-
12 June 2024 | Country Update
Building three new regional hospitals -
16 August 2023 | Country Update
Increasing influenza vaccination coverage -
16 August 2023 | Country Update
Increased capacity to undertake investments in health infrastructure -
15 June 2020 | Country Update
Total number of hospital beds to remain unchanged until 2022 -
21 May 2017 | Country Update
Total number of hospital beds unchanged until 2019
4.1. Physical resources
One of the reforms included and covered by the Romanian Recovery and Resilience Plan was to increase the administrative capacity of central and local authorities to efficiently manage health infrastructure projects. This resulted in setting up and launching the National Agency for Health Infrastructure Development (ANDIS) in 2022 (https://andis.gov.ro).
The first major assignment of ANDIS was to take over from the Ministry of Health the project to plan, construct, equip, furnish and operationalize three regional emergency hospitals in Cluj, Craiova and Iași. The preparation stages were implemented under the coordination of the Ministry of Health until the end of 2013. At the time of writing (June 2024), construction work has started. Also, a call for proposals has been launched for technical assistance for the operationalization of the hospitals and the development of a transition plan, including the development of a human resources strategy and an assessment of training needs.
The construction of the three regional hospitals is an investment of over 2 billion euros. Funding sources include the 2021–2027 EU Health Programme (1.25 billion euros), the 2014–2020 regional Operational Programme (141 million euros), European Investment Bank (EIB) loans (923 million euros) and the state budget.
The National Plan for Hospital Beds, which represents the total number of beds for which hospitals can conclude contracts with health insurance houses, is approved every three years by the government. The Government Decision 337/2020, effective from 4 May 2020, approved the National Plan for Hospital Beds for 2020–2022, setting a limit of 119 579 beds for each of the coming three years. This number has remained unchanged since 2016.
The 2016 decrease in the number of beds reflected the increase in the volume of services provided within primary and community care settings and the rationalization in the use of hospital services which were envisaged by the National Health Strategy 2014–2020 and occurred between 2011 and 2016. During this period, the number of beds decreased by 15 392.
The National Plan for Hospital Beds for 2017–2019 has been approved by the Government Decision 115/2017. The Plan envisages a stable number of hospital beds over the coming three years, setting for each year a maximum limit of 119,579 (the value of 2016).
The expected changes related to the number of beds, in the light of the National Health Strategy 2014–2020, are: a decrease in the number of acute beds and an increase in the number of beds in long-term care, rehabilitation and palliative care, for which there is a large demand uncovered.
More information (in Romanian):
http://lege5.ro/Gratuit/ge2tgmbuhaza/hotararea-nr-115-2017-privind-aprobarea-planului-national-de-paturi-pentru-perioada-2017-2019
http://www.ms.ro/wp-content/uploads/2016/10/Anexa-1-Strategia-Nationala-de-Sanatate-2014-2020.pdf
Authors
4.1.1. Capital stock and investments
Current capital stock
In 2014, there were 527 hospitals in Romania. Of these, 366 were public hospitals (69% of the total) and 161 were private (31%) (see section 5.4 for information on the classification of public hospitals). While the number of public hospitals decreased by 15% between 2008 and 2014, the number of private hospitals increased by over four times. Overall, the total number of hospitals increased by 15% between 2008 and 2014 (National Institute of Statistics, 2015a).
The decline in the number of public hospitals was driven, mainly, by the closure, in 2011, of 67 public hospitals due to their not fulfilling certain criteria (see Table6.1) (Official Gazette, 2011). Local authorities as owners of these hospitals were recommended to transform the buildings into health care centres or nursing homes. However, since most of the buildings were in a very poor state, such transformations were deemed to be economically unviable. Following public and political pressure, many of the closed hospitals were reopened as hospitals or other health care facilities, e.g. LTC facilities, in the following years.
Table6.1
The largest increase in the number of private hospitals occurred from 2013 to 2014, following a change in the payment method for day surgery and day care cases in 2014 (see sections 3.7.1 and 5.4.1). The majority of new private hospitals are day care facilities that perform simple procedures. The number of private hospitals that report cases in the RO-DRG database rose from 73 in 2013 to 197 in 2014; out of these, 107 (54%) reported day cases only. The total number of hospitals reporting in the national DRG system in 2014 was 594 (197 private and 397 public). The difference between the total number of hospitals reported above and the number of hospitals reporting in the national DRG system is due to the fact that some health care facilities with beds (for example, among the health centres; see section 5.4) are not registered as hospitals but are paid like hospitals.
