-
28 March 2025 | Policy Analysis
Housing, Support and Care for older people (WOZO), a multi-stakeholder agreement -
30 March 2024 | Policy Analysis
Implementing the Cross-sectoral Care Agreement: A stepwise approach -
09 July 2019 | Country Update
Sectoral agreements for paramedical care -
26 September 2017 | Country Update
Dutch GPs spend more time on elderly patients -
16 June 2017 | Country Update
Sectoral agreement for medical specialist care continued for 2018 -
16 June 2017 | Country Update
Budget for GP care may increase with 2.5% in 2018 -
13 February 2017 | Country Update
About 10% of the 2015 budget for youth care and social support not spent in the first year after the reform
6.1. Analysis of recent reforms
The Dutch health system has for many years been characterized by a large number of reforms, both large and small, at all levels of the health system. The focus in this edition of the Dutch Health System Review is on the period since 2006, when a large health insurance reform was implemented, which is still having an impact today, and which was followed by another major reform in the field of long-term care in 2015. Furthermore, there have been important reforms in mental health care and psychosocial youth care. For an overview of the most important reforms before 2006, see the previous edition of the Health system review of the Netherlands (Schäfer et al., 2010). Box6.1 provides an overview of all key reforms since 2006.
Box6.1

Context
As the Netherlands is facing many issues related to the sustainability of healthcare, the Dutch government introduced a long-term transition program, which includes the Cross-Sectoral Care Agreement (IZA) and other healthcare agreements such as the Healthy and Active Living Agreement (GALA) and Housing, Support and Care for Older People (WOZO) in an effort to tackle some of these challenges. In this policy analysis we further elaborate on the WOZO agreement.
In 2022, the Dutch government introduced the WOZO program together with 40 stakeholders in long-term care (including umbrella organizations of patients, health insurers, municipalities, home care providers and healthcare professionals). The WOZO is a policy program on housing, support and care for older people lasting five years in total (Programma Wonen, Ondersteuning en Zorg voor Ouderen). This program focuses on the long-term perspective of long-term care, consisting of a set of measures, initiatives and projects aimed at making it future-proof. The Dutch cabinet has allocated approximately 1.5 billion euro to support this plan. The first evaluation of this program was published in December 2024.
Impetus
Due to an aging population with more chronic conditions and increasing life span, the demand for healthcare is increasing. However, the number of people working in healthcare and the number of informal caregivers is not growing at the same pace. Without appropriate changes to how long-term care is organized, a shortage is anticipated in the near future. Therefore, reorganization to optimize the use of available resources while ensuring high quality of care is essential.
Main purpose of the reform
The aim of the WOZO is to reform care for older people with a strong focus on self-reliance. The norm will be to “take care of yourself if possible, at home if possible and digitally if possible”.
Content
In more detail, the WOZO is centred on enabling older people to be as self-reliant as possible by (re)learning skills if necessary, staying fit, using assistive devices and receiving support from their environment. The program prioritizes delivering care digitally whenever possible and encouraging people to live at home unless no longer feasible.
The WOZO program is structured around five action points, each divided into multiple subthemes:
- Growing old together vitally in a suitable environment. This point focuses on stimulating people to think about their future, promoting cohabitation of younger and older people and knowledge development on and increasing reablement.
- Strong basic care for older people entails improving the collaboration between healthcare and the social domain and strengthening primary care.
- Appropriate long-term care for individuals who require continuous and intensive care. This care needs to fit their needs by for example developing a personal healthcare plan with a cross-sectoral approach.
- Housing and care for older people focuses on creating sufficient housing in an environment that fits their needs. For each municipality, it is calculated how many houses need to be built.
- Labour market and innovation directed towards keeping healthcare workers in the sector. With the help of technological and social innovations, healthcare workers will be deployed in the most efficient way to take care of older people.
Implementation steps taken/outcomes to date
Within WOZO, there have been initiatives for housing of older people, an awareness program for older people to assess their wishes for future housing and a study to gain insight into the decision to relocate by older people. Furthermore, incentive programmes have been set up to subsidize housing initiatives for older people. Assessing the effect of WOZO is challenging for several reasons. First, its changes align with a broader societal shift, making it difficult to isolate WOZO’s effects only. Secondly, many projects have not been fully implemented yet as they require collaboration between various stakeholders, such as healthcare providers and municipalities, which is a complex process. The involvement of the social domain could also be improved.
Additionally, the current healthcare structure does not fully support the optimal use of WOZO. The Dutch Healthcare Authority (NZa) has noted the following: To be able to finance initiatives structurally, the Long-term Care Act (Wlz) needs to be restructured: the core aims of WOZO “by yourself if possible, at home if possible and digitally if possible” need to be specified further. The old budget regime – nursing homes received a budget per client - needs to be changed. The newly introduced financial separation of housing and care is a challenge for institutions that have long-lasting commitments for their buildings. Future actions foreseen by the Ministry of Health are broadening the movement, integrating it into the Sectoral Care Agreement, collecting challenges and options for improvement and focusing on reablement and options to strengthen people living at home.
