-
23 January 2026 | Country Update
Adoption of the updated regulatory framework for general practitioners -
04 May 2021 | Policy Analysis
Creation of a single portal for health data
4.1. Physical resources
In spring 2020 the Norwegian Government suggested to amend the
existing Health Registry Act and other relevant data regulations to
establish a single portal for all secondary use of health data with a
common system of governance. The reform builds on the work undertaken
under the National Health Data Programme, which was established in 2017
by the Directorate for e-Health (NDE), and the Health Registries for
Research project (2014-2019), which was aimed at improving access to
existing health data for health care improvement, monitoring, management
and research purposes (see section 2.6 in the online HiT). The reform
was further enabled by the recent (2019) changes in the Statistics Act
that allowed for a limited set of demographic and socioeconomic
variables to be linked to health data from the registries for the
purpose of health care improvement, monitoring and management and not
only for research purposes as before.
The suggested amendments
were approved by the parliament in December 2020 and enacted from
January 2021. As part of the reform, the Prescription Database (NorPD)
will be transformed from a pseudo-based registry into a registry with
unique patient identification (regulations detailing this were passed in
the Parliament in April 2021). A new organisational unit, the National
Data Service, will be established in 2021 within the NDE. The new unit
will be responsible for granting access to health data that is available
through the portal helsedata.no. The portal was established in autumn
2020 and contains information about various data sources, variables,
electronic application forms and guidance on the process of requesting
access to health data. The National Data Service will be co-located with
the National Health Archives at Tynset - a rural location in the
Eastern part of Norway.
The detailed regulation for National
Data Service will be subject to a public hearing in spring 2021. The
unit is expected to be operational - with delegated authority to
authorize access to health data - from September 2021, when production
of datasets may start. A dashboard of process and outcomes indicators
have been established to monitor the implementation of the reform. The
rural location of the unit is posing some challenges with regards to
transfer of personnel from current urban settings.
The reform supports the ‘Health, Demography and Quality of Life’ programme of the Nordic councils of Ministers, whose action areas include finding solutions on how to bridge Nordic health data and personal data for utilization in the Nordic health ecosystems. Finland and Denmark have both recently established national health data portals in support of this programme.
Authors
4.1.1. Capital stock and investments
Current capital stock
In 2019 the four RHAs oversaw a total of 20 hospital trusts. The number of hospital trusts reflects population size, with the greatest number of trusts located in the South-Eastern RHA (see Table4.2). The size of hospital trusts varies, from about 160 beds in the smallest (Sunnaas) trust to more than 1600 beds in the largest (Oslo University Hospital) trust (both in the South-Eastern RHA). Four trusts have more than 1000 beds, eight have between 500 and 1000 beds, and eight have fewer than 500 beds. The hospital trusts, in turn, comprise smaller hospitals and other institutional entities at different locations. A single trust can cover vast geographical areas. For example, in the county of Nordland, the distance between hospitals within a trust can exceed 500 kilometres.
Table4.2

Each region has one regional hospital, which is a university hospital offering the largest range of services in the region. The regional hospital may have interregional responsibilities in some areas, i.e. provide certain services to patients from all regions, or head networks within specialties at regional and/or national level. A new national hospital plan, released in November 2019, organizes hospitals into a three-tier network (see section 5.4.2).
In 2017 beds in publicly financed providers accounted for 96% of the total number of hospital beds (Statistics Norway, 2019a).
The age and condition of hospitals vary across the country (RIF, 2015). According to the survey conducted by the Auditor General in 2011 (latest information available; Auditor General, 2011), the average age of hospital buildings was approximately 45 years in that year but there were large variations in the condition of the facilities, with half of them being in good or acceptable condition, 40% in unsatisfactory condition in need of corrective measures and 10% in poor condition and in need of major technical upgrading. In general, the condition of hospital facilities was poorer in the Northern and Western RHAs.