There is no officially available information regarding the condition of public hospital buildings. However, since the majority of public hospitals (over 90%) were built in the 1970s and 1980s (Ministry of Health, 2014) and have not been well maintained due to the scarcity of public resources, their technical condition is likely to be poor. Public hospitals are evenly distributed across the national territory, but are less easily accessible in certain geographical areas, such as the Danube Delta and remote mountain regions (see for example Ciutan & Chiriac, 2009). Almost 90% of public hospitals are located in urban areas and because transport costs can be high, accessibility in rural areas is further compromised (see section 5.1). Private hospitals are also mainly located in larger cities, in particular in the more affluent regions.
The 2014–2020 Health Strategy envisages a restructuring of the regional hospital network, which would include designation of strategic hospitals, investment in their infrastructure (this was also included in the Budgetary Strategy for 2014–2016; see section 2.8.1), and the building of seven new regional hospitals. It further envisages the transformation of local hospitals in small and medium-sized urban areas into units providing ambulatory care, day care or care for chronic patients. This would include reducing the number of hospital facilities (entire hospitals or departments within hospitals) and integrating selected facilities into new or refurbished regional hospitals, allowing for the closure of beds, streamlining of services and improvements in the coordination of treatment of complex cases requiring an integrated approach (Ministry of Health, 2014).
Investment funding
Investment funding into specialized care facilities is mainly covered from the budget of the Ministry of Health and the budgets of local authorities, whereas investment at the primary care level into primary care practices has to be covered by the owners of those practices. Transfers are made according to a pre-approved yearly capital investment plan, which is developed by the Ministry of Health in accordance with the strategic investment plans and with the technically documented proposals made by the health facilities. For example, in line with the infrastructure development objective of the Health Sector Strategy for 2011–2013, in 2012 the Ministry of Health spent 361.9 million lei (€81 million) on the refurbishment of eight hospital buildings, plus 152 capital repair works and one feasibility study for the building of a regional hospital. In 2013 it spent 92.5 million lei (€21 million) on the refurbishment of nine hospital buildings and 47 capital repair works (Ministry of Health, 2013).
The second largest source of capital investment funding is from the World Bank and EU structural funds. For example, the Romania Health Sector Reform Project, conducted between 2005 and 2013 with funding from the World Bank, supported the development of feasibility studies, technical analyses and architectural designs for the refurbishment of 20 hospital maternity units, as well as the renovation of emergency departments in 17 hospitals (World Bank, 2014).
Other sources of investment funding include the NHIH and public–private partnerships (P–PPs), but these play a small role. Until 2014, it was not possible to use funding received for the reimbursement of service delivery through the NHIH for capital investment purposes but the legislation around this was amended in 2014 (see section 2.8.6). However, given the low levels of public funding, not many hospitals have been able to fund capital investments from this source.
The Law on Public–Private Partnerships was issued in Romania in 2010 but P–PP initiatives have been obstructed by numerous limitations of this Law (Government of Romania, 2015) and technical problems with its implementation. For example, although the legislation provided that the selection and awarding of P–PP notices were to be published exclusively through a dedicated section of the electronic public procurement system, P–PP contracts were only included in this system in 2013. The central government and local authorities have expressed interest in using P–PPs for the building or refurbishment of hospitals and other health facilities but there are no public data on the number of partnerships that have been set up. A new draft law on P–PP was proposed in 2014 and is still under debate at the time of writing (December 2015) (for more detail, see DPIIS, 2015).
