospital assistants or attendants. Since 2004 the total number of nurses has decreased by almost 10% (see Table4.9 and section 3.7.3).
Table4.9
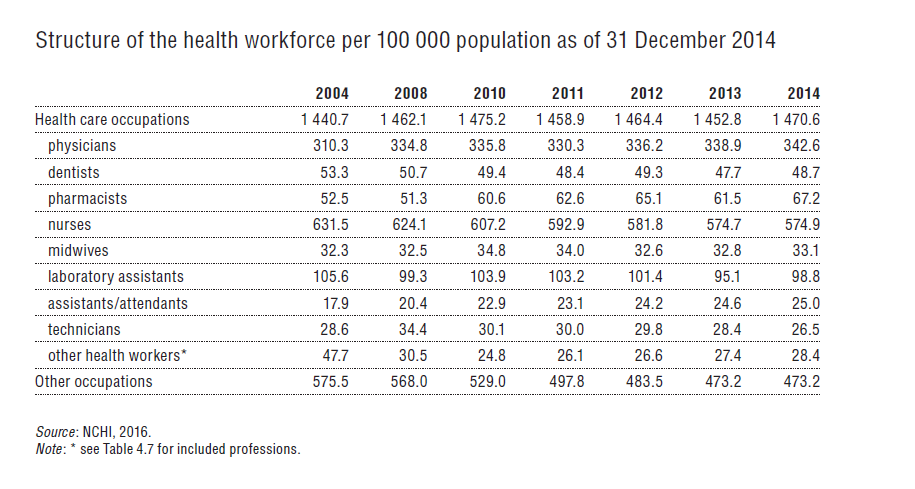
The missed opportunity to standardize minimum wages across the medical professions further exacerbated the shortage (Hunková, 2013). Moreover, younger professionals are attracted to higher wages abroad, thus advancing the ageing nursing workforce (SKSaPA, 2014). In 2010, 24.8% of nurses were younger than 35, but by 2013 this figure had declined to 16.2%. The proportion of nurses older than 50 years increased from 5.1% in 2003 to 33.6% in 2014. Since January 2016 new legislation governing minimum salaries of nurses and other nonmedical personnel could improve this situation. However, strikes preceding this act make it difficult to estimate its impact on the nursing workforce and the attractiveness of the profession (see section 3.7.3).
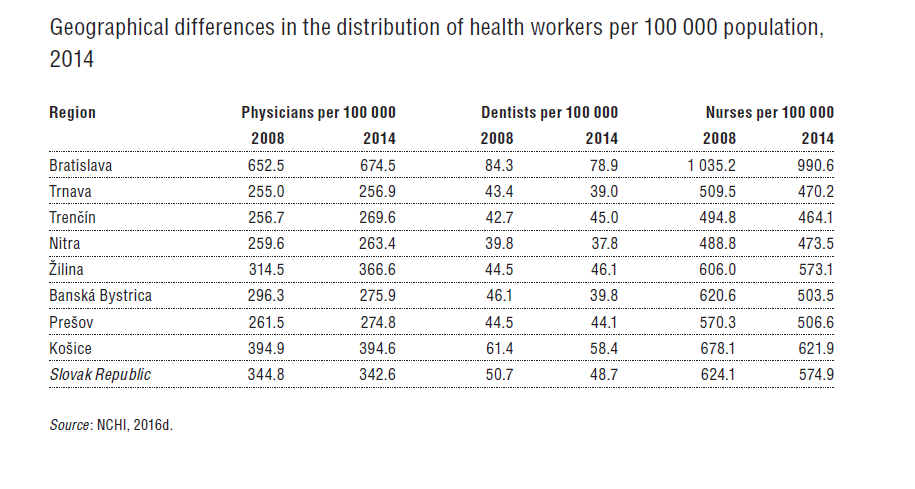
Since 2008 Slovakia has shown large disparities in the distribution of personnel. For example, Bratislava has 1.4 to 2.7 times more health workers on average per 100 000 population than other regions, and this has even increased slightly since 2008 (see Table4.10).
