-
01 November 2022 | Policy Analysis
New financing system for curative mental care for adults -
31 May 2018 | Country Update
Changes in the GP payment system in 2018: age adjusted capitation fees (Segment 1) -
31 May 2018 | Country Update
Changes in the GP payment system in 2018: new payment options for integrated care (Segment 2) -
31 May 2018 | Country Update
Changes in the GP payment system in 2018: smaller practices
Payment mechanisms
Since 2015 the payment system for GPs consists of three segments. Segment 1consists of capitation and consultation fees and covers about 77% of practice turnover. Capitation fees used to be age-related, but the age categories now changed. Especially the 85+ have become more care intensive: , GPs spent more time on organizing care for this group due to the decentralisation of long-term care in 2015, in which elderly are stimulated to stay at home as long as possible. As a result GPs receive a higher capitation fee for this age-group. Since patients aged 65-75 are nowadays in better health and thus have become less care intensive, GPs receive a lower age related capitation fee for this group of patients. The Dutch Healthcare Authority is still working on a reform of the capitation fee for patients in deprived areas as the current system does not reflect the care intensity of these areas sufficiently.
Authors
Segment 2 of the GP payment system is the segment for integrated care payment. There were four care packages defined under this segment: care for diabetes mellitus type 2, cardiovascular risk management, care for COPD and care for asthma. Since 2018, the Organization and Infrastructure payments were added, which make it possible to finance the cooperation between care providers in a broad sense, for instance cooperation with district nurses, hospitals, physical therapists, municipalities, and mental care institutions. Cooperation will contribute to a strong primary care and prevent referrals to secondary care. These payments are payable as an extra quarterly capitation for each patient on the list, regardless their condition. A contract with a health insurer is mandatory and prices result from negotiations with health insurers. In contrast, for three of the already existing integrated care pathways (for COPD, Diabetes and Cardiovascular Risk Management) the obligation to have a contract with a health insurer is abolished. Since these pathways are considered nowadays as “care as usual”, GPs without a contract may claim a fixed tariff, settled by the Healthcare Authority.
Authors
The Dutch Healthcare Authority introduced a few changes in the GP payment system per 2018. The Authority examined the number of patients listed with per GP in 2015 and noted that there was a decrease compared to 2010. Therefore, the normative number of listed patients for what is considered a full-time GP is lowered from 2168 to 2059. This number is the starting point for tariff calculations by the Dutch Healthcare Authority.
Authors
Paying for health services
Hospital care under the Health Insurance Act (Zvw)
Dutch hospitals have been paid through DBCs since 2005. The DBC system was inspired by the concept of DRGs, but it constitutes a newly developed classification system. While DRG systems group patients according to diagnosis or procedure with the highest amount of needed resources into a single DRG, the DBC system provides a DBC for each diagnosis-treatment combination and thus more than one DBC per patient is possible. This should provide more flexibility in the case of multi-morbidity, where more than one medical specialist treats the patient during one admission or the patient receives more than one treatment from one medical specialist.
The DBC system forces hospitals to provide an overview of the total costs of each treatment from the first consultation until final follow-up check after treatment. The DBC system is considered the basis of managed competition in hospital care and should increase the efficiency of the hospital sector. The Ministry of Health, Welfare and Sport, together with hospitals, medical specialists and insurers, has established the treatment options and associated costs for each diagnosis. DBCs (since 2012 also called care products) cover the costs of medical specialist care, nursing care and the use of medical equipment and diagnostic procedures. Apart from these direct costs, indirect costs such as education, research and emergency care are also included. The duration (within a certain range) of a hospital stay, or more or fewer diagnostic procedures, has no influence on the DBC. For patients who go to hospital for medical advice but are referred back to their GP without a diagnosis or treatment, different and less costly DBCs are available.
The NZa is responsible for adjusting and updating the DBC system. Hospital care providers are obliged to provide their DBC data to the DBC information system. In 2012 a new DBC system was introduced that drastically reduced the number of DBCs. Previously, 30 000 DBCs were applicable, but in 2012 this was reduced to 4400 because the system was considered too complicated, error-prone and susceptible to fraud. In the Netherlands the new DBCs are called DOTs (DBCs On the way to Transparency) to distinguish them from the old DBCs.