4.1.2. Infrastructure
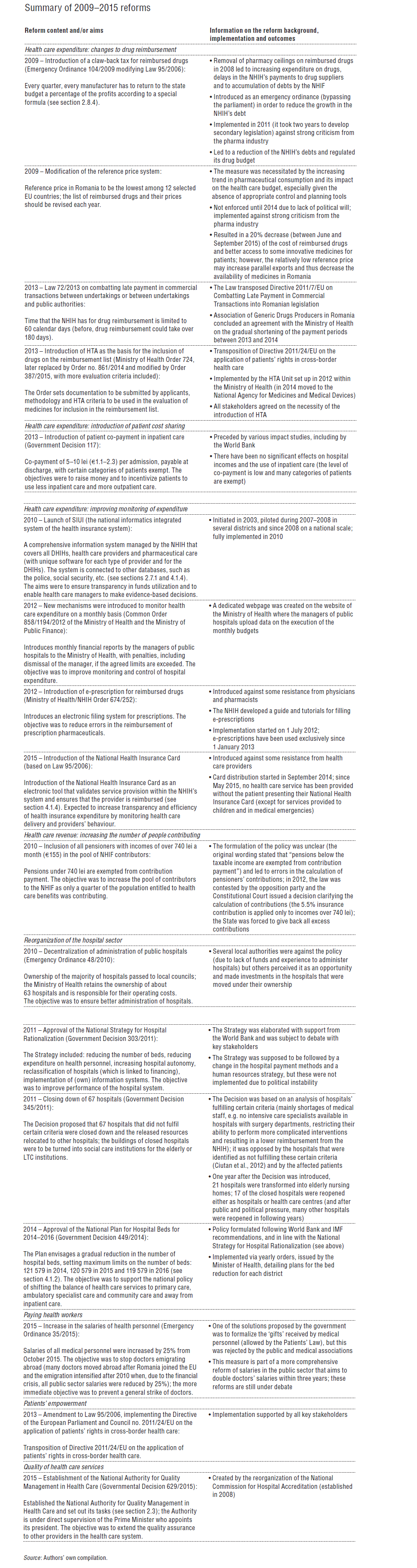
The total number of hospital beds per 1000 population decreased from 7.9 in 1990 to 6.3 in 2013 (Fig4.1). This is lower than the number of beds recorded in the majority of comparator countries, except for Bulgaria (also 6.3 in 2013), which range from 7.4 in Poland to 13.3 in Hungary, or the EU, at 11.7 (WHO Regional Office for Europe, 2016). This decreasing trend is in line with the government’s efforts to decrease the number of hospital beds and strengthen the role of primary care (see sections 5.3 and 5.4). Important reductions took place in 1992 (from 7.9 to 6.8), when excess beds were cut in departments with low occupancy rates (mainly maternity wards, following the decrease in the birth rate after the abolition of the abortion ban; see section 1.4), and in 2003 and 2010 as a means to enhance efficiency (19 912 or 12% of beds were closed in 2003 and 8266 or 6% in 2010). Additional reductions occurred in 2011 in the context of the aforementioned closure of 67 hospitals (a reduction of 3%). Policies to reduce the number of hospital beds were further enforced by Decision no. 449 of 2014 on the approval of the National Plan for Hospital Beds for 2014–2016, which made the reimbursement of hospital services by the NHIH subject to limits on the total number of beds in Romania (everything above the total number will not be paid for from the health insurance funds). These limits are: 121 579 hospital beds in 2014 (there were 125 798 beds in 2013), 120 579 in 2015 and 119 579 in 2016 (Official Gazette, 2014b).