References
- Branchevereniging Kleinschalige Zorg. (16 May 2024). WOZO. https://bvkz.nl/wozo
- KMPG, Onderzoek meerkosten geclusterde woonvormen Wlz [Study on additonal costs for clustered housing under the Long-Term Care Act], 26 September 2022. https://open.overheid.nl/repository/ronl-c04be9d3ec51062bff977cea54bba37b89e55408/1/pdf/onderzoek-meerkosten-geclusterde-woonvormen-wet-langdurige-zorg-wlz.pdf
- Ministerie van Volksgezondheid, Welzijn en Sport. (4 July 2022). WOZO: Programma Wonen, Ondersteuning en Zorg voor Ouderen. https://open.overheid.nl/documenten/ronl-63e851f8e45b8662a4d04b1d5832b98231d40670/pdf
- Ministerie van Volksgezondheid, Welzijn en Sport. (n.d.). WOZO Monitor. https://open.overheid.nl/documenten/93666e52-8b83-4557-b33e-a69be7db924e/file
- Rijksinstituut voor Volksgezondheid en Milieu (RIVM). (2024, November 22). Plan van aanpak WOZO monitor niveau 3. https://www.rivm.nl/bibliotheek/rapporten/KN-2024-0047.pdf
- Rijksoverheid. (4 July 2022). Nieuw programma ouderenzorg: meer digitaal, meer thuis en meer eigen regie. https://www.rijksoverheid.nl/actueel/nieuws/2022/07/04/nieuw-programma-ouderenzorg-meer-digitaal-meer-thuis-en-meer-eigen-regie
- Rijksoverheid. (22 December 2023). Wonen, Ondersteuning en Zorg voor Ouderen (WOZO) [Letter to the Chairman of the House of Representatives]. https://open.overheid.nl/documenten/3a49d447-e8ab-41ca-af9a-483adc50af53/file
- Secretary of State. Programma Wonen, ondersteuning en zorg voor ouderen. Letter for the House of Parliament, 20 December 2024, #4026647-1076509-LZ, Kamerbrief vervolg programma Wonen, Ondersteuning en Zorg voor Ouderen | Kamerstuk | Rijksoverheid.nl https://www.rijksoverheid.nl/documenten/kamerstukken/2024/12/20/kamerbrief-over-programma-wonen-ondersteuning-en-zorg-voor-ouderen
In 2023, the Cross-sectoral Care Agreement was signed by a broad representation of stakeholders in healthcare. The Agreement outlined that healthcare should become sustainable, and that the current system must therefore change dramatically to meet future care demand. The vision of the Agreement is that health not healthcare should be the focus, guided by the principle of “personalized care at the right place”.
To initiate programs to achieve these objectives, the Ministry of Health has allocated 2.8 billion EUR for 2023–2026. The idea is to provide budget and a stepwise approach to implement overarching innovative projects that contribute to “the right care at the right place”, without involving more personnel in healthcare.
The impetus of this new funding is that new healthcare initiatives, especially when related to care under the jurisdiction of several Acts or sectors, and where the burdens and the benefits are felt differently among different stakeholders, often face financing challenges. There was thus a felt need by stakeholders for a different financing structure to bring these overarching projects to fruition, and also to facilitate additional experiments in programs targeting care innovation.
A process has also been outlined to come to meaningful initiatives that have a broad support. This starts with a regional approach. In the Netherlands, a region usually comprises several municipalities and is an already existing entity. Within a region, healthcare providers, insurers, municipalities, and patient organizations work together under the direction of the dominant health insurer and one of the municipalities.
- The process starts with writing a region review (the challenges) and plan (the targets) by the stakeholders in the region. Based on this, transformation initiatives can be submitted by healthcare providers, patient organizations, health insurers and or municipalities.
- Initiatives receive a quick assessment from health insurers based on whether the initiative contributes to changes in either care provided under the Healthcare Act; deployment of staff; regional/national redistribution of care; or real estate in the care sector.
- Once approved, a detailed plan should be written, containing SMART-formulated targets that can be reached within five years, an impact analysis, an implementation plan and commitment of all stakeholders involved and impact of sustainability.
- This plan will be assessed by two dominant health insurers of the region(s) involved. When a plan is approved, all health insurers in the region follow this plan. Notably, an initiative does not necessarily coincides with a region, but may cover a larger or smaller scale.
- Lastly, the Dutch Healthcare Authority (NZa) makes it administratively possible for each initiative to declare costs that cannot be financed via existing channels.
All regional reviews and plans are published at a common website (Regiobeelden en regioplannen: https://www.dejuistezorgopdejuisteplek.nl/programmas/integraal-zorgakkoord/regionale-samenwerking/regiobeelden-en-plannen). In April 2024, 102 transformation initiatives had already been positively assessed and 12 had received a green light (Goedgekeurde voorstellen en plannen: https://www.dejuistezorgopdejuisteplek.nl/programmas/integraal-zorgakkoord/transformatieplannen/goedgekeurde-voorstellen-en-plannen/?soort=transformatieplan,transformatievoorstel&weergave=lijst).
Reasons for a negative evaluation are diverse, including poor writing, not adhering to the regional plan or lacking commitment of relevant stakeholders. To assess their impact and adjust where needed in the process, results of these initiatives will be monitored, and sustainability will be assessed during the implementation process.
References
Bremmers S. 40% van de transformatieplannen door snelle toets [40% of the transformation initiatives assessed positive in the first assessment], SKIPR, 9 January 2024, accessed 11-04-2024.
Juiste Zorg op de Juiste Plek, Integraal Zorgakkoord (IZA) [Cross-sectoral Care Agreement (IZA), Integraal Zorgakkoord (IZA) (https://www.dejuistezorgopdejuisteplek.nl/programmas/integraal-zorgakkoord/)
Ministry of Health. Criteria regiobeelden en regioplannen. Samen werken aan gezonde zorg [Criteria for region views and region plans. Working together on healthy care]. Ministerie van Volksgezondheid, Welzijn en Sport, January 2023
Ministry of Health. Den Haag, Beoordelingskader impactvolle zorgtransformaties en inzet transformatiemiddelen. Samen werken aan gezonde zorg [Assessment framework impactful care transformations and use of transformation resources. Working together on healthy care]. Ministerie van Volksgezondheid, Welzijn en Sport, January 2023
NZa. Van regiobeelden naar doelgerichte regioplannen. Reflecties en aandachtspunten [From region views to targeted region plans. Reflections and areas of concern], NZa, 21 September 2023
Following the sectoral agreements in acute care, now also for the paramedical care sector an agreement is signed for 2019-2022.
Stakeholders have agreed to improve quality through stimulating scientific research that can be used to develop guidelines and quality standards. In addition, information for patients should be improved, both when searching a provider and during treatment. The paramedical sector should become organized in such a way that they can be a partner in the regional organisation of (integrated) care. Implementing information technology and working on completeness of electronic medical data records are important targets to facilitate benchmarking, learning, scientific research, and data transfer among care providers. The agreement aims to reduce the administrative burden for providers of paramedical care. Finally, to improve the negotiation process between insurers and providers, research into actual costs for providers is initiated. Insurers and providers have agreed to take this information into account in the negotiations for 2020.
