-
17 July 2025 | Country Update
Changes to patient registration and appointments scheduling -
22 January 2024 | Policy Analysis
Improving accessibility of health care by introducing patient transportation service
7.2. Financial protection and equity in financing
Authors
Vulnerable people, especially those residing in remote areas, have difficulties in accessing health care services. Patients who do not require ambulance services ought to utilize public or private transportation options. Public transport routes and time tables may not be in line with patients’ needs, who often resort to enlisting help from family members, neighbours or friends, with costs of private transfers being prohibitively expensive. The precise number of patients requiring transportation is not known. Nevertheless, for some for some of them a small number of municipalities have implemented minimal logistical support. As a result, in 2023 the government introduced a limited patient transportation scheme with the view of expanding the service nationally in 2024.
The ongoing reform of the hospital network seeking to concentrate the delivery of specialist services in major urban centres exacerbates the problem of access to health care outside the cities. Moreover, the implementation of centralization within the ambulance service has removed the possibility for patients to be transported from the centers to municipalities, where the ambulance vehicles were previously stationed.
The primary aim of the reform is to improve access to specialist services for patients living in rural areas through implementation of the patient transportation scheme.
The initial pilot is scheduled to run for 12 months from mid-2023 to mid-2024 in 20 (out of 60) municipalities. Current eligibility criteria cover people with low income and over 75 years old or severe disabilities or those socially vulnerable.
A set of essential legislation was issued in 2022–2023. In summer 2023, transportation was available for patients requiring haemodialysis and transplant services. From autumn 2023, the service was expanded to wider groups (see eligibility criteria above). In 2024, it is expected that the transportation service will be expanded country-wide. An initial state budget allocation of €7 million is projected to cover 40 000 journeys.
As of early 2024, the pilot data is being collected with no formal evaluation of the project carried out to date.
7.2.1. Financial protection
The Lithuanian health system is financed through a variety of taxes and contributions. NHIF receives and allocates about 80–85% of the total public funding on health. The health insurance contributions are the main source of revenue but its share has substantially decreased since the rise in unemployment in 2008–2010, with an increasing share of funding coming from the state budget. With the economy picking up again, this trend has reversed and the contributions from an economically active population now constitute a larger share.
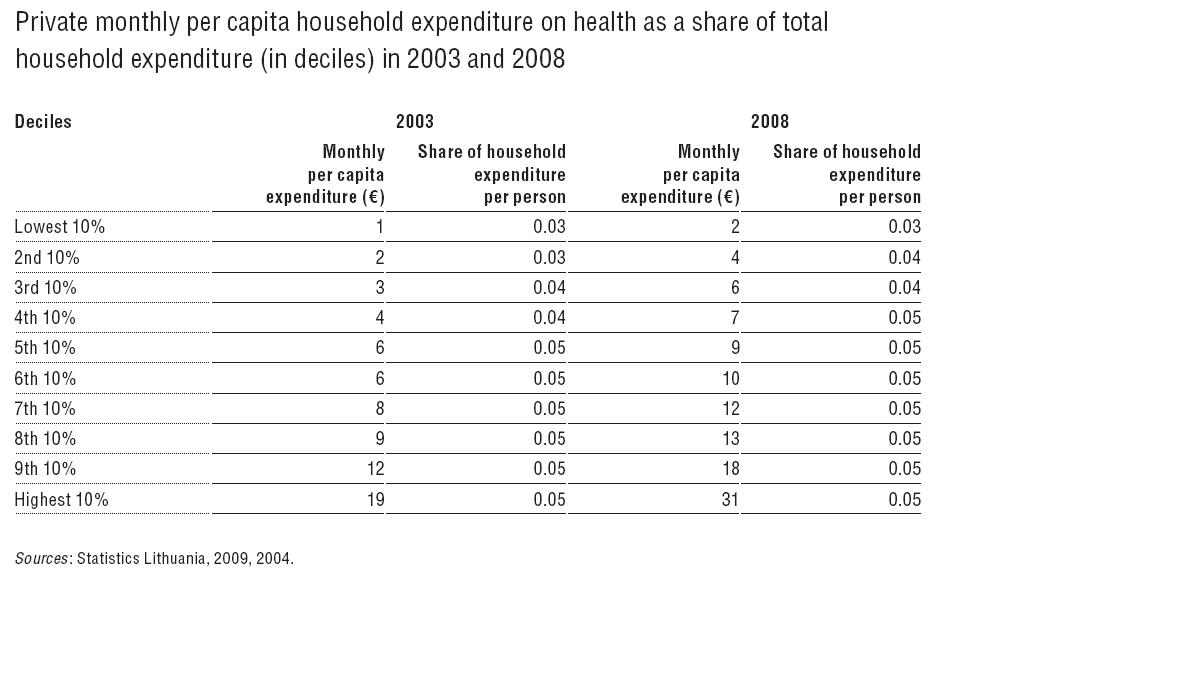
Household surveys showed that private per capita household expenditure on health was close to 5% of total household expenditure in 2003 and 2008, with the major share of this expenditure being spent on pharmaceuticals. Average private per capita household expenditure on health was distributed quite evenly across household expenditure deciles (Table7.1).
Table7.1
Direct payments in the private sector as well as frequent and sometimes substantial OOP payments for services provided by public providers may constitute financial barriers to accessing health care. The evidence on barriers to accessing services mainly comes from population surveys. For example, according to the Eurostat 2011 Income and Living Conditions Survey (European Commission, 2013), 4.3% of the population had unmet medical needs and a quarter of these responders found services too expensive. In the most deprived quintile, the unadjusted prevalence of unmet medical need reached 6.4%, almost half of these responders could not access care for financial reasons, compared with the prevalence of 3.5% among the least deprived group, in which only 1 in 30 respondents found services too expensive.
A number of surveys (see section 3.4.3) show that informal payments are widespread and may absorb a substantial share of patient’s income, particularly when both outpatient and inpatient treatments are required.
7.2.2. Equity in financing
In Lithuania, the main source of health-care financing is compulsory health insurance contributions, which are set proportionally to income levels. Vulnerable groups (about 60% of the population: children, elderly, disabled, unemployed, etc.) are covered by the state. This provides a degree of vertical equity and redistribution effect in the system.
However, as demonstrated above, large OOP payments add a substantial regressive component, as lower income and higher-need groups spend more proportionally on health care. Partly this is compensated by a reimbursement of 50–100% of the cost of the prescribed medication for the disabled, pensioners, those with chronic conditions, and so on.
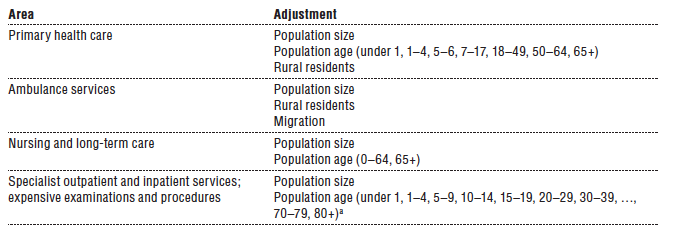
The budgets of territorial NHIF branches are determined according to a formula that adjusts for population size, age and urban/rural distribution, plus the cost of services in the past year (see section 3.3 and Table3.5).
Table3.5