Fig4.1
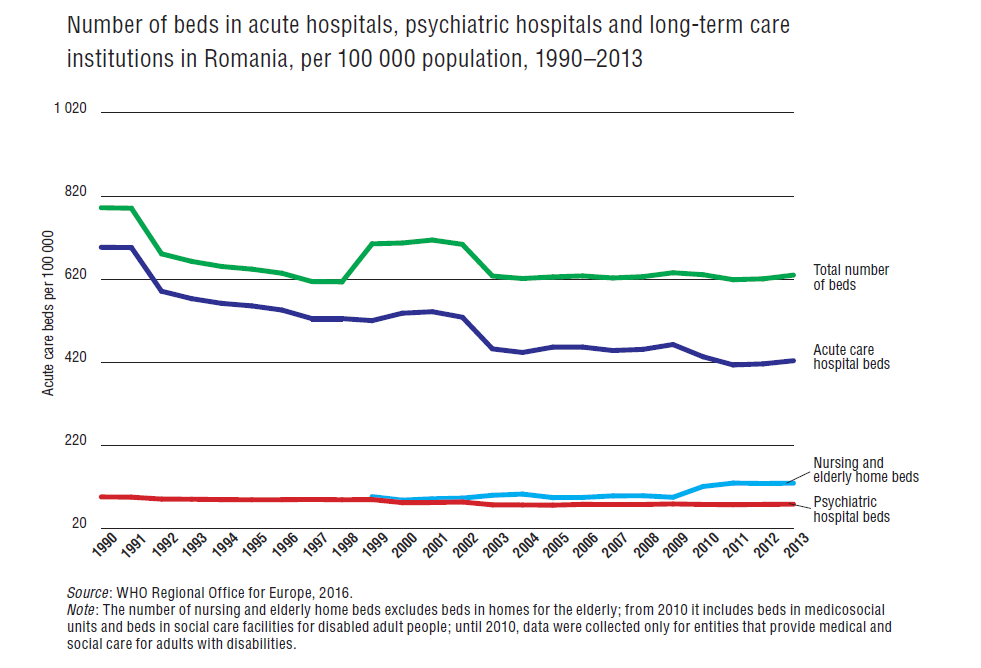
Much of the observed decline in hospital beds was in the acute care sector, with beds falling by almost 60% between 1990 and 2013, from 7 to 4.2 per 1000 population. The 2013 figure was the same as in Slovakia and Poland (4.2 and 4.3, respectively), but higher than Hungary (4) and the EU average (3.6) and lower than the Czech Republic (4.4) and Bulgaria (5.2) (Fig4.3). The number of psychiatric beds per 1000 population fell by almost 20%, to 0.8 in 2013, which was the same as in Slovakia but higher than in Poland (0.6), Bulgaria (0.7) and the EU average (0.7) and lower than in Hungary (0.9) and the Czech Republic (1). The number of beds in nursing and elderly residential care facilities increased from 0.96 per 1000 population in 1999 to 1.3 in 2013. Comparisons with other countries are difficult due to differences in the definitions of nursing and elderly home beds (WHO Regional Office for Europe, 2016).
Fig4.3
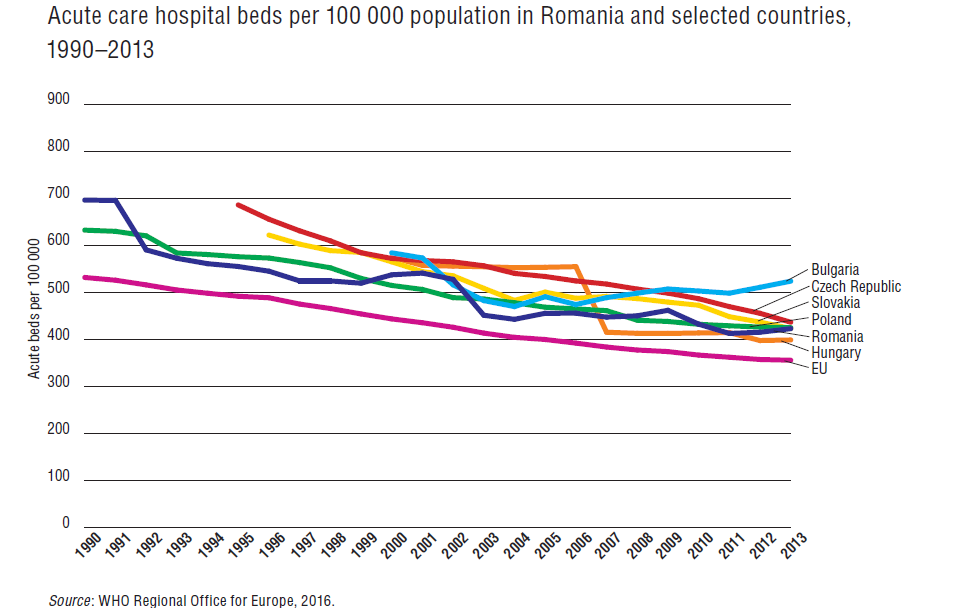
The ALOS in acute care hospitals was 6.3 days in 2013 (down from 6.6 days in 2009) (Fig4.2, a). This is similar to Slovakia (6.2) and the EU average (6.3) and higher than Hungary (5.2 in 2012), the Czech Republic (6.6) and Poland (6.7) (WHO Regional Office for Europe, 2016).