Table4.10
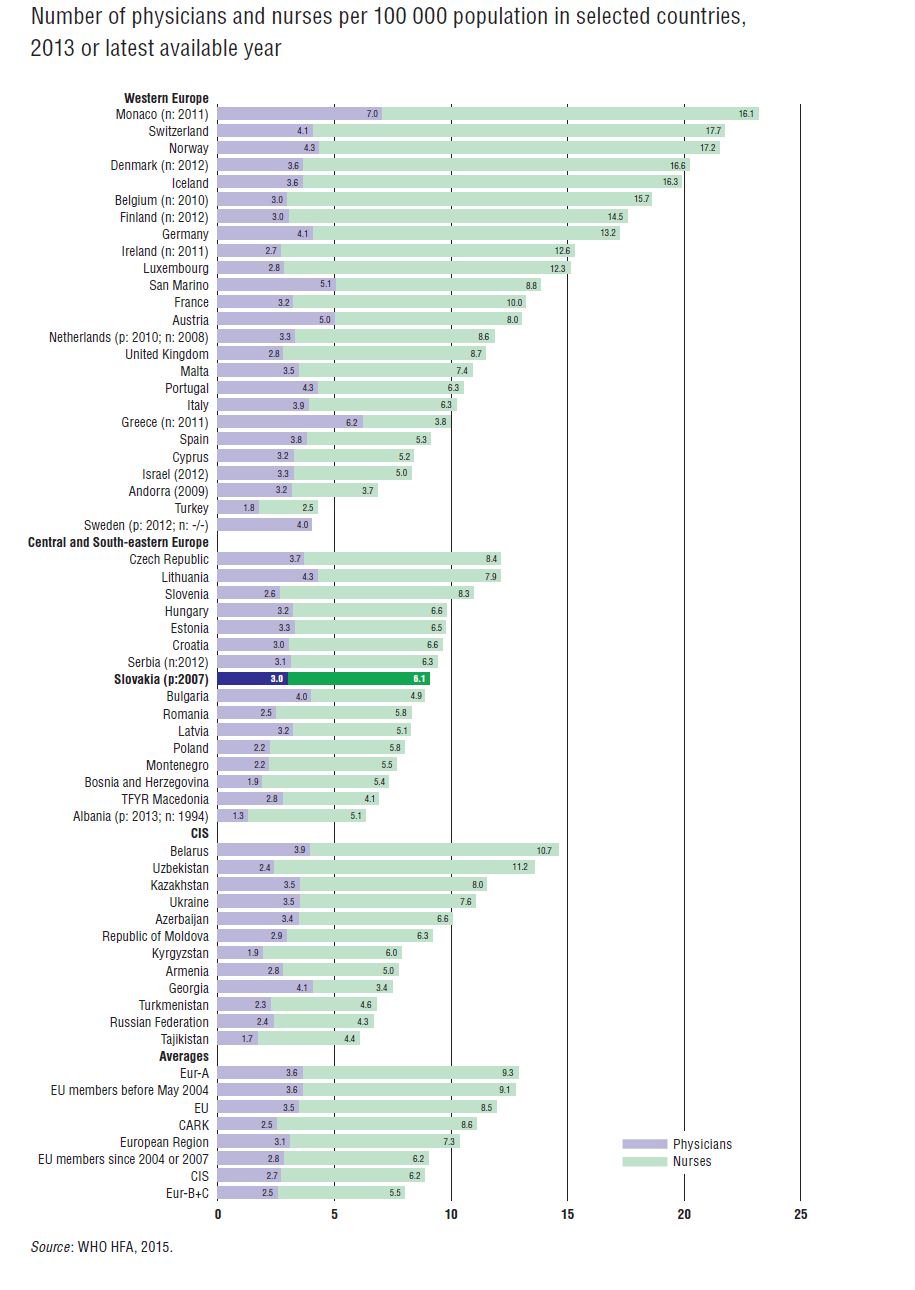
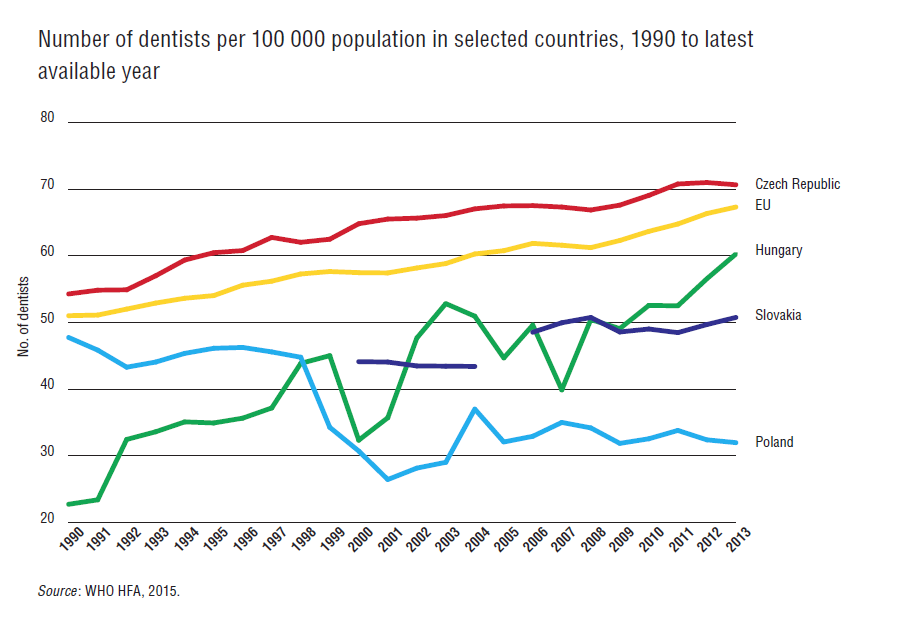
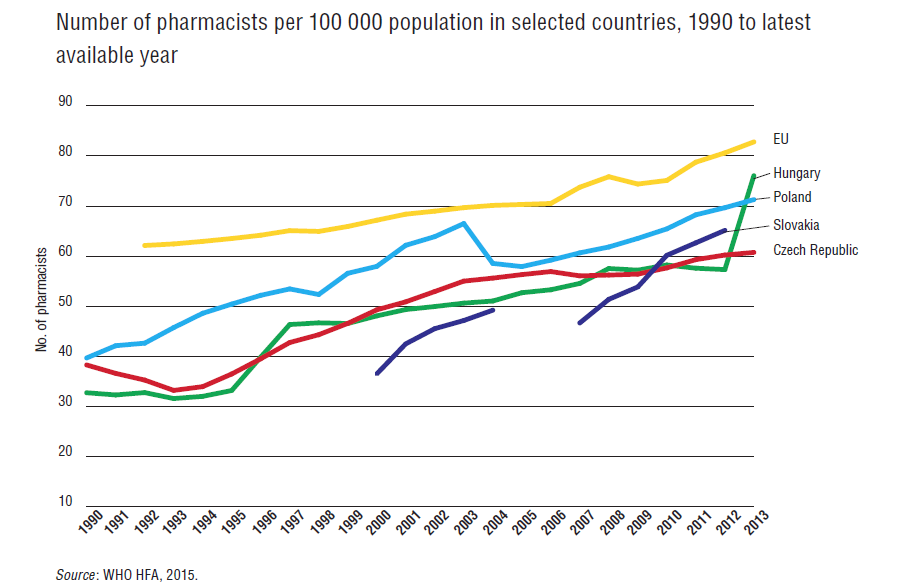
From an international perspective, Slovakia’s number of physicians was below the EU28 average in 2013 (see Fig4.8). In the same year Slovakia had 30% fewer nurses than the EU28 average and the second lowest number in the V4. Despite averaging slightly below the EU28 average, the number of dentists is increasing (see Fig4.9). The number of pharmacists is also steadily growing, with a 29% increase since 2004. Only the Czech Republic had fewer pharmacists employed (see Fig4.10). A change of methodology in data collection in 2007–2008 resulted in a peak across professional groups and limits comparability.
