-
09 March 2023 | Country Update
Excess mortality during the COVID-19 pandemic in Slovakia and a newly launched prosecution -
05 January 2020 | Country Update
Implementation of national cancer screening programmes in 2019
5.1. Public health
Public health operations are traditionally organized separately from health curative services and focus on the surveillance of communicable diseases. The Ministry of Health oversees the public health network in Slovakia, which is solely financed from the state budget. The PHA is the coordinating and supervising body of the network of 36 regional PHI throughout the country that act as executive bodies of the PHA. The PHA is headed by the chief hygienist, a post which is nominated and appointed by the Minister of Health.
The PHA conducts research, provides advice on methodology, and closely cooperates with the 36 PHIs in accordance with Act no. 355/2007. The PHA is also responsible for international cooperation in public health, initiating legislation (also harmonization with EU norms) and adopts measures for health promotion, health protection and disease prevention. The PHA has two main tasks that are kept separate.
- Firstly, it is responsible for monitoring environmental factors and population health status, as well as the promotion of healthy lifestyles through administration of prevention programmes for both communicable and noncommunicable diseases.
- Secondly, PHA focuses on epidemiological surveillance of communicable diseases and the health status of the population and conducting epidemiological and laboratory investigations. It also initiates containment or preventive measures as necessary. The PHA collaborates closely with the state veterinary authorities in incidences of food contamination and food poisoning.
Traditionally the PHA was mostly focused in the past on the second task, e.g. the prevention of communicable diseases, hygiene and sanitation. With the Act on Protection, Support and Development of Public Health in 2007 (Act 355/2007), the tasks of the PHA were broadened to reflect also the rising prevalence of NCDs.
This marked a substantial change in the PHA’s position and role. Given the high prevalence of NCDs (e.g. cardiovascular, oncological, metabolic and mental disorders, etc.), the new responsibility is of great importance to population health (see section 1.4).
With allocations less than 4% of the
total health budget for public health, Slovakia has a comparable budget
to other European countries (see Fig5.1). But a broader set of
responsibilities coupled with a fixed budget (and a cut during the 2008
financial crisis) hindered progress in developing public health. The
financial situation has been improving recently thanks to EU structural funding and linking new competences to financial means.
Fig5.1