The agreement is signed by national umbrella organisations for paramedical care, the umbrella patient association, the umbrella organisation of health insurers and the Minister of Health.
Authors
The policy that promotes elderly people living at their own home as long as possible leads to more work for GPs. Compared to 2013 GPs do not have more consultations with elderly persons, but the consultations take more time in 2016. Full time GPs spend on average 2.5 hours per month extra on direct patient care for the elderly (both consultations and palliative care) since the 2016 reform of long-term care. GPs report that they need more time for arranging care for the elderly, amongst others because they have to cooperate with more parties, such as municipalities and district nurses. A positive effect is that GPs think that the new arrangements in long-term care enables them to provide more adequate care to elderly patients.
Authors
The sectoral agreement for medical specialist care 2014-2017 is continued for 2018. The Minister of Health, health insurers and healthcare providers have agreed on this. The maximum growth for 2018 is established at 1.6% (on top of inflation). Most of the growth is dedicated to financing of the development of expensive medicines and the increasing demand of care for the frail elderly in the acute care sector. Besides there will be budget for the realization of substitution of care from secondary to primary care. There is special attention for the development of eHealth. Furthermore, providers and insurers will try to ensure that patients receive care in the right place, thus reducing unnecessary hospitalizations. The development of home nursing care is not yet included in this agreement. The Minister, providers and insurers thought it important to have clarity concerning the financial boundaries for 2018 in an early stage. For 2019 onward, the new government can start negotiations for a new sectoral agreement (if desired) after the formation of the new Cabinet.
Authors
References
The Minister of Health, primary care providers, patients and health insurers have concluded an agreement for GP care and multidisciplinary care (such as care for diabetes and COPD) for 2018. This agreement is a follow-up of the sectoral agreement for 2014-2017. The expenditure on GP care may increase with 2.5% (on top of inflation). The growth is dedicated towards creating more time for patients and should be used especially for the care for frail elderly, care in deprived areas, out-of-office care and coordination in primary care. Besides the financial agreements, there are agreements on the promotion of quality of care in the same areas as mentioned above. Furthermore, the agreement again stresses the importance of prescribing medicines in an effective and efficient way. On top of the agreed growth of 2.5%, an additional 75 million euro is available for promoting the substitution of medical specialist care to GP care
Authors
References
In 2015 youth care and home help became the responsibility of municipalities. Municipalities did not have previous experience with organizing (large parts of) this care. Many municipalities adopted a constrained spending policy because it was unclear what the actual expenditure would be in the new situation and because they preferred to save money for expected future budget cuts imposed by the national government. The nation-wide budget for municipalities for social support and youth care was 13.8 billion euro in 2015. Statistics Netherlands reported that 1.2 million euro of this amount was not spent. In 2015 there was a strong rise of court cases against decisions of municipalities concerning home and youth care, probably a result of the restrictive policies of municipalities. According to patient organisation Ieder(in), most court cases were won by clients. An often heard ruling was that municipalities had to do more in depth research for the assessment for individual citizens, instead of just reducing the hours of home care for all care recipients as a general measure.
Authors
References
Statistics Netherlands, NOS, Zorgvisie, Skipr
6.1.1. The 2006 Reform: introduction of a single insurance scheme and managed competition
The 2006 reform was targeted at the curative care sector. Curative care means care with the focus on curing the patient: in other words, restoring their health. The aim of the reform was to promote efficiency, to have less central governance and to improve access. By replacing the system of central governance, where possible, by a more decentralized system of regulated competition, the government expected to improve the performance of the health care system by introducing equal conditions for insurers and insured and strengthening the roles of citizens, insurers and providers in such a way that they are stimulated to use health care resources efficiently. Citizens get more financial responsibilities, more influence and more choice for their health plan. It was hoped that insurers would strengthen efforts to purchase care for their insured with a good price-performance ratio and, where necessary, more adjusted to the individual needs and wishes of their insured. The government remains responsible at system level for the accessibility, affordability and quality of care.
The policy process leading to the 2006 reform was discussed extensively in the previous Health System Review of the Netherlands (Schäfer et al., 2010). Below, the focus is on the changes since 2010.
The organization of curative care after 2006
The 2006 reform introduced compulsory health insurance for all citizens and managed competition for health care providers and health insurers. The assumption behind the reform was that competition should lead to affordable care with higher quality. As a result, three health care markets emerged (see also section 2.3 for an extensive description and Fig2.2 for a visual overview of the markets and their interrelationships).
Fig2.2

- In the health insurance market, citizens purchase a health plan from one of the health insurers. Major characteristics include: health insurers are obliged to accept all applicants; they may not differentiate premiums based on the health risks of the insured; and insured can change health insurer each year (Bartholomée & Maarse, 2006).
- In the health care purchasing market, insurers purchase care for their insured population from health care providers. The NZa formulates the services for which providers and insurers may negotiate prices. Health insurers are allowed to purchase selectively, as long as they meet their duty of care, meaning that they have to purchase sufficient care for their insured. If the care of a certain provider is considered to be of insufficient quality or too expensive, health insurers may decide not to contract.
- In the health care provision market, patients visit the health care provider of their choice, albeit with certain legal and practical restrictions. In the Netherlands patients are listed at a GP practice, but they are free to switch to another practice. In the case of a health issue, citizens go to the GP where they are listed. The GP may refer the patient to medical specialist care. The patient is free to go to the hospital of their choice, but cost-sharing may apply in the case of an uncontracted provider (see section 3.4.1).
Developments since 2006
With the introduction of the 2006 reform, numerous transitional measures were implemented to protect organizations from large deviations in their budget. Over the years these measures have become less protective or have been abolished. For instance, the freely negotiable share of the hospital budget was initially restricted to about 10% of the budget. The remaining share was still financed via the old budget system. The share of freely negotiable DBCs gradually increased until it reached 70% in 2012. The remaining 30% will stay regulated because the care cannot be planned (emergencies) or there are too few providers (see section 3.3.4). Another example is the degree of risk-bearing by insurers. In 2006 health insurers were compensated for, on average, 47% of their loss or had to pay back, on average, 47% of their profit (for hospital care the compensation for insurers was even higher: 74%). Over the years the ex-post compensations were gradually decreased to 6% in 2014. The compensation for higher expenditure at macro level (for example, an unexpected increase in health care expenditure at national level) was abolished in 2012. As a result, insurers bear more risk not only individually, but also collectively (van Kleef, Schut & van de Ven, 2014). Ex-post compensations reduce the incentives to purchase care efficiently and should not be necessary if the ex-ante risk adjustment system is working well (Douven, 2010). Over the years the risk adjustment system improved considerably, but still is not functioning at an optimal level (KPMG & Plexus, 2014). An extensive description of the (former) ex-post compensations can be found in the previous Health System Review (Schäfer et al., 2010).