Regulation of capital investment
Overall responsibility for the planning of infrastructure and capital investments in public facilities lies with their respective owners. The municipalities decide on investments in primary care and other care provided at the municipal level, with investment decisions in each municipality taken by the local municipal council (see sections 5.1–5.3 and 5.6–5.11). Decisions on investments in hospitals are taken by the RHAs, which represent directors of the local hospital trusts. Investment proposals are made by the boards of local hospital trusts, which later also approve the investment decisions of the RHAs. The exception is the South-Eastern region, where the RHA is responsible for all larger investments. While the RHAs have a wide authority to plan and manage their hospital infrastructure, the MOHCS is responsible for monitoring investments in specialist care. In addition, the MOHCS has the authority to approve larger capital investment projects for which 30% or more of funding comes from the RHAs.
In 2015 the RHAs established the Agency for Hospital Construction (Sykehusbygg HF). The Agency is funded by the RHAs with additional funding allocated by the government (Norwegian Ministry of Finance, 2017). It provides expertise on hospital planning and construction to all hospital trusts and can assist them in the acquisition and sale of real estate.
Investment funding
Hospital trusts finance capital investments and annual depreciation costs from their general incomes, i.e. from allocations from the RHAs. In case of large capital investments, they may apply (via their RHA and with the support of the Agency for Hospital Construction) for a special investment loan from the MOHCS for 70% of the funding. If hospital trusts enter into contracts with private service providers, the contracts must take into account the capital investment needs of these providers.
The RHAs may finance investments in the health trusts by borrowing (debt financing). RHAs are not allowed to borrow money in the private market, but can borrow from the Norwegian Central Bank. Private financing occurs occasionally in the form of donations, e.g. equipment donations.
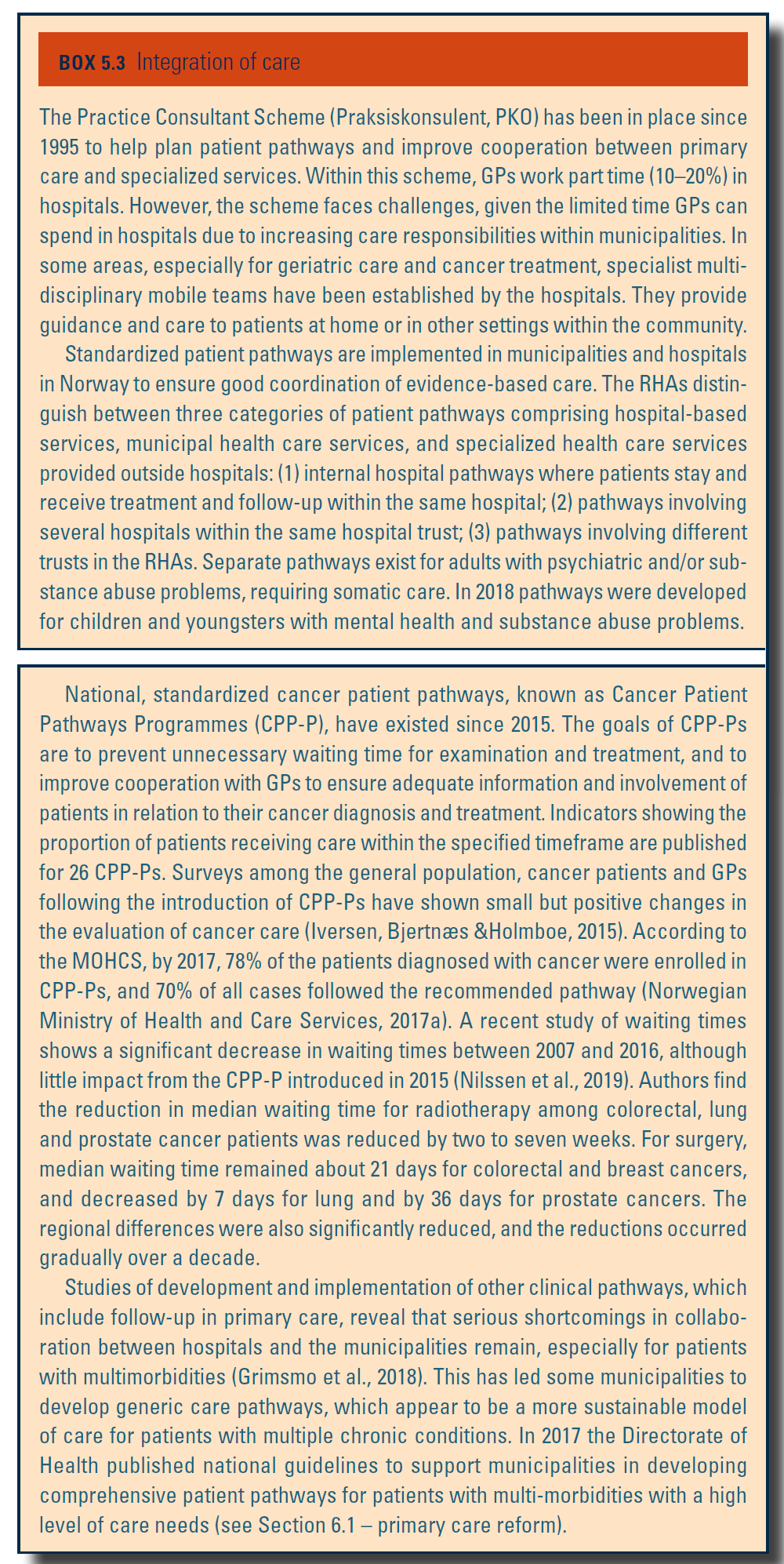
Investment decisions at the municipal level are taken by the municipalities according to local needs and means. There are also earmarked central grants for certain investment, e.g. for providing local emergency care beds to support early hospital discharge (see Box5.3).
Box5.3
4.1.2. Infrastructure
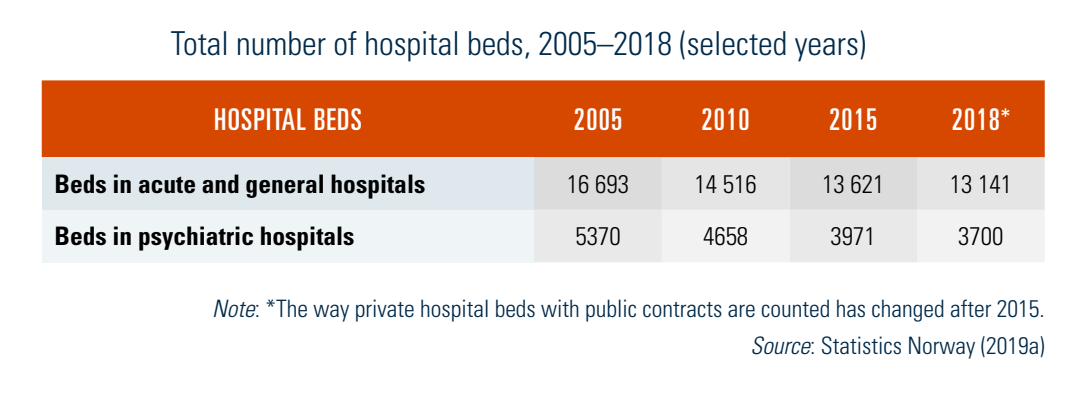
In 2017 there were 3.2 acute hospital beds per 1000 inhabitants in Norway, more than other Scandinavian countries but much less than in Germany, for example (Fig4.1). In total, there were around 17 000 beds in the hospital sector in 2018 (Table4.1). The number of hospital beds has been declining over the years and reflects the government’s efforts to improve resource allocation by shifting inpatients into outpatient settings in the community and into day surgery.