In the current strategic national health programme, an intersectoral approach of care for individual patients’ and population health involving all relevant public and private actors is a key priority. This requires active involvement of the population in public health programmes aimed at nonmedical prevention of diseases by mitigating risk factors. PHA-led activities include smoking cessation programmes, community care or people-centred projects. Additionally, dedicated programmes target worsening public health indicators of socially disadvantaged communities in Slovakia (see section 5.14).
The basis for this key strategic document was the health policy framework “Health 2020” provided by the WHO Regional Office for Europe in 2012, which guides policy-makers in priority setting for public health. The Strategic Framework for Health 2014–2030 lists three strategic objectives that need reform to meet common objectives. These include (1) improved health status and well-being of the population, (2) reduction in health inequalities, and (3) universal people-centred health systems that are sustainable, equitable and of high quality (see section 2.5).
Since 1991 a register for communicable diseases run by the PHA has been a part of the epidemiological information system of communicable diseases (EPIS) that supplies data to WHO and ECDC. This register is the focus of infection control for Slovakia.
Enforced since 1986, the National Immunization Plan aimed to eliminate and eradicate vaccine-preventable communicable diseases by targeting children. It is updated annually based on WHO recommendations and reported incidences in the previous year. Vaccination against diseases listed in the plan remains compulsory as stipulated by Act no. 355/2007. The current list includes vaccinations against diphtheria, pertussis, poliomyelitis, pneumococcal pneumonia, Haemophilus influenzae, type B viral hepatitis, rubella, morbilli and parotitis. Vaccines and vaccination under the valid immunization plan are fully covered by HIC.
Historically, vaccination rates against major communicable diseases varied between 98–99% and low or zero incidences of vaccination-preventable diseases have been reported. The last registered case of poliomyelitis was recorded in 1960 and of diphtheria in 1980.
Since 2012 vaccination rates have been falling (see Table5.1), driven by the Bratislava region, which recorded a low 90.1% MMR vaccination rate for 2015 (PHA, 2016). In 2014 a group of vaccination opponents filed a case against this compulsory vaccination at the Constitutional Court of the Slovak Republic. The court ruled in favour of maintaining the policy as it does not breach human rights to privacy and integrity, but protects public health. Thus, parents who refuse to have their children vaccinated can be penalized (SITA, 2014). Between 2013 and 2014 the PHA registered 6209 refusals of compulsory vaccinations, of which 369 cases were charged a fine (PHA, 2014). This represents a 263% increase in fines compared to 2012 (Krempaský, 2015).
Table 5.1
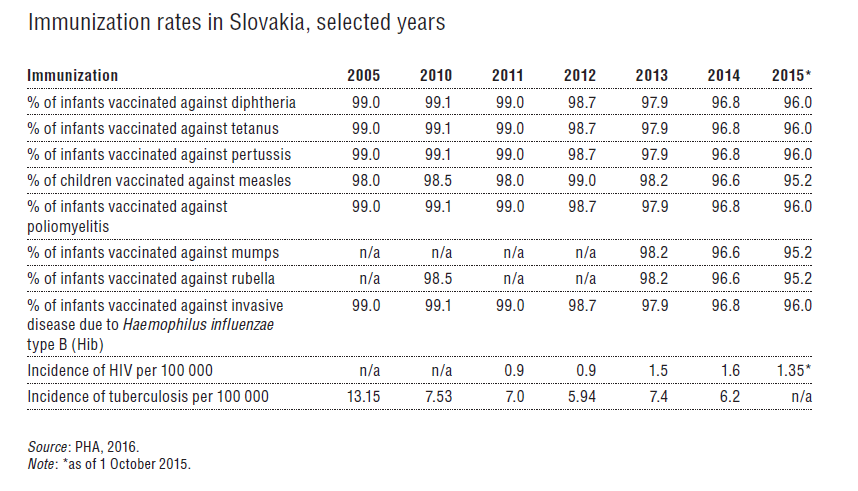
In 2012 compulsory vaccination against tuberculosis was taken off the list after tuberculosis incidence reached an all-time low at 5.94 per 100 000 inhabitants. The current increase to 7.35 in 2013 is worrying and is driven by an outbreak among the Roma minority. The incidence of type A viral hepatitis (VH-A) continues to decline thanks to childhood vaccination of children living in communities with low hygiene standards. In recent years viral hepatitis C has been on the rise, especially among drug users. The cumulative number of HIV-infected persons since 1985 has plateaued at approximately 550, but a substantial increase of new cases in 2014 poses a challenge for the future.
Health promotion and prevention of major chronic diseases
The paradigm shift towards more health prevention and promoting healthy lifestyles to mitigate NCDs in Slovakia is laid out in Act no. 355/2007. In 2014 the National Health Promotion Programme (NHPP) was adopted by the government in an intersectoral approach to minimize risk factors and consequences of risk behaviour.
The NHPP, through cooperation with health service providers, HICs and other relevant institutions (e.g. patient organizations and relevant NGOs), aims at the continuous improvement of population health status (see Box5.1). Based on health monitoring of the Slovak population through various national surveys, two priority areas were formulated to align with current WHO and EU strategies (Health for All, Health2020, EU public health policy, etc.)
Box 5.1

Implementation of these priority areas of intervention is realized
through several national programmes and action plans, either on a
regional level (children and adolescent health) or as an integral part
of the Slovak-wide public health system. In priority area A, the chief
activities are the National Action Plan for mitigating alcohol use and
the Plan for tobacco control. In priority area B the National Plan for
containing diabetes and cardiovascular diseases prevalence are the main
tools. A full list is shown in Box5.2.
Box5.2