| Fig 4.8 | Fig 4.9 | Fig 4.10 |
 |  |  |
- 7. It transposed the EU Working Time Directive (2003/88/EC). ↰
4.2.2. Professional mobility of health workers
After implementing EC Directive 2005/36, Slovak health workers were allowed to work across EU countries. Higher remuneration in neighbouring countries such as Germany or Austria and good language capabilities among Slovak professionals have favoured mobility. The migration of Slovak health workers will likely cause shortages in the health care system despite increases in training capacities. As of 2013, about 2414 vacant positions existed in Slovakia’s health sector, with further deterioration expected in the future (Tiruneh et al., 2014) (see Fig4.11). This projection did not include outpatient private providers of care, so the total number of shortages could be even higher.
Fig4.11
Robust data on Slovak health professional mobility are lacking. Although a certificate of conformity of study issued by the Ministry of Health to health workers (see Table4.11) is required to work in a foreign country, it does not capture actual migration or migration outside the EU. Thus it only provides an indication of individuals willing to work abroad.
Table4.11
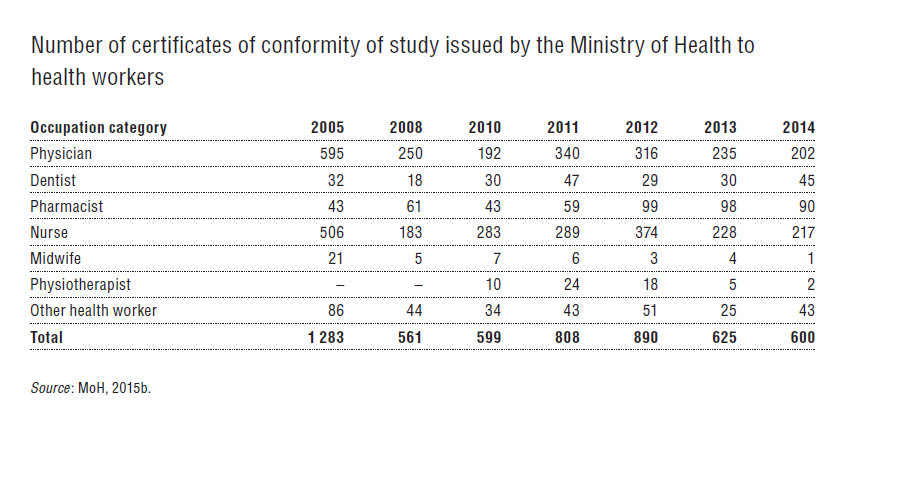
Between May 2004 and December 2014 the Ministry of Health issued 8087 certificates (7.7% of the total workforce), with a majority issued for nurses. The total number of certificates has decreased with the implementation of minimum wages. A threat to strike for increased salaries by doctors in 2011 coincided with an all-time high of 340 certificates requested. A similar development occurred in 2012 with nurses. Despite the suspension of nursing minimum wages, salaries still increased (SOZZAS, 2013). In 2013 the Ministry of Health began charging €250 for issuing certificates.
According to a 2007 statistical survey, Slovak physicians are most interested in working in Germany, the United Kingdom and the Czech Republic, while nurses preferred Austria. The Ministry of Health estimated that a total of 1620 Slovak doctors are pursuing their careers in other countries – the Czech Republic (1000), Germany (300), the United Kingdom (200) and Austria (120) (Beňušová, 2007).
