-
30 December 2022 | Policy Analysis
Changes to workforce remuneration following the mass resignation threat of hospital-employed doctors -
08 October 2018 | Country Update
Update on the roll-out of DRGs as dominant payment mechanism for inpatient care
3.7. Payment mechanisms
As explained in section 3.3.3, providers are paid by HICs according to individual contracts, which determine the amount, the nature and quality of services. The guiding principles of payment mechanisms differ for primary and specialized ambulatory care, inpatient care, diagnostics, emergency and pharmaceutical services, as illustrated in Table3.12.
Table 3.12

For inpatient services, DRG as payment mechanism has been introduced
in 2017. However, there have been several safeguard measures in place
due to lower data quality and inexperience of the coders and in order to
prevent the possibility of hospital underfinancing. HICs have
implemented several safeguards, which included individual base-rates for
each hospital, dual coding (old vs DRG coding) – with payment linked to
the old coding, safety intervals (e.g. +/- 10% of the previous period
payments), and global budgets, which had to be linked to DRG reporting.
As of 2018, all HICs introduced global budgets based on previous
payments and DRG reporting.
Full implementation (means the use of a unified national base rate) is expected by 2021.
Authors
3.7.1. Paying for health services
Inpatient care
Inpatient care is defined as an overnight stay longer than 24 hours in any licensed health care institution (not only hospitals but also sanatoriums or nursing homes). Around 95% of all hospital revenues come from HICs. There are three different types of inpatient payment mechanism.
- Inpatient care is predominantly compensated via per case payment for a completed hospitalization related to the department of admission. A hospital will receive the same amount for a patient with colorectal cancer hospitalized in the surgical department as for a patient hospitalized with appendicitis. However, the hospital will receive different amounts for different patients hospitalized in the internal medicine or neurological wards. Per case payments differ not only among departments but also among hospitals. This is due to a lack of objective pricing mechanisms that would enable HICs to dictate the value of per case payments (see Table3.13 for an overview of pricing differences among hospitals). In case of a difficult or special inpatient treatment there is an opportunity to adapt the case payment in advance with a HIC. In fact, two HICs (GHIC and Dôvera) already use compulsory software that pre-approves such complex inpatient treatments. If a hospital performs above contracted limits, HICs will pay lower or no price for that care in a given period of time. In 2014 roughly 0.92% of total inpatient claims were regarded as above-limits. Except for volume limits, some HICs also imposed limits on the monthly revenues for hospitalizations.
- A few types of hospitalizations are paid with per diem payments, mostly long-term hospitalizations in internal medicine and psychiatry, as well as balneal treatment.
- Certain short-term hospitalizations, especially one-day and short-stay surgeries (i.e. inpatient stay of 24–72 hours) are reimbursed as a fee per service.
Table3.13

Pharmaceuticals, medical devices and dietary foods are included in hospitalization costs. In the case of expensive medical devices, health insurance covers the price above the limit set for hospitalization.
The introduction of DRGs in inpatient care is expected to bring increased harmonization in payments. The process of implementation is governed by HCSA and the German DRG was chosen as the basis. Since the beginning of 2016, the system has been used virtually; this means that a provider is provided with information on his DRG payment, but still receives reimbursement through the “old” payment scheme. It is expected that during 2016 all the implementation issues surrounding the introduction of SK-DRG can be settled before the system becomes operational.
Outpatient care
The payment mechanism for primary outpatient health care is a combination of capitation (see Table3.14) and fee for service. Fees apply to certain medical services not covered by the capitation but included in SHI benefits, such as preventive care, some costly examinations such as C-reactive protein, ECG or colorectal cancer screening, pre-surgical examinations, laboratory testing and treatment of essential hypertension.
Table 3.14

The amount of an insured person’s capitation payment is mostly age-dependent, but some HICs try to motivate GPs and offer them higher capitations after fulfilling some quality criteria. The system of capitation payment allows HICs to control costs but it does not motivate GPs to perform costlier or additional medical procedures since they bear all the risk.
Specialists in outpatient care are paid on a fee-for-service basis. Each medical procedure has an assigned number of points and HICs negotiate the fee for one point (point value) with health care providers. With this system, specialists have an incentive to treat patients, but the system may not motivate them to cure patients. This makes it difficult to control the volume and cost of provided services.
Therefore, most HICs negotiate a maximum volume of points to be reimbursed. If a health care provider exceeds the negotiated volume, the HIC does not have to reimburse the extra points. Whether the HIC will cover the costs or not depends on the negotiated contract. Alternatively, a differentiated point value may be applied after exceeding the monthly volume of points. In these cases, the point value decreases with the increase in number of procedures performed (degressive point value).
Like physicians in primary care, specialists may receive additional financial rewards from HICs, for example when there is positive feedback from patients or they prescribe rationally. Lastly, pharmaceuticals given to patients during outpatient visits are reimbursed to a physician in addition to the capitation and fee-for-service payments.
3.7.2. Paying health workers
Prior to 2005, health care personnel in inpatient care facilities were paid according to a uniform system for public servants. Since January 2005 the financing of personnel in inpatient health care facilities has been governed according to the Labour Code, allowing for individual agreements. Salaries depend on the outcome of collective agreements between the employees or employees’ representatives (trade unions) and the employers’ representatives. These agreements are decentralized, and consequently the salary level varies across the country.
In 2011 doctors’ dissatisfaction with their salaries led to strikes comparable to those in the Czech Republic in the same years and the mass resignations of physicians from hospitals. The government was forced to adopt a memorandum that legally declared the minimum threshold of salaries, both for certified and non-certified hospital doctors.
Complying with the new legislation, hospital physicians’ wages have been gradually increasing. As of January 2015 hospital physicians without specialization earn a minimum of 1.25 times the national wage average of the industrial sector, while those with a specialization earn at least 2.3 times the average sector wage. The process of increasing salaries was divided into four stages from January 2012 to January 2015 to make sure that providers had sufficient time to prepare for budgetary pressures (see Table3.15 for more information).
Table3.15