Fig4.2
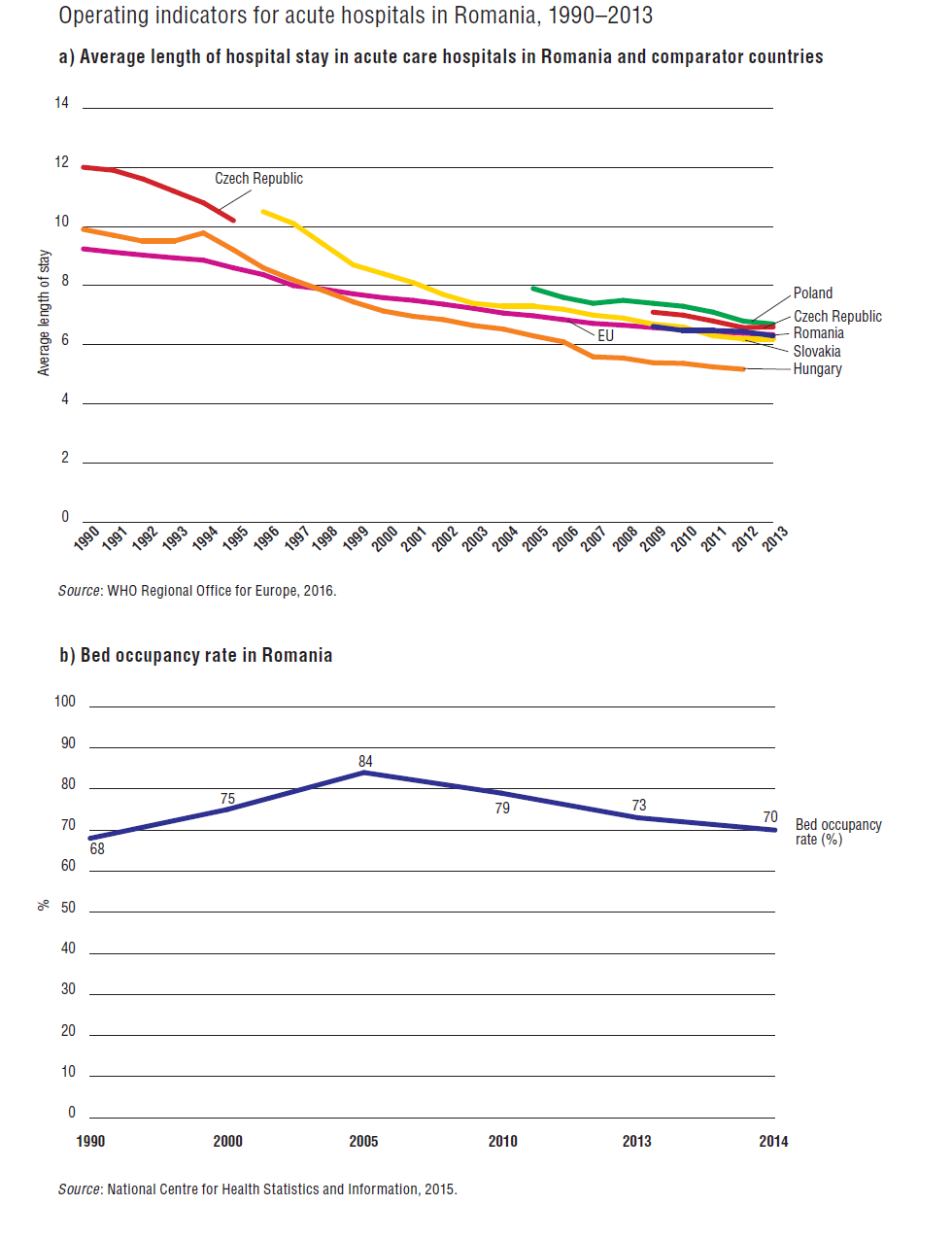
The bed occupancy rate increased from 68% in 1990 to 84% in 2005, but then fell to 70% in 2014 (Fig4.2, b). Some of the factors that are likely to have contributed to this decline were the introduction, in 2010, of ceilings in the Framework Contract on the number of ambulatory care consultations, which are often followed by a referral to a hospital at the request of patients, and the decrease in the number of doctors (see section 4.2). The bed occupancy rate in Romania in 2013 was higher than in Slovakia (67%) and Hungary (69% in 2012), but lower than the Czech Republic (74%) and the EU average of 77% in 2012 (WHO Regional Office for Europe, 2016).