Efforts to lessen the emigration of Slovak health professionals vary greatly and focus primarily on subsidizing study, improving working conditions and professional skills, and the aforementioned salary changes to raise the attractiveness of the Slovak health care system. In 2008 a pilot scholarship programme provided three-month grants to 110 doctors in specialized training. Following its initial success, the programme was extended in 2009 in order to provide longer scholarships and include nurses. Candidates signed a contract requiring them to either work in a relevant Slovak health facility or region at the end of their specialized studies for a period equivalent to the grant duration (typically one to three years, with a maximum of five years) or having to repay the grant. By 2012, 481 doctors and 864 nurses (including midwives) had benefited from the scheme, which cost €9.3 million and was mostly financed by the European Social Fund (ESF, 2016). Other ESF projects have aimed to improve health professionals’ clinical and managerial skills. From 2008 to 2012 the ESF and the Ministry of Health invested over €40 million towards the education and training of Slovak health professionals. Similar projects are currently in place for GPs (see section 6.2).
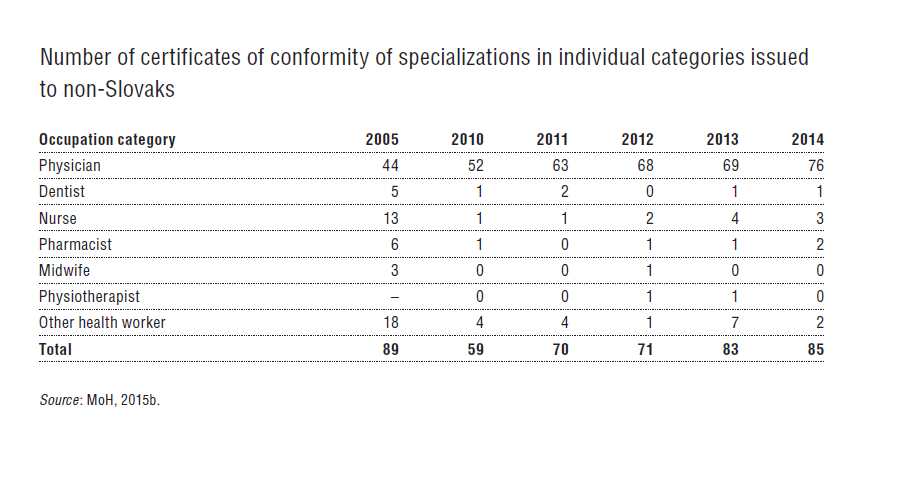
The majority of foreign professionals wanting to work in Slovakia come from the Czech Republic, Germany, Austria and France. The number of certificates of conformity of study issued to foreign professionals in Slovakia gives an indication of the inflow of doctors from abroad (see Table4.12). These figures are significantly lower than on the side of outflows.
Table 4.12
4.2.3. Training of health care personnel
A professional qualification to perform medical services can be conducted in universities, colleges or high schools. After the completion of a basic qualification, a student can obtain one of the following:
- Bachelor (Bc) degree
- Master (Mgr) degree
- Doctoral (PhD) degree
- Leaving certificate after completing secondary medical school
- Diploma on discharge to higher vocational education at a secondary medical school
- Certificate of final examination after completing secondary education
- “Doctor of Medicine” or “Doctor of Dental Medicine” title.
Doctors and dentists in Slovakia are educated in one of three universities (Comenius University in Bratislava, PJ Safarik University Košice and Slovak Medical University in Bratislava) and at four faculties (Faculty of Medicine in Bratislava, Jessenius Faculty of Medicine in Martin, Faculty of Medicine at UPJŠ Košice and the Faculty of Medicine at SZU Bratislava) which provide an accredited study programme in general medicine and an accredited degree programme in dentistry. Graduates receive either a “Doctor of Medicine” (abbreviated “MUDr”) academic degree or the academic title “Doctor of Dental Medicine” (abbreviated “MDDr”) for dentistry. Study programmes are comparable to those in other EU countries and are carried out in accordance with Directive 2005/36/EC (the recognition of professional qualifications).