Several cost-containment measures have affected the OOP expenditure of patients. Firstly, the mandatory deductible, introduced in 2008 at €150 per year, was increased to €385 in 2016. It has been a long-standing government policy that GP care is not subject to the mandatory deductible. Simultaneously, the health care allowance, a financial compensation for people on lower incomes, increased. To what extent the increase in the deductible has led to patients avoiding necessary care is the subject of discussion between providers and government. A recent report found that of the people who reported they had foregone GP care (15% of the respondents in 2014/2015), only one out of five mentioned financial considerations as a reason, a percentage that has been stable since 2009. The percentage of persons who did not follow up a referral increased from 20% in 2009 to 27% in 2013. Follow-up care is subject to the mandatory deductible. It is not clear why these people refrain from seeing a medical specialist (van Esch et al., 2015). Secondly, several treatments have been removed from the basic benefits package, including: the first 20 sessions of physical therapy for people with chronic conditions (for healthy people physical therapy was removed long ago); sleeping pills and tranquillizers (except for severe cases); statins; gastric acid blockers; stand-up-chairs; walkers and simple walking aids (Kroneman & de Jong, 2015). Furthermore, in 2014 several financial compensations for chronically ill or disabled people were abolished, such as partial compensation for the mandatory deductible and for the extra expenditure due to their condition. Municipalities may decide to provide such compensations under Wmo 2015 but are not obliged to do so.
In the first years after the reform, health care expenditure still increased at a higher rate than was expected (or desired). From 2008 the Minister of Health initially tried to curb these expenditure by charging back over-expenditure from the providers by having them pay back a fixed percentage of revenue, without differentiation towards high- and low-cost providers. This appeared to be ineffective and was perceived as unfair by those providers that had been cost-efficient. Therefore, from 2011 onwards the Minister of Health, together with the umbrella organizations of providers, insurers and patients, reached agreements on targets for cost-containment and improvement of quality of care (see section 3.1). Health insurers should better use the selective contracting tool and together with hospitals work on a better concentration and distribution of hospital care. Overcapacity should be reduced and pharmaceuticals prescribed more rationally (Ministry of Health, Welfare and Sport et al., 2011).
A massive protest among GPs led to an agreement between health insurers and GPs in 2015 restoring, inter alia, their prescribing freedom and relieving the administrative burden (Steenbergen, 2015). Furthermore, the ACM has started allowing collective GP negotiations as long as it is in the interests of the patient.
Over the years several types of care were transferred from the (former) AWBZ to the Zvw, such as curative mental care in 2008, geriatric rehabilitation in 2013 and home nursing care in 2015, resulting in a broader basic benefits package. In addition, a shift also took place within the Zvw: parts of outpatient pharmaceutical care were shifted from pharmaceutical care to medical specialist care. Several expensive medicines (TNF-inhibitors in 2012, expensive oncolytica and growth hormones in 2013 and fertility hormones in 2014) have been excluded from the GVS (see section 3.3.1) and now have to be paid from the hospital budget. The reasons for this shift were: (1) to make clear who was responsible for these medicines; in practice it was not always clear whether a drug should be seen as part of hospital care or as part of outpatient pharmaceutical care; (2) to give medical specialists control of medicines that are part of a medical specialist treatment; and (3) to improve adequate purchasing of these medicines. The consequence for patients is that they have to go to hospital to obtain their medication, instead of the local pharmacy. A study among patients and health care providers revealed that most of them are satisfied with the change, and they have experienced an improvement in communication (van der Burgt, Lescure & van Dijk, 2015).
Impact of the 2006 reform
The outcomes of the acute care sector reform on population health are described extensively in Chapter 7.
The reform has not been very successful in curbing the costs of health care provision. Table6.1 shows the overspending of selected sectors of care for the period 2007 – 2012, while Fig6.1 shows overall spending in the health system for the period 2005 – 2014. The only sectors in which a reduction of costs was realized were the pharmaceutical sector and public health. This is mainly due to the preferred medicine policy of health insurers (see section 3.7.2) and cuts in the public health budget. One explanation for the growing expenditure is that insurers lack the tools, expertise and meaningful data to become effective care purchasers and to influence providers to reduce their costs. Furthermore, although the reform has reduced prices of hospital care, these gains were not translated into lower costs, but were compensated for by hospital care providers with a higher volume of care (Schut, Sorbe & Hoj, 2013). Another explanation lies in the higher than legally required financial reserves that insurers were holding. The latter received a great deal of attention, especially after the expected premiums for 2015 were announced, which were, on average, almost 10% higher than in 2014. Insurers argue that they need these reserves because they are bearing more risk, but several critics (the media, politicians and consumer organizations) demanded that these reserves should be used to lower the 2015 premium. Another argument for insurers to have higher reserves was the introduction of the Solvency II directive, implemented in 2016. Besides, higher premiums were necessary because of the shift of care from the former AWBZ to the Zvw. Against expectations, the actual average premium for 2015 (€1158 yearly) appeared to be only a little higher compared to 2014 (€1098), but still lower compared to 2013 (€1213) (Dutch Healthcare Authority, 2015d). After 2012 cost growth flattened due to the sectoral spending agreements and preferred medicines policy (Vandermeulen, 2014).