Influenza vaccination coverage rate (VCR) is very low in Romania. The VCR for people of 65 years and over in the 2021–2022 season was 21.38%, substantially lower than the WHO set target of 75% and below EU average rates (43.9% for EU22 in 2020). The VCR among the general population was even lower, at 8% (decreasing from 13% in the previous season). To address and increase these low rates, a measure that the Ministry of Health recently considered was widening the group of vaccinators.
A pilot started in October 2022 that allows people to get vaccinated against seasonal influenza in authorized pharmacies. Vaccinations are administered following a general health status evaluation of the patient, who is required to complete a questionnaire before the vaccine can be safely provided. For children’s vaccination in pharmacies, a medical prescription is needed. Vaccinated patients are required to visit the family doctor for monitoring their post vaccination status.
At the time of writing (end of July 2023), there is no publicly available evaluation of this pilot; while there is no evidence available on a causal affect, for the 2022–23 season, the VCR for people of 65 years and over increased to 23%, and among the general population remained at 8%.
A comprehensive national vaccination strategy for 2023–2030 is currently under public debate.
More information (in Romanian):
Ministerul Sănătății [Ministry of Health] (2022), Ordin nr. 3.262 din 19 octombrie 2022 pentru aprobarea organizării și funcționării unui program-pilot de vaccinare a populației împotriva gripei sezoniere la nivelul farmaciilor comunitare [Ministry of Health Order no. 3262/2022 on the approval of organization and functioning of a pilot programme for vaccination against seasonal influenza in community pharmacies], Monitorul Oficial nr. 1031 din 24 octombrie 2022 [Official Gazette no. 1031 from 24 October 2022], https://legislatie.just.ro/Public/DetaliiDocument/260720
Increasing capacity to undertake investments in the health infrastructure is one of the three reforms included in the healthcare component of the Recovery and Resilience Plan for Romania, aiming to manage health infrastructure projects efficiently. To this end, a National Agency for Development of Health Infrastructure (ANDIS) was planned and developed, subordinated to the Ministry of Health with the mandate to manage major public health infrastructure projects and to provide technical expertise at the request of local authorities.
The agency was established by an emergency ordinance in June 2022 and became fully functional in December 2022, when the subsequent legislation for implementing its provisions were issued. The first major assignment of ANDIS is the construction of three regional emergency hospitals in Cluj, Craiova and Iași. These will be followed by further investments included in the Recovery and Resilience Plan for Romania, which holds provisions for the construction of and/or equipping of 25 new public health units/hospitals and the construction of four training centres for healthcare personnel skills development.
More information (in Romanian):
https://legislatie.just.ro/Public/DetaliiDocument/255924 (Ordonanță de Urgență nr. 76 din 2 iunie 2022 privind înființarea, organizarea și funcționarea Agenției Naționale pentru Dezvoltarea Infrastructurii în Sănătate [Emergency Ordinance no. 76 from 2 June 2022 on the organization and functioning of the National Agency for the Development of Health Infrastructure])
https://legislatie.just.ro/Public/DetaliiDocument/257323 (Hotărâre a Guvernului nr. 857 din 6 iulie 2022 privind organizarea și funcționarea Agenției Naționale pentru Dezvoltarea Infrastructurii în Sănătate [Government Decision no. 857 from 6 July 2022 on the organization and functioning of the National Agency for the Development of Health Infrastructure])
https://legislatie.just.ro/Public/DetaliiDocument/262976 (Hotărâre a Guvernului nr. 1.506 din 19 decembrie 2022 pentru aprobarea Normelor metodologice de aplicare a prevederilor Ordonanței de urgență a Guvernului nr. 76/2022 privind înființarea, organizarea și funcționarea Agenției Naționale pentru Dezvoltarea Infrastructurii în Sănătate [Government Decision no. 1.506 from 19 December 2022 for the approval of implementation norms of the Emergency Ordinance no. 76 from 2 June 2022 on the organization and functioning of the National Agency for the Development of Health Infrastructure])
More information (in English):
4.1.3. Medical equipment
Medical equipment is usually funded by the Ministry of Health. It can also be financed by local authorities, from donations and from externally funded projects. Since 2014, hospitals have also been allowed to purchase medical equipment from the income they receive under health service contracts with the NHIH (see also sections 2.8.6 and 4.1.1).