For the free segment (negotiable DBCs; see also section 3.3.4), the DBCs are automatically derived from the hospital information system. A programme, called the grouper, derives the care product based on a decision tree set by the ZiNL. This grouper provides a declaration code for each care product. This code, together with the negotiated price, is used for billing the insurer. For the regulated segment (non-negotiable DBCs), the NZa sets maximum prices. Patients get this care reimbursed in all cases, as they do when selective contracting is in place.
Some treatments that would disproportionally increase the cost of treatment, such as admission to intensive care or very expensive pharmaceuticals, are not included in the price of a DBC care product, but can be billed as an add-on: an additional reimbursement. Furthermore, the hospital may receive extra payment for costs which cannot be assigned to a DBC. Such payments may be, inter alia, payments for educational tasks and payments for maintaining an emergency department in areas with low population density, which would otherwise not be affordable.
Long-term care provided under the Long-term Care Act (Wlz)
Payment of providers of institutional long-term care is based on the intensity and complexity of the care provided. Intensity and complexity of care can be divided into several care intensity packages (zorgzwaartepakketten). A care intensity package is a specific package of care, prescribed by the characteristics of the client and the hours of care needed, and includes a description of the required care. There are different care intensity packages for different sectors of care. There are 10 packages for the nursing and caring sector, 14 packages for the mental care sector and 30 for the care for disabled people. The budget for each care intensity package is set by the NZa and covers personnel, housing and resources. In 2015 the tariffs of care intensity packages varied from €68 per day to €323 per day (Dutch Healthcare Authority, 2015a). The intensity of care a patient needs, and thus the corresponding care intensity package, is assessed by an independent organization: the CIZ. The responsibility of purchasing inpatient long-term care is delegated to care offices (Zorgkantoren).
The actual payment of Wlz-care depends on whether the patient receives the care in-kind or whether they choose a personal budget. For care that is provided in-kind, the patient settles the income-dependent cost-sharing requirements with the CAK. The CAK then pays the providers from the Long-term Care Fund on receiving a payment order from the care offices. When patients have chosen a personal budget, they contract their own care providers. The budget is paid to the SVB, which then takes care of paying the providers. Previously (before 2015) patients received the personal budget directly on their own bank account. To prevent fraud, this changed in 2015. Patients now send their contracts and invoices to the SVB. The patient pays the income-dependent cost-sharing to the CAK. Tariffs for personal budgets vary from €40 to €285 per day in 2016 (National Health Care Institute, 2015d).
Social support services provided under the Social Support Act (Wmo)
The municipalities pay the providers for Wmo home care services. The municipality settles the cost-sharing requirements or outsources this to the CAK. Municipalities purchase care from home care organizations via a public procurement procedure. This care is offered to the clients in-kind. Municipalities can independently establish the level of OOP payments by the clients. For patients who prefer to organize and purchase their own care, there is the option of a personal budget. Patients receive a budget based on their need for care. They can purchase this care from professional organizations or arrange their own care personnel. These may be professionals, but may also be family members or other non-professionals, who are directly employed by the patient. The municipal personal budget is also paid to and distributed by the SVB.
Mental health care
In 2014 a major reform was introduced in mental health care. For mental health care, the GP is initially responsible, and may employ a mental care practice nurse (POH-GGZ). The GP gets paid for the services of this practice nurse through a contract with the health insurer.
When the GP suspects a DSM-IV disorder, the patient is referred to basic mental care. Four care products have been defined for this type of care: short, medium, severe and chronic (Table3.5). For each care product, the NZa has established a maximum tariff. Providers and health insurers negotiate the actual reimbursed tariff. If providers have a contract with a health insurer, the bill is directly forwarded to the health insurer. If there is no contract, the bill is sent to the patient, who then can get the amount (partly) reimbursed from his insurer.
