-
01 January 2025 | Country Update
Planned new organizational model for primary care not implemented -
26 January 2024 | Country Update
Changes in coordinated care within primary health care -
10 October 2021 | Policy Analysis
Piloting of a new model of primary health care provision (2018–2021)
5.3. Primary / ambulatory care
The obligation to establish teams in primary health care planned for introduction on 1 January 2025 was not introduced, and all existing patient declarations remained valid. The creation of integrated care teams – consisting of a family doctor, a nurse, and a midwife – therefore remained a voluntary option.
Another change concerned physicians specializing in paediatrics, internal medicine, and general medicine. Under the previous regulations, in order to continue working in primary health care, they were required to complete a course in family medicine by the end of 2024. However, this deadline was postponed for two years.
Authors
From 1 November 2023, primary care services will be able to provide more comprehensive, coordinated care to a wider range of patients. In particular, people with pre-diabetes, who were previously excluded, will now benefit alongside those with diabetes. Similarly, patients with hyperthyroidism will be included in addition to those with hypothyroidism.
The scope of coordinated care will also be expanded to include the diagnosis and treatment of chronic kidney disease. In addition, patients under the age of 18 using coordinated care services will now have access to specialist consultations.
In addition, primary care physicians will be empowered to order tests that were previously the domain of specialists, in particular for allergies (both inhalants, for example, tree pollen, dust and foods, for example, milk, wheat), thereby speeding up diagnosis and improving the effectiveness of treatment.
Conversely, healthcare providers providing night and holiday services will be authorized to refer for laboratory testing.
References
Primary health care (PHC) in Poland has traditionally suffered from several key weaknesses, including the insufficient provision of preventive services, limited budgets for diagnostics, and workforce shortages, including family medicine specialists and nurses. The PHC PLUS pilot, in place between 2018 and 2021, offered an opportunity to strengthen provision of preventive services within PHC, improve coordination of care for the patients and retain more patients at the PHC level by increasing diagnostic competencies of PHC doctors and their links with specialist doctors.
The model put much more emphasis on disease prevention and health promotion within PHC, with Individual Health Plans offered to qualifying patients. These were to be largely led by the nurses, focusing on educating patients about behavioural risk factors. The model also aimed to shift management of common chronic conditions to multidisciplinary PHC teams, with enhanced competencies of PHC doctors to order diagnostic tests and consult with specialists, instead of referring them to specialist consultations. Disease management programmes (DMPs) for 11 most prevalent non-communicable chronic conditions and Individual Medical Care Plans tailored to patients’ individual condition(s) were offered within the pilot. As such, the model had the potential to strengthen the role of PHC and reduce hospital referrals.
Only about 40 PHC practices met the criteria to be included in the pilot, with small PHC practices (which dominate PHC provision in Poland) severely underrepresented in the pilot. Workforce shortages, especially in the rural areas, were another major obstacle to the pilot’s implementation. The pilot ended in September 2021 and so far, there are no plans to roll it out nationally, mainly due to the high cost of the pilot. At the end of 2021, introduction of care coordinators was mandated in all PHC practices – the only solution tested in the PHC PLUS pilot that has been implemented to date (see Country updates section).
References
Badora-Musiał K, Sagan A, Domagała A, Kowalska-Bobko I. Testing the 2017 PHC reform through pilots: Strengthening prevention and chronic care coordination. Health Policy. 2021 Feb;125(2):185–190. https://doi.org/10.1016/j.healthpol.2020.10.014. Epub 2020 Nov 5. PMID: 33298319.
5.3.1. Scope
PHC constitutes the main entry point to the Polish health care system. PHC providers serve as “gatekeepers” and the patient must obtain a referral before accessing more specialist care, although exceptions are made for certain types of specialists and certain population groups (see section 5.2).