| Table6.1 | Fig6.1 |
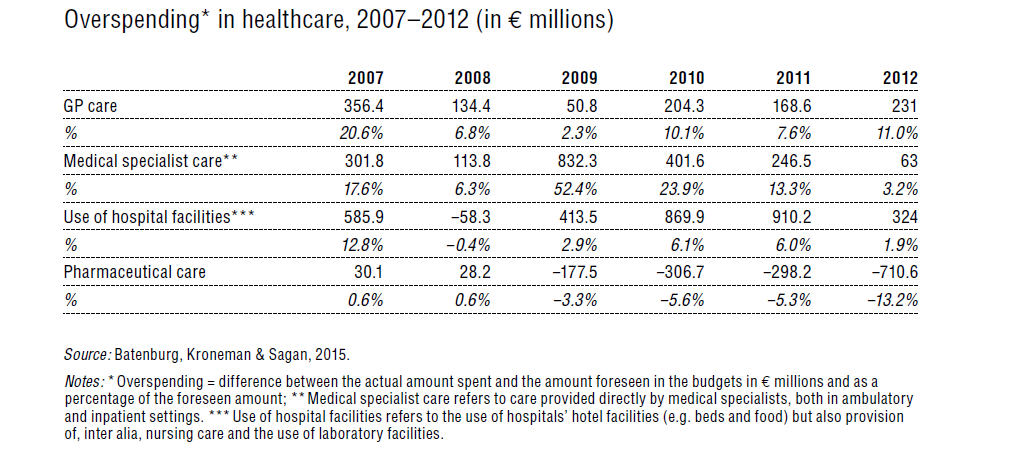 |  |
The free choice of health care provider is seen as an important means to improve quality, but in practice citizens hardly make use of this right. People tend to go to the nearest hospital and to the provider that is recommended by their GP. People use the Internet to search for information on health and diseases, but they hardly use the available information to choose a health care provider. Almost half of the Dutch population (48%) do not have sufficient knowledge, motivation or self-confidence to take an active role in managing their condition (van Esch et al., 2015). Furthermore, in 2014 the umbrella organization of Dutch patient associations (NPCF) revealed that according to their data, in practice changing is not always feasible. From 1100 patients (about 10% of the respondents) who wanted to switch, only one-third were successful in doing so (NPCF, 2014a). Although people do not always make use of their right to switch insurers, the threat that people or collectives (group contracts; see section 3.3.2) can switch insurer stimulates health insurers to purchase efficient and good quality care. In practice, switching insurers by collectives seldom occurs (KPMG & Plexus, 2014).
Quality of care is not yet a leading subject in the negotiations between health care providers and health insurers. A reliable set of quality indicators is not yet available, despite the efforts made to develop such indicators (Court of Audit, 2013). Insurers tend to negotiate on volume and prices, and quality is of secondary importance (Kooiman, 2014). In 2015, for the first time since the 2006 reform, a contract between health insurer and hospital explicitly concerned improvement of quality outcome. The cardiology department of the Catherina Hospital and insurer CZ have developed a method to measure quality. If quality improves, the hospital receives an extra amount of money.
To summarize, the markets are functioning now as envisaged, since almost all transitional measures have been abolished. There are a few weak points, however, that need to be addressed. Quality of care is not yet a leading principle in the negotiation process, the focus of which is mostly on price and volume, although there have been some initiatives for a limited number of DBCs. The influence of the patient on quality is still rather weak: information on quality of care, freedom of choice of health care provider and the option to switch insurer because of quality issues is hardly used. On the other hand the threat of switching empowers the insured, especially collectives representing large groups of insured, to negotiate attractive packages often tailored to their group members. In the health care purchasing market there appears to be an imbalance. The four main health insurers (representing about 80% of the insured) have to negotiate with individual care providers. Whereas hospitals are merging to increase their negotiation power, many small providers, such as GP practices and physical therapy practices, were hitherto not allowed to combine their efforts and have their associations negotiate for them (van der Bom, 2014). However, since 2015 cooperation is allowed if it is in the interests of patients. In contrast, the evaluation of the Zvw in 2014 concluded that there was an undesirable market power for health care providers, considering the excess growth, the high income levels of GPs and medical specialists, the lack of transparency and the existing practice variation (KPMG & Plexus, 2014). Irrespective of position, both views signal problems in the proper functioning of the market that need to be addressed. The introduction of managed competition has not yet brought a decrease in expenditure, although growth in expenditure has slowed down considerably over the years. The Minister had to reintroduce the traditional Dutch way of dealing with large societal problems, that is, through consensus-based economic and social policy-making (often called the “Polder-model”). Sectoral agreements between stakeholders and the Minister of Health were deemed necessary to curb the increase in health care expenditure.
6.1.2. Reform of mental health care: GPs in a central position
The new organization of mental health care
In 2014 mental health care was fundamentally reformed and is now organized in three segments.
- Patients first have to visit their GP with mental complaints. If feasible, the GP will treat the patient with the help of a mental health practice nurse.
- If the GP suspects a DSM-IV disorder, the patient is referred to the basic mental health care sector, which provides outpatient care for non-complex DSM-IV disorders. No OOP payments (other than the mandatory deductible) are required for this care in order that patients do not (1) forgo care due to financial considerations and (2) visit specialized care, where co-payments were lower.
- For complex disorders, specialized mental health care exists. The first three years of outpatient care and inpatient care are financed under the Zvw. After this period, care is financed under the Wlz (see section 5.11).
The policy process leading to the 2014 mental health care reform
The developments in the past 20 years in the mental health care sector are strongly related to the modernization and ultimately the abolition of the AWBZ. Mental health care used to be a separate sector that was financed completely from the AWBZ. As early as 1998 the wish was formulated to integrate curative mental health care with medical specialist care and thus transfer its financing to the predecessor of the Zvw, the ZFW. The Council for Public Health and Health Care (RVZ) argued that there was no difference between curative mental health care and somatic care (Council for Public Health and Health Care, 1998).
The mental health care financing system was substantially reformed in 2008. The goal was to remove all mental health care other than long-term mental health care from the AWBZ. The new regulations divided the financing system among three different sources: (1) mental health care with the emphasis on treatment and cure was transferred to the Zvw; (2) long-term care (longer than one year) was still financed by the AWBZ; and (3) public mental health care and social support were financed by the Wmo, administered by the municipalities. Most mental health care could not be characterized as long-term care and the financing was thus transferred to the Zvw. The Ministry of Health, Welfare and Sport estimated for 2008 that about 75% of the expenditure on mental health care would be covered by the Zvw and about 2% by the Wmo (van Hoof et al., 2008). As a consequence of these new regulations, curative mental health care is now financed through DBCs, based on the type and length of treatment, while long-term mental health care is based on care intensity and complexity.