There are no publicly accessible national data on the types and amount of medical equipment available in health care facilities and anecdotal evidence suggests there are large variations in the distribution of medical equipment across hospitals and geographical regions, and that the availability does not reflect the level of need.
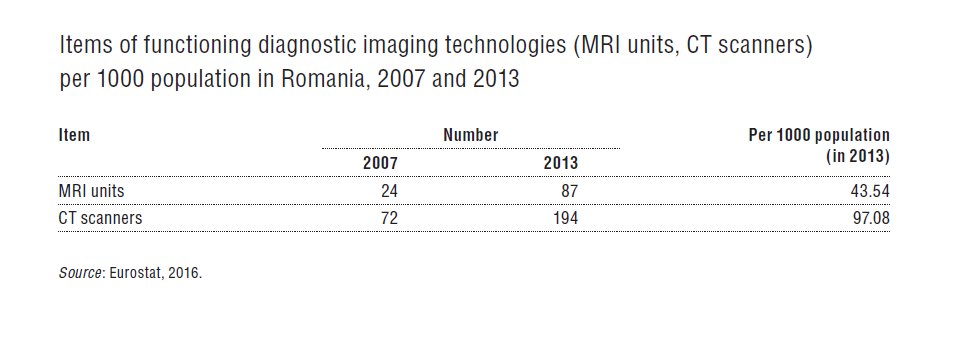
Data that are available provide insights into aggregate numbers of medical equipment only. According to Eurostat data (Table4.1), between 2007 and 2013, the number of magnetic resonance imaging (MRI) units in Romania increased from 24 to 87 and the number of computed tomography (CT) scanners from 72 to 194. In 2013, there were 43.5 MRI units per 1000 population, which was higher than in Hungary, at 30.3, but lower than in Poland (64.4), Slovakia (66.5) and the Czech Republic (74.2). Similarly, the number of CT scanners was, at 97.1, higher than in Hungary (78.8) and lower than in the Czech Republic (150.3), Slovakia (153.3) and Poland (171.7) (Eurostat, 2016). In terms of utilization, in 2012, there were 1.7 MRI scans per 1000 population, compared to an EU average of 46.5 (the average excludes Italy and Sweden) and 13 CT scans per 1000 population compared to 98 in the EU on average (the average excludes Estonia, Italy and Sweden) (OECD, 2014a). There are no data on the number of positron emission tomography (PET) scanners in Romania.
Table4.1
4.1.4. Information technology
Data from the National Institute of Statistics show that, in 2014, some 54.4% of households in Romania had Internet access. Access rates are higher in urban areas (70.9%) and vary across geographic areas, from 46.1% in the south of Romania to 76.7% in Bucharest (National Institute of Statistics, 2014a). Also in 2014, 61% of Romanians reported having ever used the Internet, a figure that is low compared to the average among EU countries, at 82% (Eurostat, 2016). The share of Internet users is lower when only daily users are considered, at 32% in Romania compared to 65% in the EU (2014 data; Eurostat, 2016). Furthermore, 27% of Romanians aged between 16 and 74 used the Internet for seeking health-related information (injury, disease, nutrition, improving health, etc.) compared to an average of 44% among EU countries.
Electronic reporting requirements were first introduced in the ambulatory care sector; since 1999, family medicine physicians and ambulatory care specialists have to report to the NHIH on the services provided to their patients in order to get reimbursed. Hospitals started to use electronic reporting with the introduction of the DRG system in 2006 (see section 3.7.1). In 2008, the NHIH implemented the SIUI (see section 2.7.1), which harmonized existing electronic reporting systems. SIUI is used by all providers for the reporting of services performed under the contract with the DHIHs. It also collects data on the insured population. In 2012, electronic prescribing was introduced for all reimbursed pharmaceuticals and is currently used across the country, and on 1 May 2015 the National Health Insurance Card was established as a tool for validating service provision. The Card contains patient identification data and may contain medical data upon a patient’s request. Patients’ health records are currently kept in paper form but an electronic health record is currently being implemented within SIUI. Electronic appointment booking systems are rarely used, typically in some private ambulatory care facilities.