-
01 January 2023 | Country Update
Compulsory waiting time of five days for abortion abolished
5.2. Patient pathways
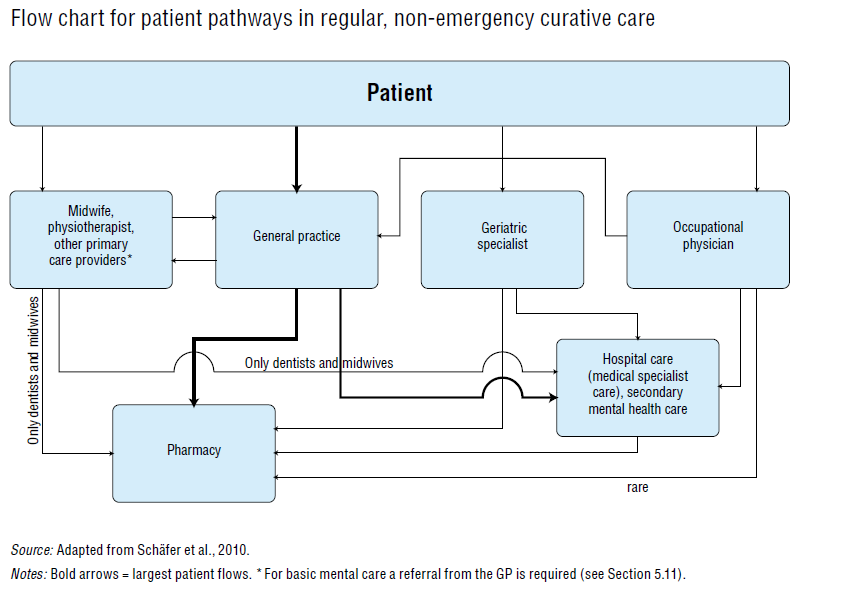
In most cases the first contact with the health care system takes place after a medical problem occurs. Which health care provider the patient consults, and which path the patient follows through the health care system will depend on the type and severity of the complaint.
Fig5.1 shows the pathways of patients in curative, non-emergency care. The bold arrows represent the pathways that the majority of patients follow; first they contact their GP who treats the patient, prescribes medication or refers to a secondary care provider, or a combination of these possible actions. Box5.1 describes in more detail an example of a specific case: a patient who needs a hip replacement.
| Fig5.1 | Box5.1 |
 |  |
In the case of emergency care, patients can contact their GP or GP out-of-hours service. The patient can also go directly to the emergency ward, but this is not the preferred route. The pathways of patients for emergency care are shown in section 5.5. An example of a man with acute appendicitis is provided in Box5.2.
Box5.2
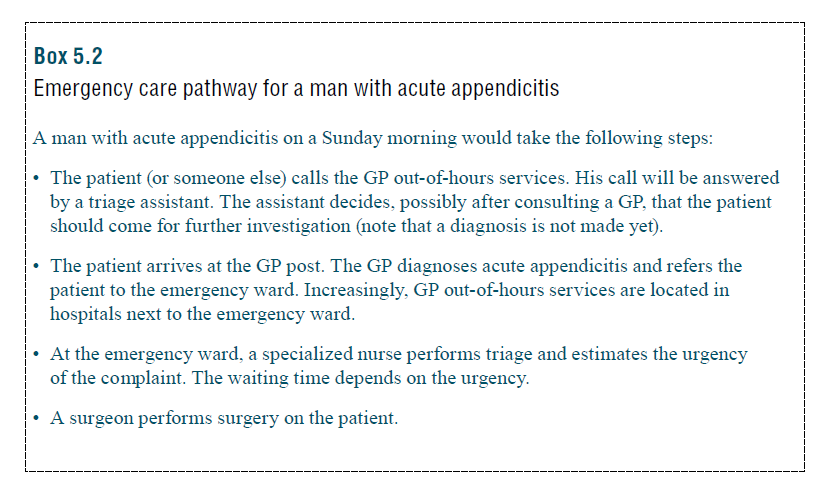
Another possibility is that the man goes directly to the emergency ward, without consulting a GP. Around 60% of the patients of emergency departments come without referral. However, the preferred route is via the GP out-of-hours services.
As a result of the ageing population, there is an increasing number of patients with multiple chronic conditions. The coordination of care for these persons is important; how this is achieved is described in Box5.3.
Box5.3

Integrated care
Due to the growing numbers of older citizens and people diagnosed with chronic diseases, integrated care has gained the attention of policy-makers and care providers. Integrated care is proactive, multidisciplinary and well coordinated care that is tailored to the individual patient’s needs, priorities and preferences. Integrated care approaches in the Netherlands target two main groups: (1) people with chronic diseases, and (2) frail older people.
Chronic illness care
The implementation of a national integrated care strategy in the Netherlands is currently disease-specific and focuses on the care for patients diagnosed with specific chronic diseases, such as diabetes or COPD. What is considered appropriate care is laid down in a nationally agreed protocol or “care standard”; currently 14 such protocols are available. Based on these care protocols, primary care groups consisting of 4 to 150 GPs and other primary care providers develop their care programmes, which need to be contracted by private health insurers. The care group coordinates the care and pays the different care providers involved. Patients are free to participate in integrated care or to organize the necessary care themselves. Integrated care for COPD, diabetes and vascular risk management (VRM) are financed by bundled payment.
In addition to these disease-specific care programmes, there are multiple initiatives that have a more overarching needs perspective. Especially for patients suffering from complex needs, such as multi-morbidity patients, disease-specific strategies often fall short in providing appropriate care (Gijsen et al., 2013). For these patients it may be important to integrate medical care, social care and/or home care, as well as community services. Efforts are being made to extend disease-specific care programmes with case management principles for patients with co-morbidities (Rijken et al., 2014). In the CasCo programme, for instance, trained practice nurses apply case management in addition to diabetes management. The INCA model (Snoeijs, Struckmann & van Ginneken, 2015) stimulates an integrated approach using the care modules of the care standards mentioned above. Stepped care modules, also covering health behaviour and psychological issues, are described and an individual care plan is developed, based on the patient’s individual needs and situation. This approach, which is currently being piloted, may suit the needs of patients with specific combinations of chronic diseases, for which care standards are available. However, there is no national strategy to provide integrated care for all patients suffering from multi-morbidity.
Care for frail older people
To improve integrated care for older people with complex care needs, the National Care for the Elderly programme was set up, allowing regional networks to experiment with models of integrated care delivery exceeding the boundaries of existing legislation and financing structures (CSO, NFU & ZonMw, 2012). Between 2008 and 2016 a total of 125 innovative approaches have been implemented. An example is U-CARE, which aims to improve the identification and monitoring of general practice patients aged 60 years and older at high risk of developing frailty. It makes use of a software application to detect potentially frail patients. A multicomponent care programme integrating medical, social and home care is delivered by trained practice nurses. The programme has proven to result in less functional decline (Bleijenberg, 2013).
In the Netherlands, abortion services are part of insured care. Until now, women who were seeking an abortion had to go through a compulsory waiting period of minimum five days in which she was meant to consider whether to proceed with the procedure. As of 1 January 2023, this waiting period no longer has a five-day minimum and is instead determined in discussion with physicians.
References
Verplichte minimale bedenktermijn bij abortus vervalt | Nieuwsbericht | Rijksoverheid.nl: https://www.rijksoverheid.nl/actueel/nieuws/2022/07/08/verplichte-minimale-bedenktermijn-bij-abortus-vervalt