Pharmacists are educated at two universities (Comenius University in Bratislava and the University of Veterinary Medicine in Košice). After completion of the master’s programme, graduates in the pharmaceutical programme undergo a rigorous examination to earn the title “Doctor of Pharmacy” (abbreviation “PharmDr”).
Nurses can study in an accredited nursing programme in accordance with Directive 2005/36/EC at eight universities or one private high school (Slovak Medical University in Bratislava, Faculty of Nursing and Health Professional Studies and Faculty of Health in Banska Bystrica, Catholic University, Faculty of Health, University of Health and Social Work of St Elizabeth in Bratislava, Constantine the Philosopher University in Nitra, Faculty of Health and Social Sciences, University of Presov, Faculty of Health Care Disciplines, Alexander Dubcek University, Faculty of Health, University of Trnava, Faculty of Health and Social Sciences, Comenius University in Bratislava, Jessenius Faculty of Medicine in Martin and UPJŠ Košice, Faculty of Medicine). After completing their education, nurses receive an academic bachelor degree comparable to those in other EU countries and the professional title of nurse. Graduates have the opportunity to pursue a master’s degree and earn the title of “Master” (abbreviated “Mgr”).
Midwifery is taught at three universities (Comenius University in Bratislava, Jessenius Faculty of Medicine in Martin, Prešov University, Faculty of Health Professions, Slovak Medical University in Bratislava, Faculty of Nursing and Health Professional Studies) in accordance with Directive 2005/36/EC.
Since 2004 further education of health professionals has been provided by educational institutions other than the Slovak Medical University in Bratislava, which still educates the highest number of health workers in Slovakia. In 2014 the Slovak Medical University conducted training in more than 130 accredited programmes for specialized training, certification training and continuing education for all health professions. Doctors can specialize in 49 accredited specialized study programmes which are eligible for automatic recognition in other EU Member States that comply with the requirements of Directive 2005/36/EC, as well as 46 programmes of specialized training (lasting three years) and 33 certified activities. A dentist can pursue further education in two specialized programmes eligible for automatic recognition in other EU Member States and six additional specializations. Health workers may also pursue the third level of higher education (PhD) to continue towards a scientific and teaching career (i.e. associate professor or professor at a university).
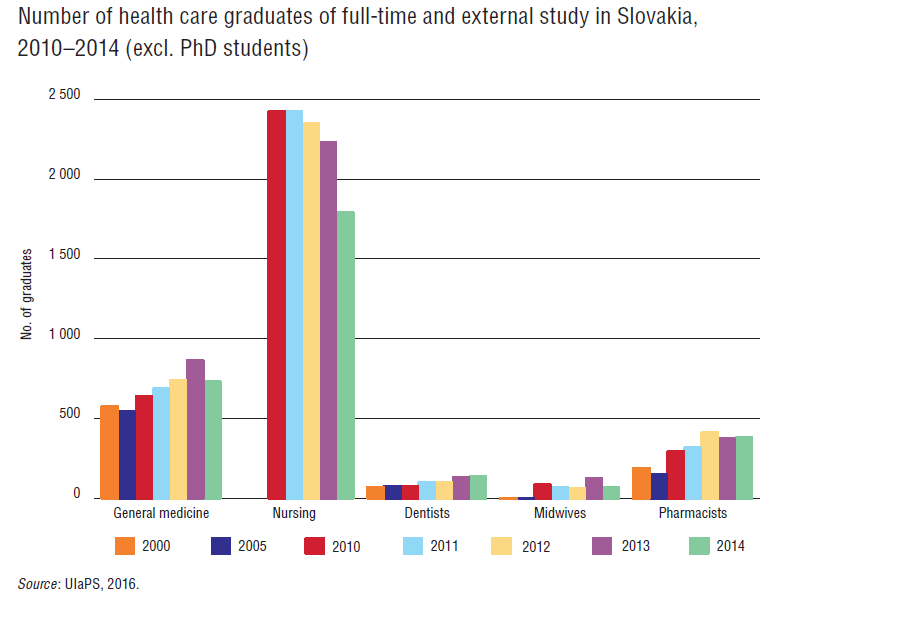
The number of graduates and enlisted students of medicine and dentistry has steadily increased while the number of nursing graduates has gradually declined. The number of graduates for selected years is depicted in Fig4.12.