Fig4.1
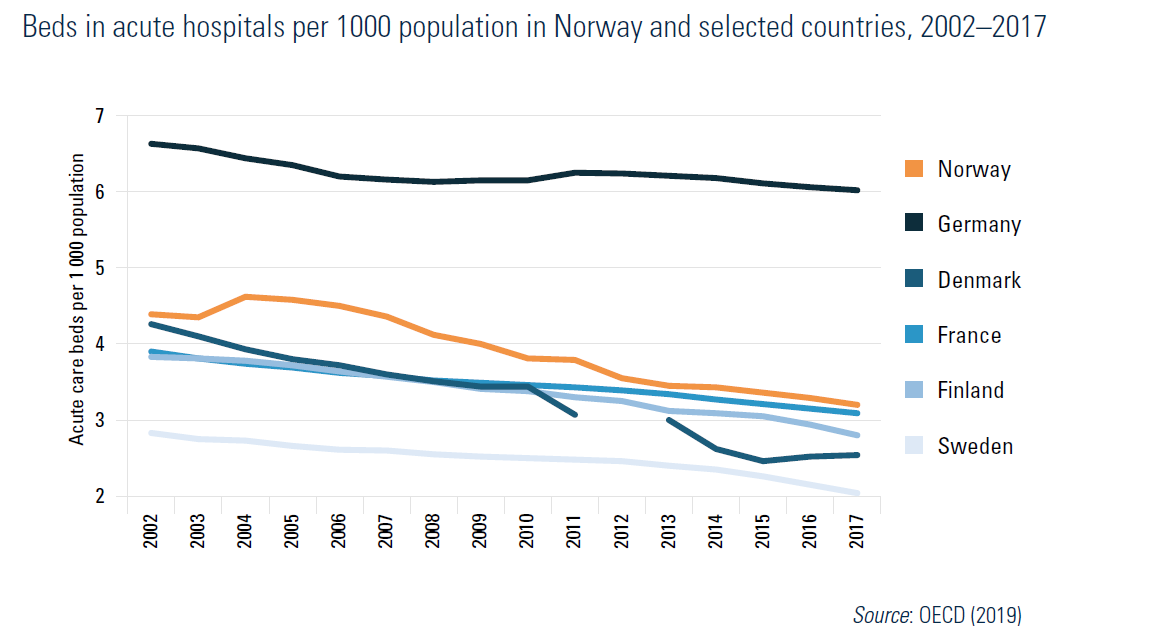
Table4.1
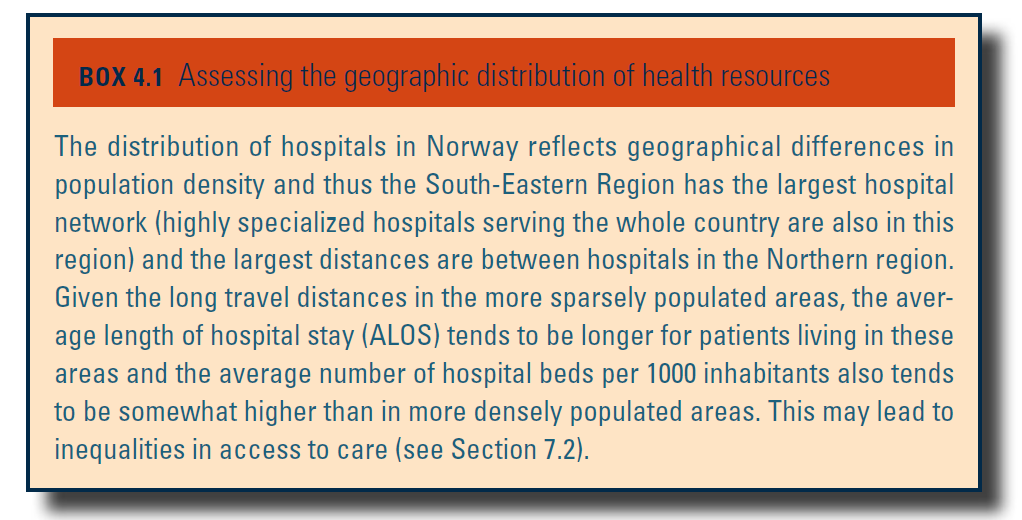
The geographic distribution of hospital beds is uneven (see Box4.1).
Box4.1
4.1.3. Medical equipment
Medical equipment is financed in the same way as capital investments (see section 4.1.1). The availability of medical equipment varies and its utilization rates are mixed compared to other countries in the EU (see Table4.3).
Table4.3

Almost all imaging diagnostic equipment is in specialist care. There are documented differences both between and within regions in accessibility of medical equipment such as positron emission tomography (PET) or computed tomography (CT) scanners, as well as palliative radiotherapy (PRT) (Asli et al., 2018; Office of the Auditor General of Norway, 2017).
The updated regulatory framework for general practitioners (GPs) largely preserves existing rules, but clarifies responsibilities of both the municipalities and GPs. It strengthens digital service requirements, obliging all GPs to offer online appointment booking through helsenorge.no and, from April 2026, and to provide suitable digital consultations via video, text or telephone. The upper age limit for working as a GP increases from 75 years old to 80 when both the doctor and municipality agree.