For 2012 the Minister of Health introduced several measures to curb the growth in the mental health care sector after significant overspending occurred. Measures included, inter alia: introduction of extra OOP payments for patients; removal of the treatment of adaptive disorders from the basic benefits package; for long treatments a maximum of 18 000 minutes became applicable as a maximum tariff; a reduction from eight to five consultations covered under the basic benefit package for primary mental health care; and a government clawback amounting to €222 million from the sector in 2012 for the overspending in the years before, via the Macro Management Tool (macrobeheersinstrument) (Ministry of Health, Welfare and Sport et al., 2011, 2012).
Whereas the measures in 2012 were mainly one-directional, in 2012 the Minister of Health negotiated with the mental health care sector for a new agreement, in line with the previously concluded agreements for GP care and hospital care. The 2012 agreement, covering the period 2013 – 2014, aimed to safeguard the quality and financial affordability of mental health care. The goal was to organize care closer to the patient, by shifting care, when feasible, from specialist care to general care, from general care to GP care and from GP care to self-care (see above). The number of inpatient beds should be decreased by one-third, while care should be provided at home as much as possible (Ministry of Health, Welfare and Sport et al., 2012). Generic measures to claw back overspending are the ultimate measure when cost-containment targets are not met by the sector. It was agreed that yearly growth (excluding the growth in salaries and inflation) should not exceed the 2.5% in 2013 (Ministry of Health, Welfare and Sport et al., 2012), 1.5% in 2014 (lower than previously agreed) and 1.0% yearly in the period 2015 – 2017. This growth percentage is in line with demographic developments (Ministry of Health, Welfare and Sport et al., 2013).
Impact of the mental health care reform
A first evaluation of the new mental health care system revealed that substitution from specialist to generalist care seems to have been successful. Fewer patients use specialist care, while the number of patients treated in GP practice or basic mental health care has increased. The average expenditure on treatment for mental health care has increased now that it is provided as part of GP care. This is mainly explained by the fact that more GPs use the service of a mental health care practice nurse and charge a capitation fee for this care. Besides, the capitation fee for the mental health care practice nurse has increased from €1.97 per quarter of a year in 2013 to €2.73 per quarter in 2014 for every listed patient. As a result, costs have increased more than proportionally. Average treatment costs have also increased in basic and specialized mental health care. This may be explained by downward substitution (in other words, more severe cases have been treated compared to the former situation). Between 2011 and 2014 the percentage of unique patients visiting their GP for mental and/or social problems has been rather stable, so no increase in demand was detected (KPMG & Plexus, 2015). The authors of the evaluation stress that conclusions have to be interpreted with caution, because of the short time since the introduction of the reform.
6.1.3. Long-term care: decentralization and promotion of care at home and self-reliance
The continuous growth in long-term care expenditure financed under the AWBZ has long been considered untenable. In 2014 expenditure under the AWBZ amounted to €27 840 million, which represents 29% of the total health care budget (Budgettair Kader Zorg) (Ministry of Health, Welfare and Sport, 2015d). Long-term care could become unaffordable due to population ageing and subsequent increases in demand. Furthermore, the economic crisis has resulted in an increasing budget deficit and constraints imposed by the European Commission. Also the European Semester urged the Netherlands to reform long-term care. To keep the care affordable, a major reform was deemed necessary.
New organization of long-term care and social support [6]
The AWBZ was introduced in 1968 as an insurance against excessive costs of residential care for persons with disabilities or severe diseases. Over the years the AWBZ was extended to many other kinds of care, such as home care (nursing care and partly domestic care, supportive care for people with mental disabilities, sheltered housing; for more information on past reforms of the AWBZ, see the previous edition of the Health Systems in Transition review (Schäfer et al., 2010)). Also the eligibility criteria for residential care had become very broad, resulting in a large number of people living in residential homes who, with adequate care, could probably stay in their homes. Therefore, access to residential long-term care became restricted to persons needing supervision 24 hours per day (either medically, functionally or because of their mental condition). All others should remain living in their homes.
The reform of long-term care is based on the assumption that decentralization will lead to a more efficient organization of care. As municipalities are closer to the citizens, they are thought to be in a better position to make tailor-made, more efficient and cheaper arrangements for citizens than the care organized under the responsibility of the national government. A second important assumption is that in the past citizens relied too much on the welfare state. Citizens will have to be stimulated to take responsibility for their own care.