Fig4.12
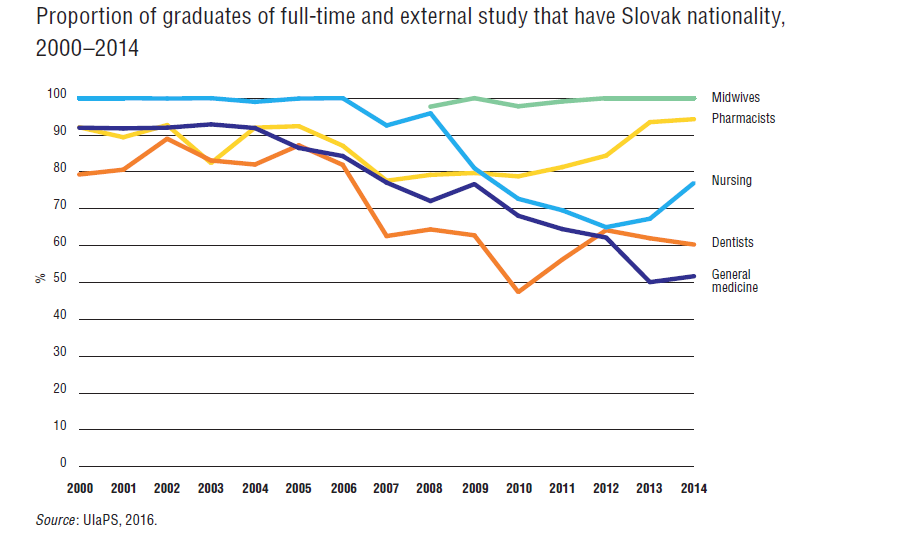
Although these changes might seem to be a consequence of the aforementioned changes in legislation on minimum wages and the restructuring of health care providers, a main driving factor is an influx of foreign students into Slovakia. As Fig4.13 shows, the proportion of Slovak graduates has significantly decreased since 2006. In fact, in 2014 only 51.7% of new students of medicine were Slovak and 40.5% of new graduates of nursing were foreign students (UIaPŠ, 2016). In 2012, for the first time in history, one of the medical universities – Jessenius University in Martin – had more foreign than domestic enlisted students. A majority of foreign students come from Greece, Norway, Poland or Israel (Pažitný et al., 2014).
Fig 4.13
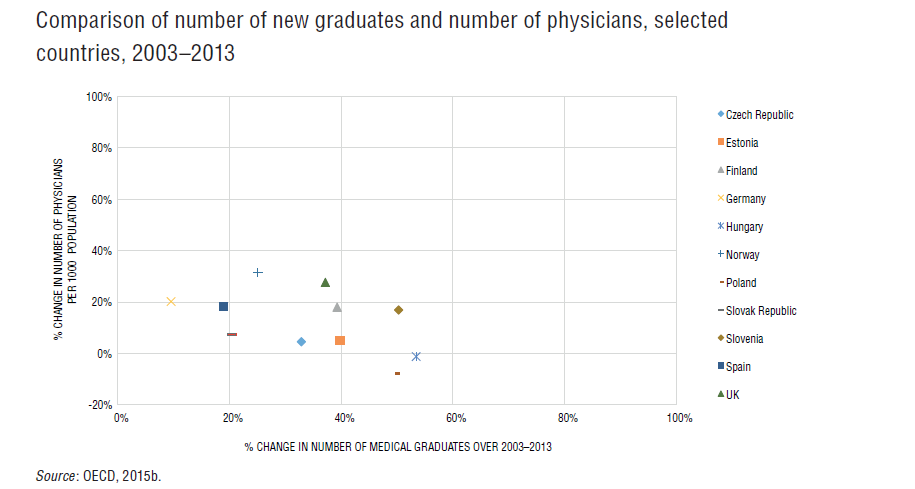
Increasingly, foreign students leave Slovakia after graduation to pursue their careers elsewhere. The increase in medical graduates will neither broaden the health workforce in Slovakia nor reverse the lack of health professionals (as depicted in Fig4.11). This phenomenon is shared amongst the V4 countries (see Fig4.14) and other EU Member States. Slovakia had a 20% increase in total number of graduates, but only a 7% increase in total number of physicians, whereas Hungary experienced a 57% increase in the number of graduates and a slight decrease in the number of physicians (OECD, 2015b).
