-
24 April 2023 | Country Update
Two new pieces of legislation seek to improve the prevention and control of healthcare-associated infections -
09 February 2023 | Country Update
Increase of the income threshold for the eligibility for lower user charges for medicines for pensioners -
21 February 2018 | Country Update
Implementation of the European Drug Verification System in Romania -
14 May 2017 | Country Update
Modification of positive lists of drugs following HTA implementation
2.8. Regulation
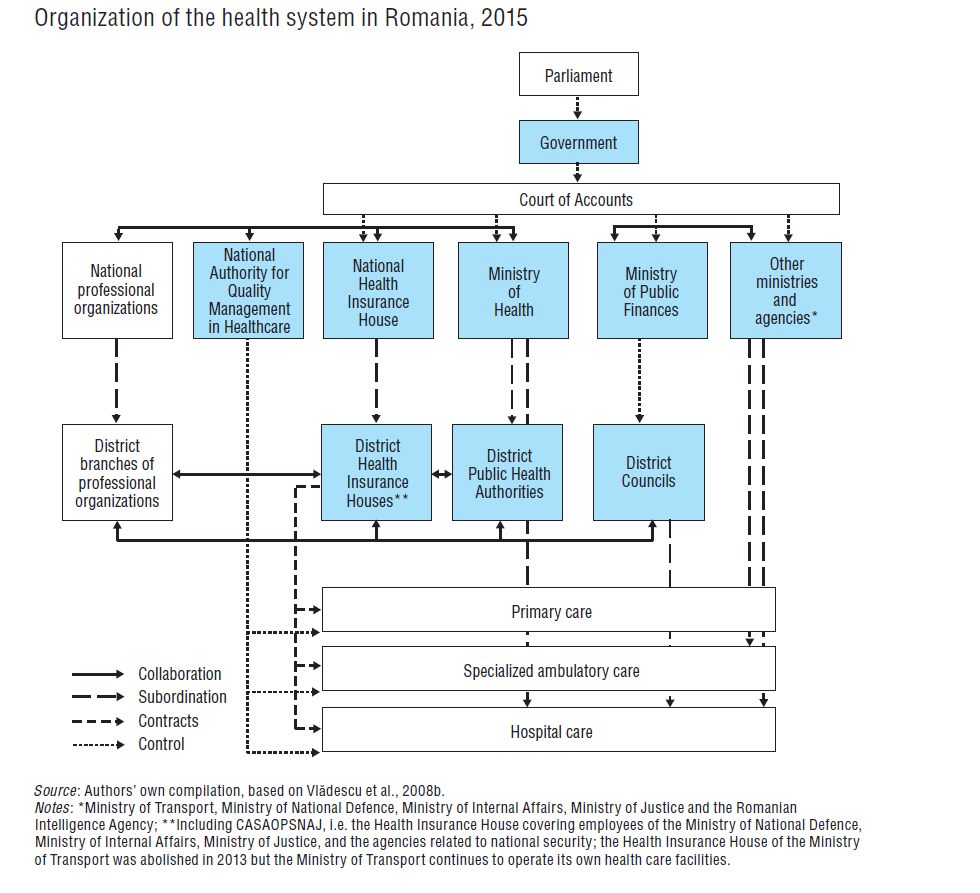
Regulatory functions are concentrated in the Ministry of Health and, since 1999, also in the NHIH (see section 2.4). Standard setting is mainly the responsibility of the Ministry of Health and the NHIH. Some regulatory responsibilities are vested in the professional organizations (see section 2.8.2). Other institutions, such as the National Agency for Quality Management in Health Care (see section 2.3) are only just beginning to assume some regulatory functions. Approval from the Ministry of Public Finances is required when a new regulation has implications for public finances and other ministries may need to approve regulations that touch upon their areas of work (see section 2.6). The ultimate oversight is held by the parliament. However, major health care legislation has often been issued by the government through emergency ordinances, bypassing the parliament (see section 6.1). Monitoring and enforcement are shared with certain other national institutions, such as the NIPH, and local organizations, such as the DHIHs and DPHAs.