Nurses and midwives, perhaps inspired by the success of the physicians’ strike, successfully demanded a similar legislative guarantee of a minimum salary in 2012. This guarantee was approved by the government in February 2012, but revoked in June 2013 by the Constitutional Court as it was deemed discriminatory against other branches of health personnel. In 2015 the Ministry of Health prepared legislation that aimed at standardizing the minimum salaries of not only nurses and midwives but all paramedical staff in public hospitals. Minimum salaries were to be set in relation to national wages two years prior, with the applicable coefficient depending on specialty and achieved education. The trade union of nurses and midwives and the Slovak chamber of nurses and midwives criticized this draft because the proposed coefficients did not take into account experience. The Ministry of Health refused to alter the legislation, which led to a second wave of strikes of nurses and midwives in November 2015.
The strike saw 1374 nurses and midwives from seven public hospitals handing in their notice of resignation. However, only roughly 4% of nurses and midwives were represented. Although the Slovak president placed a veto on the minimum wage legislation in December 2015, the parliament re-approved the act and it came into effect from 1 January 2016. The strike did not accomplish the goals the nurse and midwives were aiming for. See Table3.16 for an excerpt from the act.
Table3.16

According to an official publication by the Ministry of Health (MoH, 2015b), the average salary of health professionals[6] employed in the public sector increased on average by 25.5% over the period 2010–2014. Compared to the average national monthly salary in the industrial sector for 2014 (i.e. €858), the average salary of a health professional was 19.2% higher (i.e. €1023, see Table3.17).
Table 3.17