From 1 January 2026, reimbursement rules will allow GPs to receive payment for nurse led consultations when delegated, supporting enhanced task distribution and interdisciplinary practice, and contributing to increase capacity.
Changes in standards and national e-health solutions also adjust the financial model for municipalities and health authorities. Competence requirements for physicians in municipal health services are consolidated into one regulation, requiring specialist certification or progress in later stages of specialist training, with limited exceptions. These requirements aim to ensure safe services while balancing quality, patient safety, recruitment and flexibility.
References
Endringer i lover og regler fra 1.1.2026 – regjeringen.no https://www.regjeringen.no/no/dokument/lover_regler/endringer/endringer-i-lover-og-regler-fra-1.1.2026/id3141571/?expand=hod
Forskrift om fastlegeordning i kommunene (fastlegeforskriften) – Lovdata https://lovdata.no/dokument/SF/forskrift/2025-12-02-2405
4.1.4. Information technology and eHealth
IT use in the health system
The NHN was established in 2004. The NHN is responsible for provision of efficient and secure electronic exchange of patient information via a health communication network between all relevant parties within the health and social services sectors, including across the regions and different administrative levels. Since 2016 the NHN has been responsible for delivering ICT services to the central health administration and its subordinate agencies. Currently, all public hospitals and pharmacies and 365 municipalities, together covering over 90% of the population, are covered by this network (www.nhn.no). From January 2020 their responsibility will be extended to include Summary Care Records (see below), as well as e-prescriptions.
The NDE was established in 2016 with the mandate to implement the national policy on eHealth, establish the requisite standards, and administer the use of eHealth methodology nationwide (see also section 2.1). It has been responsible for the development of the above-mentioned Summary Care Records and e-prescriptions, which will be transferred to the NHN from 2020. While the NHN takes on more responsibility for implementation, it is envisaged that the NDE will strengthen its governance role.
The National ICT Health Trust, established in 2014 by the RHAs, currently implements a system of electronic medical records, known as Summary Care Records. By December 2018 the system was accessible to all citizens; however, only 35% had accessed their record and 6% entered or corrected their information (Norwegian Directorate of eHealth, 2019). At the same time it was used by 71% of GP practices and 86% of pre-hospital emergency medical services (see section 5.5).
Almost all (98%) GP practices have computers. According to the NDE’s monitor (Norwegian Directorate of eHealth, 2019), in early 2019 more than 400 municipalities (out of a total of 429) had an electronic system for exchanging patient information with hospital trusts, as well as a system for exchanging patient information among GP practices. Most GP practices (93%) use computers and decision-support systems during consultations. The use of electronic exchange of patient data is also high. The use of e-referrals to specialist and hospital care has increased dramatically since 2013. In 2017, 96% of the municipalities sent electronic referrals to hospitals. In 2017 nearly all patient information sent from hospitals to municipalities was sent electronically.
E-prescriptions were implemented nationally for GPs in 2011 and for hospitals in 2016. By the end of 2018 more than 92% of all human prescriptions were e-prescriptions and about 12% of these prescriptions were issued by hospitals (Norwegian Directorate of eHealth, 2019). With e-prescriptions, patients can collect their prescription medicines from any pharmacy in Norway and may also authorize others to collect their medicines for them. In addition, since 2013 a service within helsenorge.no has given patients access to information about their active prescriptions and medicines collected during the past month, as well as about all prescriptions in the previous three years. The next step is a roll-out of e-prescriptions for unit dose dispensing.[5]
Telemedicine is routinely used to improve access to care and to provide continuous education to health personnel in remote areas. In recent years the use of telemedicine has been piloted for monitoring people with chronic diseases and a national scale up of the pilots has been recommended.
According to Statistics Norway, use of the Internet as a source for health-related information increased from 39% in 2009 to 65% of the population in 2018 (Statistics Norway, 2019a). The Directorate of Health promotes the use of mobile applications for those who seek a healthier lifestyle and to improve their mental well-being. Via the website “Bare du”, people can download relevant applications, e.g. to help them give up smoking and reduce alcohol intake.
- 5. The unit dose dispensing system of medications is a pharmacy-coordinated method of dispensing and controlling medications. ↰