Table3.5

Specialized mental care for complex cases was formerly exclusively financed through the AWBZ. Since 2008, however, the first year of this type of care has been covered under the Zvw; this was extended to the first three years in 2015. The payment for mental care providers for complex mental care is based on the same system as curative hospital care (that is, DBCs). Only care that is the result of an individual and voluntary demand for care can be reimbursed under the Zvw. Treatment of the patient is categorized by the type of activity and the time spent on this activity and/or in days of stay for inpatient care in combination with the care intensity, varying from light to very intensive (Dutch Healthcare Authority, 2014c). The care is financed based on diagnosis and time spent in ranges (for instance: alcohol disorder: 250 – 700 minutes: €1102; 800 – 1799 minutes: €2280). This provides strong incentives to treat patients for longer, without better treatment outcomes (Douven, Remmerswaal & Mosca, 2015; Douven, Remmerswaal & Zoutenbier, 2015). Prices are calculated by the NZa, based on cost data of a sample of providers.
Inpatient youth care is financed in the same way as specialized mental care (through DBCs) and is, since 2015, the responsibility of municipalities. The DBC system was introduced to enable negotiations between mental care providers and health insurers. Since 2013 the budget system for mental care has been abolished and health insurers now purchase care from mental care providers. The current DBC structure is mainly based on diagnosis and time spent. The NZa found indications of upcoding (providers register a bit more time in order to receive a higher tariff). As a preventive measure, providers now have to register the actual time spent. The NZa advocates a further development of the product structure so that it better accounts for actual care demand.
For care that takes longer than 365 days, payment changes from DBCs to care intensity packages (see long-term care). After three years the care falls under the Wlz and continues to be paid via care intensity packages.
Pharmaceutical care
Inpatient pharmaceutical care (for both somatic and mental care) is included in the DBC system for institutional care. In outpatient care, pharmaceuticals will only be reimbursed by health insurers if they are included in the GVS (see section 3.3.1). A few expensive outpatient medicines have been shifted from the GVS and became the responsibility of the hospitals: these include TNF inhibitors (in 2012), growth hormones and expensive cancer medicines (2013), fertility hormones (2014) and all other cancer medicines (2015) (see section 6.1).
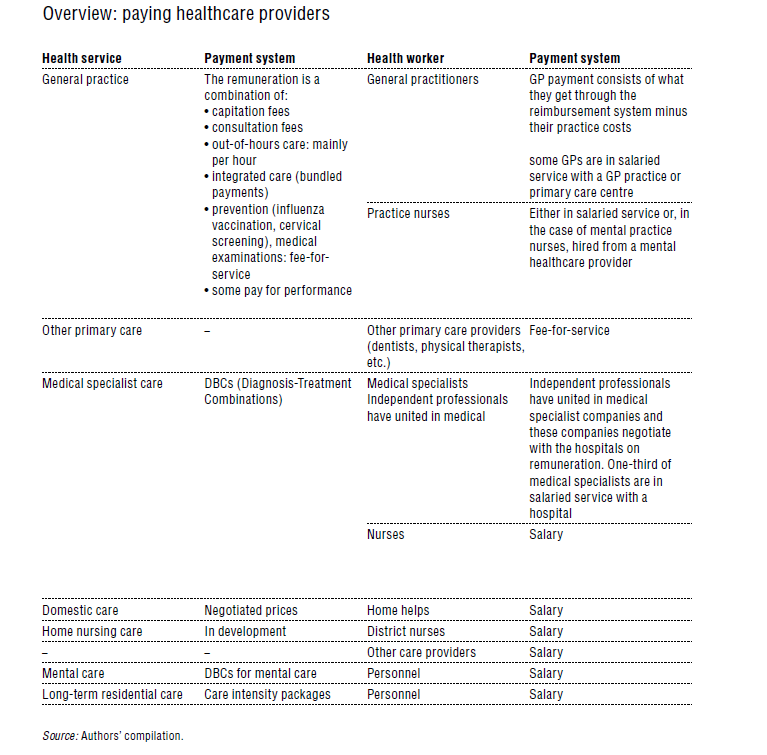
An overview of the payment mechanisms for health services and health workers is given in Table3.6.