Reporting of healthcare-associated infections (HAIs) in Romania has shown significant improvement over the past decade. In 2020, the estimated incidence of HAIs at the national level was 1.04% of all discharged patients in hospitals, with higher levels recorded at large university hospitals/tertiary care centres where more complex cases are treated and where reporting of HAIs is likely to be better. In 2020, 2.8 times more HAIs were reported compared to 2012. However, compared to the EU, where the average reported incidence of HAIs is around 6%, the reported incidence in Romania remains relatively low.
The main pieces of legislation supporting actions towards the prevention and control of HAIs in Romania are Law no. 3 from the 8 January 2021 on the prevention, diagnosis and treatment of healthcare-associated infections in medical facilities and residential centres for disabled adults in Romania and Government Decision no. 926 from 20 July 2022 on the establishment of the National Committee for the Prevention and Control of Healthcare-Associated Infections.
Coordinated by the Ministry of Health, the Committee includes representatives of several ministries (Ministry of Health, Ministry of National Defense, Ministry of Internal Affairs, Ministry of Justice, Ministry of Transport, and Ministry of Labour), the National Institute of Public Health, the National Administration of Penitentiaries, the Romanian Intelligence Service, the Romanian Academy, the National Union of District Councils, and associations representing other administrative levels (municipalities, towns and communes).
After seven months since its establishment, the Ministry of Health approved regulations for its organization and functioning, and the Committee became fully functional. The Committee is primarily responsible for developing the national strategy for the prevention and control of HAIs, defining the authorization criteria related to HAI prevention for health-care facilities, developing management performance indicators related to HAI prevention, and creating guidelines, protocols, and surveillance systems for HAIs.
More information (in Romanian)
https://legislatie.just.ro/Public/DetaliiDocument/265514In Romania, some ambulatory drugs are only partially covered by the statutory health insurance, with users having to pay a percentage of the price, depending on the drug category: 10% for generics, 50% for expensive generics and branded medicines, or 80% for medicines with a low health technology score.
Since 2009, pensioners with low incomes of up to 600 Ron (approximately 150 Euro) per month have paid only 10% of the price of expensive generics and branded medicines, with the remainder covered on their behalf by the Ministry of Health from the state budget. This “low income” threshold has been periodically updated, reaching 900 Ron (200 Euro) in 2017, 1299 Ron (270 Euro) in 2020, and 1429 Ron (286 Euro) in 2021. The new threshold approved by the Government for 2023 was increased to 1608 Ron (321 Euro).
More information (in Romanian):
https://legislatie.just.ro/Public/DetaliiDocumentAfis/263269
According to the EU legislation, the European Drug Verification System (EDVS) should be fully operational across the EU from 9 February 2019. In February 2018, implementation of EDVS was officially launched in Romania.
To this end, the Organization of Serialization of Medicines in Romania (OSMR) was established. It is an NGO with the specific task of implementing Directive 2011/62/EU on preventing entry of falsified medicinal products into the legal supply chain. It will provide a verification platform for Romania, connected to a European hub, through which pharmacies and other stakeholders will be able to verify the authenticity of medicinal products. Producers of medicines will be obliged to place a unique identifier and an anti-tampering device on each pack of medicine to allow their identification and authentication.
The implementation of this Directive will be financially supported by the pharmaceutical industry.
More information (in Romanian):
Authors
The introduction of HTA as the basis for the inclusion of drugs on the reimbursement lists has already led to several revisions of those lists. Further, besides the existing five positive lists for pharmaceuticals with different degrees of reimbursement (90% (list A), 50% (list B), and 100% (lists C1, C2, and C3)), a new level of reimbursement was introduced by the end of 2015 (20% (list D)). List D includes those medicines that obtained low scores following the HTA process, and consequently were moved from the other lists to a lower level of reimbursement (20%).
Authors
2.8.1. Regulation and governance of third-party payers
The Framework Contract, introduced for the first time in 1999, is the main legislative tool that regulates the purchasing of health services. It is developed by the NHIH, in consultation with the representatives of service providers, patients and civil society. It is approved by the Ministry of Health and passed as a Government Decision. The Ministry of Public Finances influences the purchasing of medical goods and services by defining expenditure ceilings for the key cost categories, such as human resources, pharmaceuticals, and so on.