| Fig 4.11 | Fig 4.14 |
|  |
The Ministry of Health has amended several aspects of health care workforce education throughout the year in 2022.
- As a response to staff shortages during the COVID-19 pandemic, health care facilities have been empowered to use trainee doctors and nurses as fully qualified employees. They perform their duties under the supervision of qualified experts.
- At the same time, the Ministry of Health has clearly defined practical teaching in medical facilities – in university and faculty hospitals, practical teaching takes place for university study fields, specialization fields and certified work activities in all medical professions. For other health workers – psychologists, speech therapists, medical pedagogues, physicists and laboratory diagnosticians – completion of the mandatory six-month training for working in the health sector has been repealed.
Further education of health care workers has also been adjusted. With regard to specialized studies and certification preparation:
- After the probationary period, a health care worker can ask their employer to submit an application for inclusion in a specialized study. After agreement with the worker, the employer submits the application no later than 30 days after its delivery.
- The educational institution enrols students in courses throughout the year, with the exception of residency studies.
- Medical procedures and professional practice completed in Slovakia, as well as abroad, and professional practice beyond the scope of the established weekly working hours can be included to count towards the mandatory requirements of the specialization study.
The Ministry of Health has also amended several aspects regarding the recognition of education obtained outside the Slovak Republic, including the option for temporary professional internships for persons who received their medical education in third countries, and several steps to relax bureaucratic requirements for submitting required documents and shortening the terms of recognition of documents for the further education of health workers.
These changes have not proven sufficient, since labour unions representing Slovakia’s physicians requested further changes. Hence, the Ministry of Health announced in October 2022 that it will update the processes on the specialization training of physicians in order to make the process more decentralised and flexible. These further measures are in response to several long-running factors, a main one being (and supported by surveys) that most younger doctors who have left Slovakia for Czechia declared that it was because of:
- rigid processes regarding further education
- a lack of opportunities in their preferred field(s) of study
Authors
4.2.4. Doctors’ career path
Professional development for doctors depends on individual motivation and ambition which leads to variations in possible nationwide career paths.
- Doctors can stay without further specialization and work in a hospital with limited scope of practice.
- Doctors can obtain a specialization in one of the specialty fields, acknowledged by the EU (e.g. surgery, internal medicine, obstetrics and gynaecology) and practise across all EU states without limitation on their scope of specialization. Certain requirements exist for each specialization in terms of length of training, rotations and the number of procedures performed.
- In hospitals, doctors can progress from senior physician to assistant medical director and medical director. In university hospitals, doctors may combine clinical duties with research activities.
- Doctors can obtain a licence that enables them to provide medical services as sole proprietor or become sponsors of another entity that provides medical guarantees for provision of care.
- Doctors can pursue research and conduct pure biomedical research or focus on lecturing at one of the medical universities while receiving a PhD degree.
4.2.5. Other health workers’ career path
Unlike medical doctors, there is no binding nationwide career path for other health workers. Pharmacists can decide to pursue a career in the private sector or choose to run a private pharmacy. Nurses can work in a hospital and progress to different specializations and levels of patient responsibility. Furthermore, nurses can choose to work in ambulatory settings or obtain a licence to provide either nursing services as a sole proprietor or run a nursing home and nursing care services. Other health care professionals, such as hospital auxiliary staff, do not follow a defined career path either.