Table3.6
Adult, curative mental healthcare is provided at three different levels in the healthcare system. Adults first go to their GP, where mild problems are treated by the GP or a mental care practice nurse. For more complex problems (that is, a DSM diagnosis), patients are referred to the basic mental care services, provided mostly by ambulatory psychologists and psychiatrists. Severe cases are referred to specialized mental care services, including inpatient care.
While each level had its unique financing system, as of 1 January 2022, an integrated financing system is in place. Care for children until 18, covered by the Youth Act and paid by municipalities, is not included as is long-term care, defined as those needing 24-hour care due to their (medical or mental) condition, including mental healthcare patients after four years of treatment.
How was care financed?
Basic services were financed via four patient profiles: short, middle, intensive and chronic. Specialized care was financed through diagnosis-treatment combinations (DBCs), like DRGs, but including elements of treatment (for example, length of treatment) and inpatient care in the second and third years of treatment via care packages, reflecting intensity of care (zorgzwaartepakketten).
What were shortcomings?
Providers experienced a high administrative burden, especially for specialized care, and it was difficult to organise care that shifted between care levels. DBCs had long throughput times, delayed insight into care expenditure, hampering monitoring and steering of care. They did not correspond well to actual care provided, insufficiently distinguishing between milder and complex cases, or a transdiagnostic approach. As many insurer-provider agreements focused on maximum reimbursement amounts, it also took a long time to know if the budget ceiling was reached. Additionally, patients could not understand the billing, and the system’s complexity made it difficult to introduce care innovations. Finally, the system organisation led to adverse incentives: with DBC payments being based on average care, more severe patients faced longer waiting times, leading to under-provision of care.
What is the new financing system?
All adult mental care (except by GPs) is now financed in one system characterized as pay-for-performance (PfP). Provider declaration of care occurs any day rather than at the end of a patient trajectory. Consultations and (in)patient stays are the only payable elements. Consultations can vary from short (5 minutes) to extended (120 minutes) in 15-minute increments, with a normative addition for indirect patient time. Regarding stays: there is day care and eight inpatient titles (according to care demands defined by intensity of care needed). Tariffs for consultations vary by setting (for example, monodisciplinary, multidisciplinary, inpatient) and provider (for example, medical specialist, psychologist, nurse). There is a special tariff for diagnostic consultations. The Dutch Healthcare Authority (NZa) sets the maximum price for each payable element.
The type of care provided as previously done through the diagnosis in the DBC and the characterization of basic care into short, middle, intensive and chronic is not an aspect of the payment system. Providers must deliver this information to insurers, however, to support forecasting mental healthcare needs in the future.
What are the challenges?
Although the system is presented as PfP, it has characteristics of a fee-for-service system (consultations and patient days are elements for reimbursement), possibly leading to provider-induced demand. Further, type of care is still incorporated and will likely be used in negotiations between provider and insurer in 2024.
Several provider-related problems exist. For example, issues with software providers meant that several providers are not yet able to file claims, which has considerable implications for patients and providers. Patient may have to pay the mandatory deductible for this and next year together next year. Providers must deliver information on care provision to the NZa, but if they cannot register claims, they cannot provide data. Meanwhile, there are privacy concerns related to these data.
Finally, providers complain that tariffs, set by the NZa and based on 2017 data, do not reflect current reality. NZa plans to conduct a new cost study, but until published, undesirable effects should be absorbed.