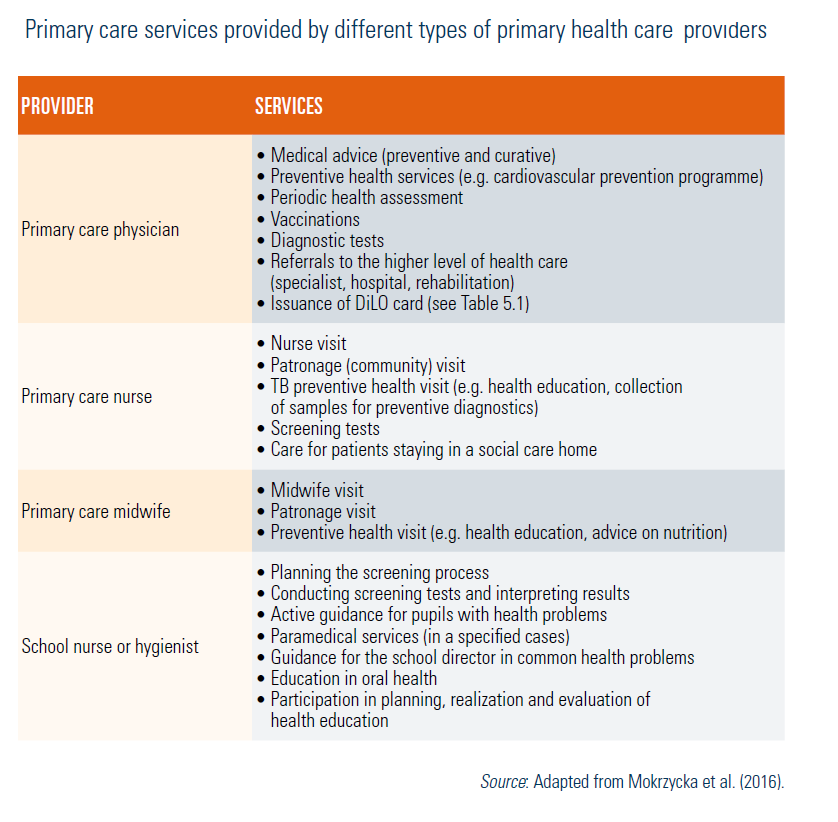
Statutory PHC services are provided by PHC physicians, nurses and midwives, school nurses and hygienists (see Table5.3). The scope of services covers diagnostics, treatment, rehabilitation, and nursing services in the scope of general medicine, family medicine and paediatrics; as well as health promotion and disease prevention. The latter are specified in the 2005 Executive Regulation of the Minister of Health on the Scope of Tasks of Primary Care Physician, Nurse and Midwife Working in PHC and include: indication and diagnosis of health risk, health education, advice on healthy lifestyles, education in hygienic nursing of neonates and education in prevention of gynaecological diseases. National preventive programmes are also implemented within PHC, including prevention of cardiovascular diseases, prophylaxis of tuberculosis, prevention of cervical cancer and prevention of tobacco-related diseases (including COPD) (see section 5.1). In addition, guaranteed PHC services include night time and holiday care and sanitary transport.
Table5.3
The Act on Primary Health Care that came into force in 2017 introduced important changes in the organization of PHC. It introduced PHC teams consisting of a PHC physician, a nurse, a school nurse and a midwife and, optionally, a physical therapist. The PHC physician will coordinate the care over the patient provided by the PHC team as well as provide necessary referrals to specialist care and diagnostics and collaborate with specialists during the patient’s hospital stay. Patients with selected chronic diseases will be able to choose between integrated care specific to their condition and coordinated by the PHC physician and specialist care provided by a specialist physician. Coordinated PHC is currently being piloted (see section 6.2). The objectives of the reform are to provide comprehensive and high quality PHC that is centred on the patient and well coordinated, which includes coordination between the PHC physician, nurse and midwife and coordination between the various levels of care; and increase the role of prevention and health education. Chronically ill patients who wish to receive coordinated PHC must declare this in writing. Choice of coordinated PHC means that the patient will no longer be able to see specialist of his/her choice – the choice of specialist will be determined by the PHC physician coordinating care.
5.3.2. Organization of provision
In 2017, approximately 33 500 PHC physicians (98 per 100 000 population), approximately 21 400 nurses (60 per 100 000 population) and 6 200 midwives (38 per 100 000 female population) provided health care services financed by the NFZ (NFZ, 2018d). The vast majority of PHC physicians, nurses and midwives (over 90%) work in therapeutic entities as defined in the 2011 Act on Therapeutic Activity (see section 2.4.2). In practice, more than one PHC physician and nurse work together in one clinic (and in many cases also a midwife) to provide easy access to PHC services. Patients have a free choice of PHC physician, nurse and midwife and switching is generally possible up to twice a year (see section 5.2).
Physicians with a specialization in family medicine (or physicians undergoing such specialization) and physicians with level II specialization in general medicine can work as PHC physicians. In addition, due to the shortage of family medicine specialists, until the end of 2024 physicians with grade I specialization in general medicine or internal medicine and paediatricians may work as PHC physicians (paediatricians can only look after patients up to 18 years old) (Badora-Musiał & Kowalska-Bobko, 2017; Mokrzycka et al., 2016).
According to NFZ regulations, the maximum number of patients registered with one PHC physician cannot exceed 2500. The maximum number of patients registered with one nurse is also 2500 and up to 6600 patients can be registered with one midwife. The average actual numbers of registered patients are 1020 for PHC physicians (more than 96% of the population is registered), 1532 for nurses (92% of the population is registered), and 2573 for midwives (80% of the female population is registered) (NFZ, 2018d).