The Framework Contract contains a definition of the statutory benefits package and information on the terms under which patients can obtain services, provider payment mechanisms, the relationship between providers and the DHIHs, terms of contracts (e.g. quality criteria for providers), providers’ rights and obligations, and transposition of EU regulations with relevance to health care provision. Benefits are described in the Framework Contract for each area of care with a different level of detail, depending on the type of service. The benefits, especially those services that are paid by tariffs or procedures in the diagnosis-related group (DRG) system, are further detailed in a document titled “The application norms of the Framework Contract”, which is a Common Order signed by the president of the NHIH and the Minister of Health. The Framework Contract and its norms are issued periodically (yearly until 2013, and every two years since then) and form the basis for concluding individual contracts between the DHIHs and health service providers (see section 3.3.4) and for reimbursement of cross-border health care services (see section 2.9.6).
The contracts must take into account the following criteria: the number of residents registered with the family medicine physicians, number of hospital beds, ALOS, number of consultations, and so on. These criteria are linked to the health needs of the local populations, but also to the existing infrastructure and health personnel. The DHIHs monitor the fulfilment of the contracts. All DHIH activity is monitored and controlled by the NHIH according to a control and monitoring plan.
Romanian health care legislation (Law 95/2006) allows for private third-party payers in the market. The voluntary health insurance (VHI) market is regulated by the Ministry of Health and the Insurance Supervisory Commission (Olsavszky, 2016) but this market is virtually nonexistent (see section 3.5).
2.8.2. Regulation and governance of providers
Organization
The key legal act regulating the organization and functioning of health care providers is the Law 95/2006 (see section 2.1). The Ministry of Health develops the secondary legislation on the technical norms required for issuing the authorizations for the establishment and functioning of health care providers, and, together with the NHIH, secondary legislation on service provision, including quality norms.
Primary health care physicians are independent practitioners. Physicians are accredited by the College of Physicians. Each professional association plays a role in setting regulations for their respective professions. Most of the secondary and tertiary health care facilities are publicly owned and are under state administration (see Chapter 5). Private providers are allowed to enter into contracts with the DHIHs. Individual providers who wish to be contracted must fulfil conditions on professional competence and technical equipment. An important condition for entering into contracts with the DHIHs for hospitals is having an accreditation from the National Commission for Hospitals Accreditation, which started its operations in 2009. Accreditation is granted for five years. This Commission was recently integrated into the National Authority for Quality Management in Health Care (see Fig2.1). In the future, the accreditation process will be extended to other health care providers besides hospitals (at the time of writing, the Authority is still in the process of being established; see section 2.3).
Fig 2.1
Quality
Except for care provided in hospitals, quality is not regulated by a specific act. Law 95/2006 (art. 238–239) includes some references to the quality of care for different types of services, and secondary legislation in this area is still being developed. It also stipulates that the Ministry of Health and the NHIH are responsible for establishing quality criteria for care provided to insured persons. All health care providers who have signed contracts with the DHIHs must adhere to these criteria. These criteria include, for example, the average time per consultation, share of referrals to specialist care in the total number of consultations (for primary care) and percentage of patients referred to other hospitals (for inpatient care), percentage of operations performed in surgical wards, the rate of nosocomial infections for hospitals and ISO-certification for laboratories.
Compliance is monitored at both the NHIH and DHIH levels. Monitoring mainly focuses on financial aspects and the volume of services rather than on quality. The units responsible for monitoring are not adequately staffed. Some criteria are only checked ‘on paper’ when contracts are signed. Audits are rare because of the lack of capacity.
The Ministry of Health has made several attempts to improve the quality of care and its monitoring, especially at the hospital level. These included Order 4017 on the establishment of quality control structures in hospitals (quality cores) in 2001 and Order 975 on the establishment of a quality management structure in hospitals, which also in 2012 included the obligation for hospitals to train staff in quality assurance. Neither has been sufficiently enforced however, mainly because the hospitals do not have the necessary resources for their implementation.
Romania is a member of the European Union Network for Patient Safety and Quality of Care (PaSQ), a project funded by the EC. The project aims to organize platforms for promoting patient safety and quality in health care in all EU countries, by exchanging information and experiences on best practices. In the future, it is envisaged that the newly established National Authority for Quality Management in Health Care (see section 2.3) will take over responsibility for the regulation and monitoring of quality of care.
Provisions regarding negligence by officials of a public service (such as health care provision), including medical negligence, are incorporated in the New Criminal Code of 2014. According to the regulations, negligence is punishable with a fine or imprisonment from between three months to three years (see section 2.9.4). The Criminal Code applies to health care professionals in both public and private sectors.