Authors
References
NZa, Beleidsregel Prestaties en tarieven geestelijke gezondheidszorg en forensische zorg – BR/REG-22137b [Policy measure Performances and tariffs mental health care and forensic care], https://puc.overheid.nl/nza/doc/PUC_658427_22/, accessed 21-11-2022
NZa, Informatiekaart informatiestromen in het zorgprestatiemodel en privacy versie 2 [Information chart on the flow of information in the care performance model and privacy, version 2], https://puc.overheid.nl/nza/doc/PUC_706881_22/, accessed 24-11-2022
Kiers, B. Zorgprestatiemodel duwt ggz-aanbieders richting miljoenenverliezen [Care performance model pushes mental care providers into million losses], Zorgvisie, 21-11-2022. https://www.zorgvisie.nl/zorgprestatiemodel-duwt-ggz-aanbieders-richting-miljoenenverliezen/, accessed 24-11-2022
Ten Houte de Lange, S. ICT zorgprestatiemodel ggz nog steeds niet op orde [ICT care performace model mental care still not on the road], Zorgvisie, 15-07-2022, https://www.skipr.nl/nieuws/ict-zorgprestatiemodel-ggz-nog-steeds-niet-op-orde, accessed 24-11-2022
Algemene Rekenkamer. Bekostiging van de curatieve geestelijke gezondheidszorg [Paying for mental care]. Den Haag, 2017
Paying health workers
GPs
In 2013 the providers of GP care, health insurers and the Minister of Health agreed that a new payment system for GPs would be introduced in 2015. The new system should contribute to the central role of primary care in the Dutch health care system. It should stimulate integrated care and cooperation between health care providers. It should also stimulate substitution from secondary care to primary care (InEen, 2014; National Association of GPs et al., 2013).
The new system consists of three segments. The first segment addresses the basic care of GPs. This is care for which the GP is the first contact and where the GP functions as a gatekeeper to secondary care. There are three different payment types in this segment. First, there is a capitation fee for each patient registered with the practice, which is differentiated according to age (above or under 65 years of age) and deprivation status (based on zip code). In addition, GPs may bill for each consultation and home visit. GPs can bill these two payment types even if they have no contract with a given health insurer. Furthermore, there is a fee for the practice nurse providing mental care and a few other types of care, but the GP needs a contract to receive payment. The NZa establishes maximum tariffs for the care elements in this segment.
The second segment applies to integrated care. In 2010 a bundled payment system was introduced for this type of care. Integrated care addresses care for patients with the following chronic conditions: diabetes type II, COPD, asthma and those at high risk of cardiovascular diseases. What is considered appropriate care is laid down in a care standard that has been developed for each of the four conditions. According to the system of bundled payments, a care group organizes all the care necessary for managing these diseases. Care groups are owned by GPs in a certain region, and vary in size from 4 to 150 GPs. The care group coordinates the care and remunerates the care providers involved. Patients are free to participate in a care group or choose their own care providers. About 80% of Dutch GP practices joined a care group in 2014 (van Hassel et al., 2015).
The care group is responsible for all the care that is related to the chronic condition of the patient. The care group negotiates a fixed fee per patient with a health insurer. A contract with a health insurer is a necessary precondition for bundled payments. GPs continue to receive the existing capitation fee. Payment for consultations that address the chronic condition(s) is included in the integrated care fee, while for issues that are not related to the chronic condition, the GP still receives the consultation fee from the insurer. If there is no contract with health insurers, GPs do not receive payment for this type of care. The costs of practice nurses for somatic care are covered by this segment.
The third segment is dedicated to pay-for-performance and innovation. These types of payment are also subject to having a contract with health insurers. The pay-for-performance scheme addresses, for example, the accessibility of the practice, efficiency of prescribing pharmaceuticals and efficiency in referring patients to secondary care, but also non-care-related issues such as accreditation of the practice (InEen, 2014; National Association of GPs et al., 2013). For 2015 the pay-for-performance scheme focused on adequate performance of the gatekeeping function and rational prescribing of medicines, as well as service and access (National Association of GPs et al., 2014).
At the level of GPs, the first segment should cover about 77% of the practice turnover and the other two segments 23%. At macro level, the Minister of Health, insurers’ associations, patient associations and the primary care association have agreed a growth rate of 1.5% per year for basic GP care (segment 1) and integrated care (segment 2). For the substitution of secondary care to primary care, innovation and the introduction of pay-for-performance (segment 3) an additional annual growth of 1% is permitted (InEen, 2014; National Association of GPs et al., 2013).