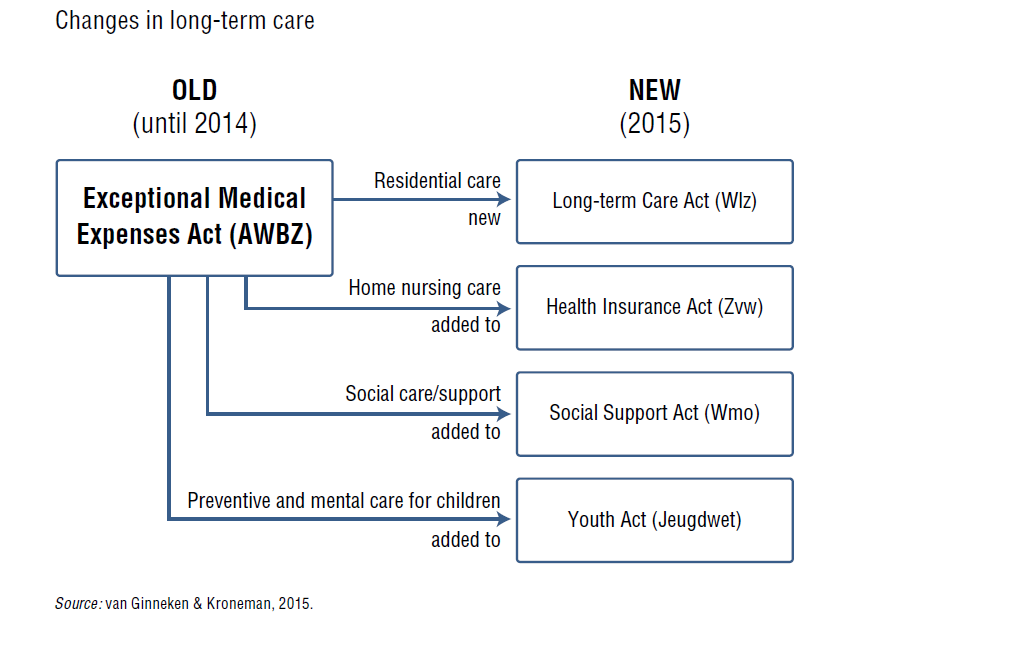
The old long-term care scheme (AWBZ) was split into four parts; three parts have been integrated into three existing laws and one new law has been introduced (see Fig6.2). Long-term care is now organized as follows: (1) if living at home is no longer possible, residential long-term care is available under the new Wlz; (2) insurers are made responsible for home nursing (which includes personal care), which is now part of the Zvw; (3) most forms of non-residential care (the social care part) were transferred to the municipalities and added to the Wmo; (4) preventive and mental health care for children were transferred to the completely revised Youth Act (Jeugdwet). The overall goals of this reform are to: (1) save costs, and thus keep long-term care affordable, starting with a saving of €500 million in 2015, reaching €3.5 billion annually by 2018; (2) keep people self-sufficient for as long as possible, especially given the high Dutch institutionalization rate; and (3) improve quality and coordination of care.
Fig6.2
 Residential care: Long-term Care Act (new Wlz)
Residential care: Long-term Care Act (new Wlz)
The new Wlz will replace the AWBZ as the main scheme for long-term care but with a much lower contribution rate (9.65%, with a maximum of €3241 per year in 2015). It will nevertheless absorb by far the largest share of the funding previously allocated to the old Act. Clients who, due to their limitations (functionally or mentally), are in need of permanent supervision have access to 24-hour inpatient care. Eligibility will be based on a needs assessment. Eligible people who nevertheless would prefer to stay at home can apply for in-kind care provision at home (Volledig Pakket Thuis, VPT) or for a personal budget. Previously, budget holders could manage their own budget, but following concerns about fraud, a government body – the SVB – now manages the budget on behalf of budget holders.
People who were already living in a residential home, but who do not meet the new, stricter entitlements, fall under transitional provision arrangements. This provision allows this group of individuals to retain their entitlement to long-term care for the rest of their lives.
Home nursing care (including personal care): the Health Insurance Act (Zvw)
Home nursing is now included under the Zvw, i.e. the curative care insurance scheme. With this shift, home nursing has moved closer to other types of primary care, such as GP care. Health insurers become responsible for the whole medical domain, from home nursing care to specialist hospital care. Ideally, this would foster a better integration of care. District nurses will play a key role in keeping people in their homes. They will visit home nursing recipients and assess whether it is possible for them to be more self-reliant. These nurses combine their nursing tasks with improving the cohesion between prevention, care, well-being and housing. In addition, the Zvw will now cover the first three years of inpatient mental health care, before the Wlz takes over. Previously, it covered only the first year. The shift was accompanied by the abolition of the cost-sharing requirements. In addition, home nursing care is not subject to the mandatory deductible.
Social care: the Social Support Act (Wmo) 2015
The objective of the Wmo is that municipalities will support citizens to participate in society. This includes, for instance, domestic care, transport facilities, aids such as wheelchairs and house adjustments. According to the national government, municipalities will be better able to provide tailored solutions and to promote informal care than the previous regionally organized (via care offices) system. Part of this care was already transferred to the municipalities under the first Wmo in 2007. Municipalities first explore the opportunities for applicants to take care of themselves, with the help of their social network. If these are considered insufficient, publicly funded support will become available. Interestingly, municipalities are free to organize tailor-made support for their citizens, which may lead to different solutions among municipalities. The rights-based approach of the AWBZ has been replaced with a provision-based approach. For example, municipalities may choose to substitute professional care with other solutions, such as care provided by neighbours or volunteers, whereas in the previous situation eligible people had a right to professional social support and domestic care. Since municipalities are closer to their citizens and in a better position to assess their needs, they are expected to organize care more efficiently by, inter alia, appealing more strongly to self-reliance. Thereby the state budget for non-residential long-term care will be lowered.
Long-term youth care: the Youth Act
The fully revised Youth Act, which came into effect in January 2015, makes municipalities responsible for care services targeted at parenting problems, developmental problems, mental health problems and disorders for all people under 18 years and their parents. Only those who are expected to depend on 24-hour supervision after they reach the age of 18 will receive care under the Wlz. The Youth Act intends to improve coordination of care by combining all care (except somatic care) into one Act and by making one organization, the municipality, responsible. Municipalities should install care and advice teams to reach this goal. In practice, a family experiencing problems will be assigned a care coordinator to ensure easy access to services.
Policy process leading to the 2015 reform
The time frame of introduction of the 2015 reform was rather short. The first plans were published in the coalition agreement of the government in October 2012. The first elaboration of the plans was sent to parliament in April 2013. A further refinement was discussed in the health care commission of the parliament in December 2013. Finally, the new Youth Act passed parliament in October 2013, the new Wmo 2015 in April 2014, the amendment of the Zvw, concerning home nursing care, in July 2014 and the new Wlz in September 2014. Both health insurers and long-term care providers tried to postpone the introduction to January 2016, stating that the preparation time was too short, but this was not successful.
Impact of the 2015 reform
The long-term care reform comprehensively alters both the financing of care and the organization of care. The responsibility for the organization of care was shifted to organizations (municipalities, health insurers) that had little or no previous experience of organizing such care. Taking into account the short time frame of the introduction and the assumption that from day one cost savings could be realized, it is not surprising that the introduction was accompanied with a great deal of social unrest. At the end of 2015 it is unclear whether the implementation problems are start-up problems or reflect more fundamental shortcomings.