- 6. Information includes all public providers of health services; information from private providers is not available in the required level of detail. Public providers employed 56% of all personnel active in the health care sector (see section 4.2). ↰
In response to the deteriorating state of health care in the country, highlighted by poor government response to four waves of COVID-19, the trade union of doctors in Slovakia (“LOZ”) declared an emergency in April 2022 and an intent to strike. LOZ announced that if conditions for doctors employed in Slovak hospitals had not improved by the end of summer 2022, they would consider the full-fledged strike via a mass resignation of doctors from hospital employment; LOZ claimed that up to 3 000 doctors declared an interest to participate in the strike (TASR, 2022).
Unions and chambers of other medical professions also joined the declaration, though not LOZ’s intent to strike and/or resign.
The four demands from LOZ in April were as follows:
- a systemic solution for the salaries of nurses and doctors employed in hospitals, reflecting the salary landscape across the Visegrád Four countries;
- a financing system for hospitals to avoid having to treat below cost;
- support for medical faculties so in producing more high-quality Slovak doctors and reforms to educating and training doctors; and
- proportional increases in personnel and available space in hospitals for departments that take on care provision from other decommissioned departments or hospitals via the “Optimization of the hospital network” project (LOZ, 2022).
Public opinion and that of professionals in Slovakia was initially supportive; even the Slovak President, Zuzana Čaputová, acknowledged demands from LOZ months before, that is, during winter 2021 (LOZ, 2021), as all Visegrád countries but Slovakia significantly increased health financing during the pandemic, including wages.
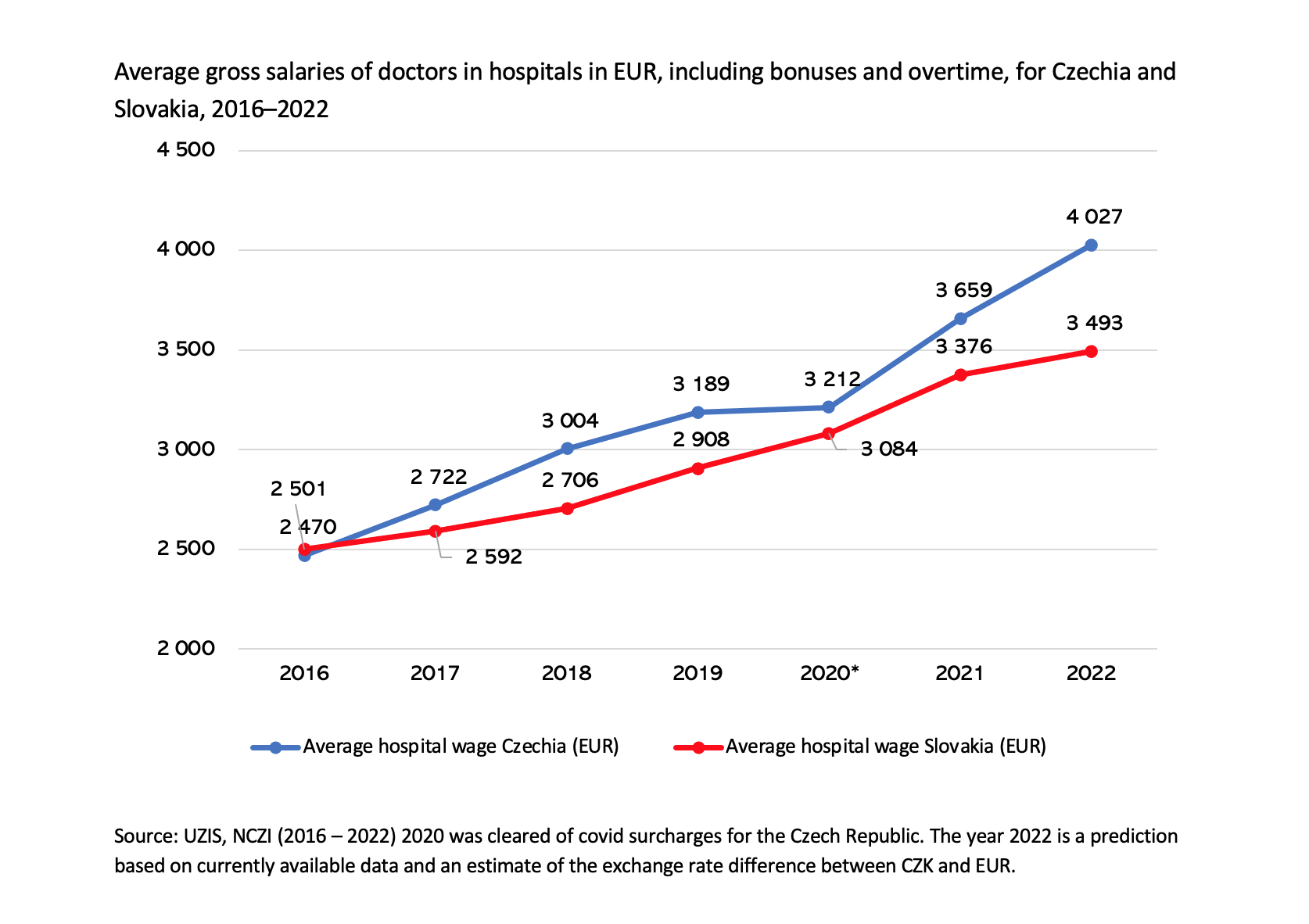
While the average gross salary of doctors in Slovak and Czech hospitals was at par in 2016, Czech salaries outpaced Slovak salaries beginning in 2017, due to the implementation of a plan increase salaries in Czech (public) hospitals (Fig.1). The biggest jump occurred during the pandemic, with the difference in 2022 growing to roughly €530 per month, on average. LOZ’s list of demands then grew to eight by the end of summer 2022 to include further changes in education, taxation and enforceability of legislation. However, the primary point of conflict between LOZ and the government remained compensation.
Fig.1
Slovak Parliament approved a wage increase for hospital workers, as prepared by the Ministries of Health and Finance, on 5 October 2022. LOZ was not satisfied with the increase, however, and it came days after more than 2 100 doctors had handed in their notices on 1 October, starting their two month resignation period.
The government’s increase comprised a two-fold change in the legislation governing hospital workforce remuneration: first, every hospital employee would receive a bonus based on every year of experience (up to 20) by a 0.01 multiple of average wage in Slovakia and second, every profession would see base salary increase based on a pre-defined multiple of the average wage in the industry. Thus, each profession received a profession-specific increase, depending on a relative wage comparison between Slovakia and Czechia; the aim was to ensure that relative wages (compared to the average industry wages of the respective countries) would be the same or better in Slovak hospitals.
The approved increase would raise doctors’ wages in hospitals, on average, to €3 970 in 2023 (a 14% increase). LOZ demanded €5 510 (a 58% increase), knowing such a number would not be feasible, they wanted at least the same increase as nurses (whose increase on average was 28%) and hence gave notice. Increases for other professions ranged from 10% to nearly 30%.
The government and LOZ did reach an agreement in the hours just before 1 December, that is, the end of the notice period, and the average wage of a hospital doctor is set to be roughly €4 580 in 2023, i.e., 30% more than in 2022.
The government furthermore agreed on all other remaining conditions of LOZ and signed a memorandum that details all steps that the government will take over coming years (MoH, 2022). Doctors withdrew their resignation notices on 30 November.
The wage increases are likely to cause a series of issues, as the broad increases are set only for hospital workers and are not tied to any quality or efficiency parameters. The Finance Ministry has not provided funds for outpatient providers, for example, who have consequently requested a €600 million increase in the budget, i.e., 24% more than in the planned budget for 2023, which is set to rise by 6% (SITA, 2022).