Out-of-hours services for GP care are mostly provided by GP out-of-hours cooperatives. GPs who participate in this system receive a per-hour compensation. For GPs who do not participate, specific fees for consultations, home visits and prescription refills are applicable that are higher than the fees charged during office hours. Almost all GPs participate in a GP out-of-hours cooperative.
As GPs are independent entrepreneurs, the income of GPs is the difference between revenue and practice costs.
Medical specialists
Medical specialists are either independent professionals organized in partnerships working in a hospital (60%) or they are in salaried service of a hospital (Rabobank, 2014/2015). Between 2008 and 2015 independent medical specialists were paid through the DBC system. For each DBC a normative time spent by the specialist and an hourly tariff were established. The norms were established by the NZa. The tariff was equal for all medical specialties and was based on research from the Normative Hourly Tariff Commission (Commissie Normatief Uurtarief), which was set up by the Minister of Health in 2004 after consultation with the Association of Medical Specialists (OMS).
Since 2015 health insurers have negotiated with hospitals on prices of DBCs, which include the payment of medical specialists. Independent medical specialists now have to negotiate their remuneration with the hospital they are working in. The Minister of Health hoped that independent medical specialists would become salaried professionals of hospitals. However, a questionnaire by the Federation of Medical Specialists among 67 hospitals found that only about 5% considered this option. In the other hospitals medical specialists mainly chose to unite in a medical specialist company (medisch specialistisch bedrijf) and negotiate their remuneration with the hospital. Another small share of specialists considered becoming shareholders in the hospital (de Kwant, 2014; Sijmons, 2014). The new situation led to a discussion as to whether independent medical specialists can still be seen as independent entrepreneurs. This is relevant because if the Tax Office now considers them to be in salaried service, this may have consequences for their fiscal position. There is no information available yet (late 2015) on the effect of these changes on the remuneration of medical specialists.
Pharmacists
Since January 2012 there have been two important developments in the payment of Dutch pharmacists. Firstly, a distinction was introduced between the costs of medicines and the related care activities provided by pharmacists, such as providing information and checking the appropriateness of prescriptions. For the care delivered by pharmacists, the NZa defined a number of services that may be subject to reimbursement. Secondly, the prices of all services are to be negotiated with health insurers.
In 2015, 13 different services were defined in the care that pharmacists deliver, of which seven are covered by the Zvw:
- care related to the delivery of a first-time prescription (introduced in 2014), which includes a check on the appropriateness of the prescription and potential interference with medicines already used by the patient; advice on how to take the medicine and providing information about possible side-effects;
- care related to the delivery of a prescribed medicine (repeat prescription) which includes, inter alia, a check on appropriateness, correct use and experiences of the patient with its use;
- instructions for the use of a device needed to take a medicine (such as an inhaler);
- medication review, a periodic evaluation of the medicines used by patients with a chronic disease;
- pharmaceutical counselling (including a medication review) in case of a hospital admission;
- pharmaceutical counselling in case of a hospital discharge; and
- pharmaceutical counselling in the case of day care or outpatient hospital visits.
The remaining, non-insured (secondary) services may relate to advice for travellers, advice on the use of self-care medicines, group counselling of patients with a specific disease (for example, diabetes mellitus) or using a specific drug, and services between pharmacists. The primary services have to be negotiated between insurers and pharmacists on volume and price in such way that in a given area there is sufficient pharmaceutical care for the insured. Health insurers may negotiate with pharmacists with respect to the availability and price of non-insured secondary services, but they are not obliged to do so.
For the delivery of medicines, there are two main options. Most health insurers follow a preferred medicine policy which means that they select one specific brand from different brands of pharmaceuticals with the same active substance. Generally, this is the cheapest available. Pharmacists are obliged to deliver only the preferred brand to the insured of a specific health insurer. Preferred medicines are listed (and thus may change) every six to twelve months. Another option is that the insurer sets a maximum price (price preference) and leaves the choice of the brand to the pharmacist. If the pharmacist does not succeed in buying the pharmaceutical for this price, he is not allowed to charge the patient for the difference. If he succeeds in buying the product more cheaply, he may keep the difference.
A summary of the payment mechanisms is provided in Table3.7.
Table3.7