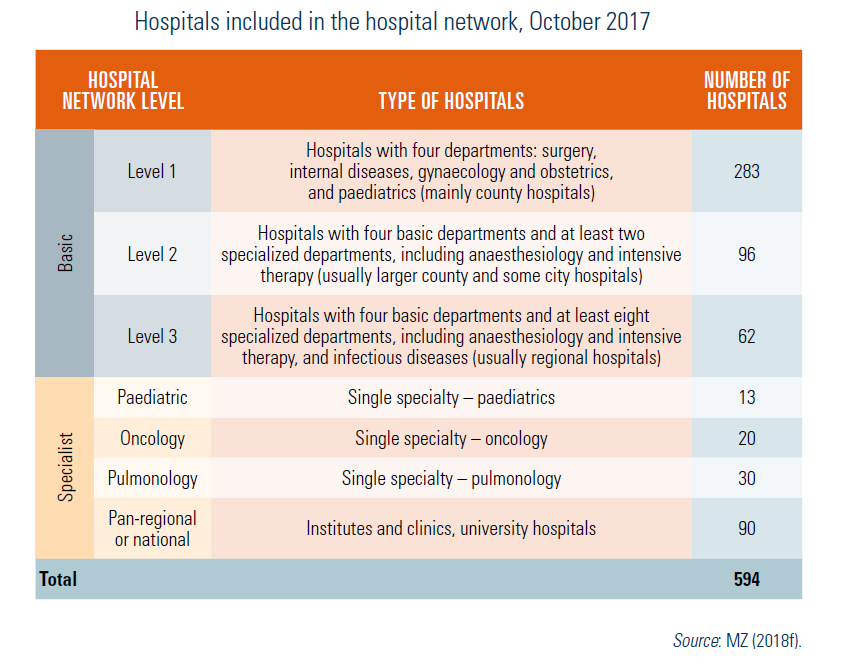
PHC physicians must be available to their patients 10 hours per day (from 8am until 6pm) from Monday to Friday, excluding official holidays. PHC services are also available after 6pm on work-days, as well as on Saturdays, Sundays and during official holidays in entities that have signed contracts with the NFZ for provision of “night and holiday health care”. The on-call physician can provide medical advice at the clinic, by telephone or at patient’s home (if the patient’s condition is serious). No referral is needed to access night and holiday health care and patients can seek care at any entity that signed contract with the NFZ, irrespective of whether they are registered on the patients list or not. Since 1 October 2017, hospitals that are included in the hospital network (level 1–3 and paediatric hospitals; see Table4.3) have been obliged to provide “night and holiday care”. The “night and holiday” services function concurrently with the SORs. Patients who report to a hospital without a referral are admitted and sent to either the SOR or to the “night and holiday health care” unit.
Table4.3
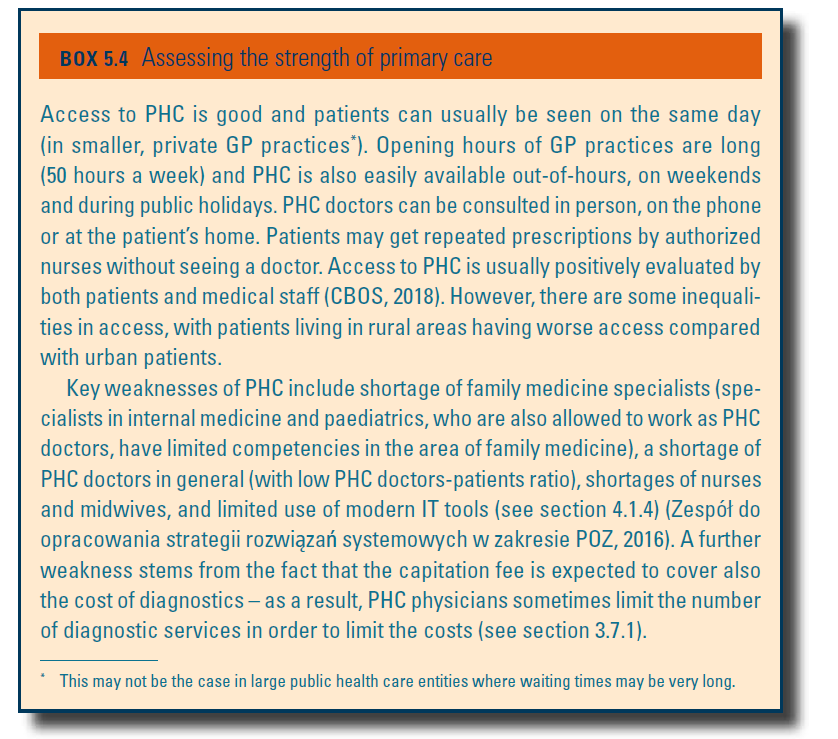
Box5.4 provides an assessment of the strength of primary care.
Box5.4