2.8.3. Registration and planning of human resources
Health professionals are registered with the relevant professional organization (see section 2.3), to which they apply to be accredited or reaccredited. In order to be reaccredited, health professionals must comply with continuing medical education (CME) requirements (see section 4.2.3). Any citizen of an EU Member State, an EEA country or Switzerland, who has graduated from a medical university in their country of origin, is entitled to practise in Romania. Any citizen of a third country having permanent resident status in Romania and a diploma recognized by Romania or any EU Member State, or having documents issued by any EU Member State that prove professional experience of at least three years in the medical field, is also entitled to practise.
The Ministry of Health controls, both directly and indirectly, the number of health professionals in the system. Direct control is exerted by approving the number of posts and types of medical specialties within the publicly owned health care units. Indirect control is exerted by issuing regulations in cooperation with the professional associations in order to ensure better geographical distribution of human resources. For example, special commissions at the DHIHs determine the number of ambulatory care specialists (and thus the number of contracts) that is needed at the district level, based on the number of residents, workload and available funds.
The planning of human resources is mainly based on the number of workplaces within the public system, which is relatively constant. If a numerus clausus is in place at medical universities, on which each university may decide autonomously, it mainly reflects the teaching capacity and not the health care needs of the population. The number of residency places for doctors is determined by the Ministry of Health based on the historical number of doctors in each specialty. Every year, the DPHAs report their estimated needs for a five-year period (five years is the average duration of residency training) based on how many new trainees enter and exit each specialty. Decisions to increase the number of trainees are taken on an ad hoc basis.
Recent changes in the regulation of human resources have mainly been driven by the harmonization of national legislation with the EU regulation on the mutual recognition of professional qualifications (EU Directive 2005/36/EC). They have mainly targeted training and retraining of health care professionals as well as upgrading of educational and training facilities. They were not intended to change the mix of skills in the health care sector.
2.8.4. Regulation and governance of pharmaceuticals
Regulation of pharmaceutical products
Pharmaceuticals are extensively regulated by the Law 95/2006. The Law provides a definition of pharmaceutical products for human use that are intended to be placed on the market in Romania, and includes provisions related to their marketing, manufacture and importation, labelling, wholesale distribution, advertising and pharmacovigilance. The NAMMD, which was set up in 2010 through a merger of the National Medicines Agency with the Technical Office for Medical Devices, is responsible for market authorization and surveillance of the safety of medicinal products on the market. It is subordinated to the Ministry of Health.
No medicinal product may be placed on the market unless a marketing authorization has been issued by the NAMMD. Every year, the Agency issues an index of medicinal products authorized for marketing in Romania, specifying for each whether or not it is subject to prescribing. The Ministry of Health may temporarily authorize the distribution of an unauthorized medicinal product in situations of public health concern or other emergency situations. Medicinal products are divided into those that are subject to medical prescription and those that are not. The first category includes pharmaceuticals that: are likely to be dangerous if used without medical supervision; contain substances that can cause adverse reactions requiring further investigation; or are injectable.
Pharmacovigilance
The NAMMD operates the pharmacovigilance system and the Ministry of Health, through the NAMMD, undertakes appropriate measures, such as issuing warnings and temporary withdrawals, to encourage doctors and other health care professionals to report suspected adverse reactions. The pharmacovigilance system is in line with Directive 2001/83/EC on the European Commission Community code relating to medicinal products for human use.
Patent protection
Patent protection is governed by the Patent Protection Law of 1996 and its subsequent amendments, and any patent has to be registered by the Romanian State Office for Inventions and Trademarks (OSIM). A generic drug may not be marketed in Romania before the passage of 10 years since the authorization of the original drug. An application for market authorization does not need to provide the NAMMD with the results of preclinical and clinical trials if it can prove that the medicine is a generic for a drug that has been authorized for at least eight years in Romania or in another EU Member State.
Advertising
Advertising is prohibited for products that do not have a valid marketing authorization. It is also not permitted for prescription-only drugs or drugs that contain psychotropic or narcotic substances. Advertising of pharmaceuticals should encourage the rational use of drugs and must not be misleading.