In the run-up to the reforms, many stakeholders voiced important concerns, often relating to the short time provided to prepare adequately because uncertainties in the new legislation persisted well into 2014. Patient umbrella associations worried that patients who are ineligible for residential care could not stay at home because of a lack of adequately adapted housing (NPCF, 2013a). The associations also feared the lack of coordination in provision, which, in the new situation, is split across separate institutional arrangements (municipalities, health insurers). Another concern was the position of informal carers, and that the new arrangements would make informal care an obligation (NPCF, 2013b). Health insurers were more positive about the reform, but they feared not being ready for its implementation as their financial systems were not yet adapted (Zorgverzekeraars Nederland, 2014). The association of long-term care providers was positive about the reform, but also feared that 2015 was too early and voiced concerns that it was unclear who is entitled to care.
Half a year after the reform was implemented, it is clear that the process has been far from smooth. Many of the concerns and fears voiced in 2014 have become a reality. There has been continued heated political debate and media coverage. A newly published report by the Netherlands Court of Audit (Algemene Rekenkamer) called the expected savings unrealistic (Court of Audit, 2015). Problems were reported with late payments to providers, made by the SVB on behalf of budget holders, putting both the provider and the patients into difficulty. The SVB was not ready to fulfil this task, mostly due to inadequate staffing levels, computer system problems and increased numbers of applications for a personal budget. After apologizing to parliament for the chaos, the Ministry of Health will now allocate more funds to the personal budgets than originally planned. Patient umbrella organizations, which have installed a hotline where people can report problems, mention that in October 2015 there were still problems with access to care and with finding the right window to apply for care, and that needs assessments were mainly dealing with cost-containment instead of providing appropriate care. People report having to wait a long time before an application results in a decision for care (even longer than legally allowed). The provided care often does not meet the needs of the applicants. The patient organizations based their report on 10 821 complaints collected from June to October 2015 (Ieder(in), NPCF & LPGGz, 2015).
Another problem is the organization of domestic care (help with household chores under the Wmo), which has been the subject of a major funding cut. The government has set a savings target of 30% on the budget (Secretary of State of the Ministry of Health, 2014). Municipalities reacted in different ways: some abolished the provision of domestic care completely, some decreased the number of hours provided and some decided to keep the existing level of provision at the expense of other spending items in the municipal budget. To mitigate the negative effects, a transitional measure was agreed by which municipalities can temporarily apply for a higher budget for social support. Many recipients of social support (about 3000 in June 2015) have filed complaints with the municipalities (de Koster, 2015) and in some cases people have sued their municipality. One court ruling stated that municipalities are not allowed to cut into domestic care provision without an in-depth investigation of the situation of the recipient.
Lastly, the closure of residential homes is a concern because they also provide day care and meals to people living in the neighbourhood (Actiz, 2014). Municipalities felt that the new Wmo provided an opportunity for a broad and cohesive support package for citizens, but were concerned about a lack of funding and instruments to stimulate the self-reliance of citizens. The cooperation with health insurers and home nurses was another source of concern (Association of Netherlands Municipalities, 2014).
- 6. This section is mainly based on van Ginneken & Kroneman, 2015. ↰
6.1.4. Psychosocial youth care
The reform of psychosocial youth care sought to concentrate the responsibility of all mental health care and help with parenting for children and their parents into the municipalities. Youth care used to be scattered over several levels of government and organizations, leading to fragmented care provision, where care providers were not always aware of the involvement of other care providers in the same case. Therefore, as of 2015, municipalities have become responsible for most preventive and mental health care services for youth and their parents. This includes services targeted at parenting problems, developmental problems, and mental problems and disorders. With the shift of psychosocial care for youth to the municipalities, and with that the adoption of one legal framework and one financing system for youth care, the government aims to ensure that:
- the youth psychosocial care system is clear and straightforward and enables a faster and more effective organization of support and care;
- cooperation between local youth care providers is more effective;
- there is a more explicit focus on prevention; and
- care has to be purchased by municipalities.
The patient pathway for youth care can be described as follows. When parents or members of their social network experience or signal problems with their children, they can contact a gatekeeper (often a GP or a professional at one of the municipal centres for youth and families or one of the newly created municipal youth care teams). These gatekeepers will offer support and care by themselves as much as possible. The focus of the gatekeeper will be on timely prevention and empowerment of parents and children in order to minimize referrals to specialized care. When parents do not succeed, or the safety and development of a child are at risk, the municipality has to decide whether (and which) specialized services are needed for the child and their parents. Many municipalities have installed youth care teams, which assess the need of the family for support and, if necessary, provide this support.
The policy process leading to the youth care reform
The transition reflects the changing views, attitudes and approaches of professionals and policy-makers, who believe that the starting point of care is the parents and their child. The transition and transformation of the Dutch youth care system is laid down in the Youth Act, which was adopted by the Dutch parliament in 2014. The aim of the Youth Act is to empower the child and their parents and others in their social environment. The ultimate goal is a safe and healthy environment to grow up and optimal participation in society of children and young people.
It is intended that municipalities organize the care as close as possible to the child and their parents. However, in some cases it will not be possible to achieve this because of the nature or severity of the problems. In that case, cooperation between municipalities on a subregional level will be considered (Clarijs, 2014; Overheid.nl, 2014).
Impact of the youth care reform
A first evaluation of the Youth Act in the spring of 2015 found the following concerns. First, the administrative burden for youth care providers has increased due to the variation between municipalities in terms of care products for which the providers can bill the municipality. There are, however, also a few initiatives with population-based financing, which decreases the administrative burden (van Rijn & Dijkhoff, 2015). Second, the Monitor Transition Youth (Monitor Transitie Jeugd) records problems mentioned by clients. The main problems are related to information provided by the municipality on the continuation of care. Parents complain that they are sent from pillar to post. Parents also complain about untimely decisions concerning the (continuation of) their personal budget and that they are facing reduced personal budgets without clear explanations. Some clients do not feel heard or taken seriously. Furthermore, the privacy of clients is not well regulated. Since August 2015 municipalities may receive information from the care provider about the treatment of a client in order to check the legitimacy of the bill. It is not clear whether all municipalities handle this sensitive information carefully (Monitor Transitie Jeugd, 2015).