Additionally, screening programmes exist for cervical, breast and colon cancer. Screening rates in 2013 were around 48% for cervical cancer, and 38.9% for breast cancer (compared to over 80% in Slovenia, Denmark, Austria and the Netherlands) (OECD, 2015). A National Plan for Cancer is necessary to achieve comparable targets, but it is not yet developed. Costs of screening programmes are fully included in the Slovak benefits basket.
Health promotion counselling centres were established as an integral part of PHA and PHIs to advise on health risk factors, healthy nutrition and physical activity, smoking cessation, mental health and stress management, and occupational health. They also provide non-pharmacological treatment for early stages of NCDs, advise on environmental factors, quality of housing, drinking and recreational waters, and can provide flu vaccinations. In 2015 the centres saw 10 384 clients, of whom 5964 were first-time users of these services. Altogether, the centres have seen more than 230 000 patients since 1993 (PHA, 2016). These centres organize various events to raise awareness about specific public health problems. Because of insufficient state funding of the government-adopted health promotion and primary prevention programmes, the activities and campaigns are often conducted and co-financed in partnership with NGOs and the private sector.
Evaluation of the public health system after the 2007 reform
With
the reorientation from communicable to noncommunicable diseases in
2007, a whole range of new competences, tasks and instruments were
introduced. In 2013 an evaluation of the public health system in
Slovakia was carried out in collaboration with the WHO Regional Office
for Europe using the EPHO (European Public Health Operations) Tool,
which mapped its strengths and weaknesses and proposed future measures
(see Box5.3)
Box5.3

The evaluation proposed several measures to improve the public health system in Slovakia by strengthening the systematic monitoring of health, creating an independent institution for the coordination of health promotion and preventive programmes, and improving the educational standards of the public health workforce.
When looking at the development of excess mortality in the Slovak Republic (third-highest in the EU27 over the analysed time period, see Table 1), the second (September 2020 to May 2021) and later also third waves (September 2021 to May 2022) saw Slovakia record a high number of infections and deaths. The exception was indeed the first wave of the pandemic (March to May 2020), during which the hard lockdown introduced very quickly brought the expected results and numbers remained low.
While the strong second wave was primarily the result of neglected preparation (planning, contact tracing, testing), chaotic political decisions often without a scientific basis (population-wide rapid antigen testing), inappropriate communication to the public and the late introduction of a hard lockdown, the main problem in the third wave was the politicization of COVID-19 vaccinations (inconsistent support across the political spectrum, scandal with the Sputnik V vaccine, and the unsuccessful vaccination lottery) leading to only 51% of the population being vaccinated and another late-introduced lockdown.
Although all EU countries recorded an increased excess mortality during the pandemic, a more detailed comparison shows that the situation in Slovakia was particularly unfavourable (reaching 70% at the peak of the wave, a total of 26,786 excess deaths were recorded). Hypothetically, it is even possible to quantify the number of lives that could potentially be saved if the same anti-pandemic measures as in selected EU countries had been introduced in Slovakia. Based on country benchmarking for instance, if Slovakia had followed the same pandemic measures as Estonia or Denmark, up to 12,391 or 21,308 fewer deaths, respectively, could have occurred. This could have also been the case with higher vaccination rates, that is, Slovakia would have recorded 14,483 fewer deaths with the same vaccination rates as Portugal.
As a result of this, then Minister of Health Krajčí resigned on 11 March 2021, followed by then Prime Minister Matovič on 30 March 2021. One reason specifically given from the official government website for the coalition’s collapse was the purchase of the Sputnik V vaccine. Nearly two years later, on 6 March 2023, Slovakia’s Attorney General confirmed the launch of a criminal prosecution (begun in January 2023) for (mis)management of the COVID-19 pandemic.

Authors
Authors
References
Ministry of Health (2019): https://www.health.gov.sk/?rok-prevencie
Ministry of Health: Licenced providers of colonoscopy: https://www.health.gov.sk/?skrining-kolorektalneho-karcinomu
Ministry of Health: Licenced providers of mammography: https://www.health.gov.sk/Clanok?dops-zamerana-na-zabezpecenie-kvality-namamografickych-preventivnych-a-diagnostickych-pracoviskach