Regulation of pharmacies and wholesalers
Disbursement of drugs takes place through community pharmacies (pharmaceuticals can be pre-ordered on the phone, or via the Internet in some pharmacies, but must be collected in the pharmacy within 24–48 hours). Prescribing has been done electronically since 2012 and paper prescribing can only be used under special conditions. A pharmacy can only be established by a legal person (company) and not a natural person, and it has to employ at least one pharmacist. Decisions on whether a new pharmacy can be established depend on the ratio of existing pharmacies and the number of residents. In urban areas, the total number of pharmacies cannot exceed one pharmacy per 4000 inhabitants; in district capital cities, the ratio cannot be higher than one per 3500; and in Bucharest one per 3000. There are debates about eliminating these limits based on free market arguments. The Ministry of Health is responsible for the registration and licensing of pharmacies. Inspection and control of pharmacies are performed by the Ministry of Health and the NAMMD.
Generic prescribing was officially introduced when indicative maximum budgets for prescribing doctors were introduced in 2005 and is now customarily used with electronic prescribing. It was temporarily abolished in 2007 for political reasons and then reintroduced in 2010. If a doctor prescribes by generic name (International Nonproprietary Name, INN), pharmacists must dispense the cheapest drug and must inform the patient of the available generic substitute.
In 2006, the system of indicative maximum budgets was replaced by yearly budget ceilings for pharmacies set by the NHIH (see Vlădescu et al., 2008b), but the latter was abandoned in 2008. The ceilings were highly unpopular among patients with chronic conditions as many pharmacies reached their ceilings before the end of the month and patients were then forced to look for pharmacies that had not reached their ceilings. When in the absence of any ceilings the cost of pharmaceuticals kept increasing, in 2009 the Ministry of Health introduced a type of claw-back system (implemented in 2011), mainly at the level of marketing authorization holders (MAHs) of the drugs on the reimbursement list (i.e. manufacturers or distributors). Every quarter, each producer has to return to the state budget a percentage of the profits (the claw-back point) according to a formula that depends on the difference between the sales value in that quarter and the reference sales value set annually by the government. The claw-back system has been heavily criticized because it does not take into account the differences in sales between the manufacturers. Producers of generics are worst off under this system. In 2014, the Ministry of Health proposed to amend the claw-back system so that new drugs being approved for reimbursement would be subject to cost–volume and cost–volume–outcome agreements (IHS, 2014). Cost–volume outcomes were implemented in 2015.
Wholesale distribution and storage of medicinal products are allowed only for medicinal products that have a marketing authorization granted by the NAMMD or through the EU centralized procedure. Pharmacies are not allowed to conduct wholesale of drugs.
Counterfeit drugs
The NAMMD provides information on counterfeit drugs in Romania on its website (www.crimemedicine.ro). The purpose of this site is to inform the public about counterfeit drugs (e.g. through warnings), their possible effects on health, legislation and how to report counterfeit drugs. The scale of this problem in Romania is not known.
Policies to improve the cost-effective use of pharmaceuticals
Apart from generic prescribing, there are currently no specific measures in place aimed at improving the cost–effectiveness of prescribing. However, electronic prescribing, in place since 2012, may help improve monitoring of the use of pharmaceuticals and contribute to better prescribing practices. The effects of electronic prescribing are yet to be analysed. There is also no coherent policy aimed at influencing patients to improve the cost-effective use of pharmaceuticals.
Pricing of prescription pharmaceuticals
After a new drug obtains market authorization from the NAMMD, the MAH applies to the Ministry of Health for a price. A price increase or decrease for an already registered drug can also be requested, although permissions for a price increase are seldom granted. Prices of over-the-counter (OTC) medicines are not regulated, but the MAH has to notify the Ministry of Health of the price within 30 days after putting the drug on the market. The distributor has to submit the manufacturer’s price to the Ministry of Health. Based on this information, the price is usually compared with the prices of the same product in the following reference countries: the Czech Republic, Bulgaria, Hungary, Poland, Slovakia, Austria, Belgium, Italy, Lithuania, Spain, Greece and Germany. The price in Romania can only be lower than or equal to the lowest price among the reference prices. No other comparison tools are used. If the drug is not registered in any of the reference countries, then the price in the country of origin is used as reference. The price of a new generic cannot exceed 65% of the reference price of the original drug. The formula to calculate the maximum retail (pharmacy) price takes into account the manufacturer’s price (ex-factory price), wholesale price and VAT (9% in Romania). The mark-ups of the wholesaler and the pharmacist depend on the price of the package and discounts; importers may give discounts to wholesalers and wholesalers may give discounts to pharmacies. The total mark-up of the wholesalers and pharmacies varies from 10% for prices up to 300 lei (around €67) and 24% for prices below 25 lei (around €6). For drugs priced at over 300 lei, the mark-up becomes a flat rate of 30 lei (around €7) for the wholesaler and 35 lei (around €8) for the retailer. Once a year, prices can be adjusted for exchange rate fluctuations. Retail prices are published in a Drug Catalogue that is updated quarterly.
Public reimbursement of pharmaceuticals
Drugs that are reimbursed by health insurance are included in the positive lists elaborated by the HTA department of the NAMMD (see section 2.7.2) in cooperation with a special commission at the Ministry of Health. As described above (section 2.7.2), inclusion (or exclusion) depends on a number of parameters, including: therapeutic benefit, reimbursement status (e.g. whether it is reimbursed in another EU Member State), treatment cycle (if several treatment rounds are needed as opposed to one), patient accessibility, treatment cost and in relation to GDP per capita (compared to treatment costs in other countries). Pharmaceutical companies have to apply for their products to be evaluated and included on the positive lists. Evaluation can also be initiated by the NAMMD when there are safety concerns about a particular drug, when the drug’s prescription status has been changed or a new indication is in place, or if there are concerns about the drug’s budgetary impact. Since 2015, the lists have to be updated every year.
There are five positive lists (Table2.1). List A contains mainly generics, and list B includes expensive generics and branded names. Lists A and B are for outpatients, with drugs listed as generic compounds in alphabetical order. A reference price system is applied to all drugs on the lists. The reference prices are based on the lowest-priced product within a cluster of medicines, based on the generic substance, the pharmaceutical form and strength. In addition, patients must pay 10% or 50% of the reference price (i.e. of the lowest-priced product of the cluster). If a patient prefers a more expensive product, they will also have to pay the difference between the price of the lowest-priced product and the preferred drug (see section 3.3.1).
Table2.1

2.8.5. Regulation of medical devices and aids
Since 2014, the NAMMD has had regulatory authority over the market of medical devices in Romania, taking over from the Ministry of Health. The Agency performs the evaluation (including audits) of manufacturers and other distributors of medical devices that are regulated by the European directives (93/42/EEC, 98/79/EC, 90/365/EEC). The purpose of the evaluations is to confirm that they meet all the necessary conditions, such as technical equipment, qualifications of staff, safety and quality certificates. All medical devices used in the health sector must have authorization certificates issued by the NAMMD. Certification can be requested by the users (purchasers), producers or distributors.
The procurement of medical devices is done at the level of health care facilities in both private and public sectors. Procurement by public sector health facilities must meet administrative regulations on public procurement. Quality of the procured devices is monitored periodically (every two to three years, depending on the device) in both sectors by the NAMMD. The Ministry of Health can procure medical devices centrally, as part of capital investment in the publicly owned health facilities (see section 2.8.6).
2.8.6. Regulation of capital investment
Financing of capital investments in health care facilities and equipment is mainly from the state budget, through the Ministry of Health, but can also come from local budgets (according to investment plans pre-approved by the Ministry of Health) and external funds (World Bank, EU structural funds). Medical units can also cover capital investments from their own revenues and donations. Until 2014, funds received by hospitals from the NHIH for the contracted services could not be used for capital investments. A change of legislation (of Law 95/2006) in February 2014 allowed hospitals to pay for investments in infrastructure and medical equipment from the income received from the contracts, but only after all operating expenditure (e.g. salaries, drugs) has been covered.
The Ministry of Health develops yearly capital investment programmes that are included as an annex to the state budget. The methodology for the development of these programmes and the allocation of funds for capital investments to public health care institutions is approved by a ministerial order. The Ministry of Health elaborates the investment programmes in accordance with the health care investment policy. The current policy was included in the Budgetary Strategy for 2014–2016 and has as objectives: modernization of infrastructure and equipment of medical institutions (see section 4.1), including emergency services; rehabilitation of neonatology and obstetric wards; repairs of hospital buildings; and development of cardiovascular surgery centres for children and newborns.
There are no systems in place aimed at ensuring an equitable distribution of capital across the country and across various levels of care.