-
21 May 2024 | Country Update
Latvia expands Center for Disease Prevention and Control’s helpline services -
31 January 2021 | Country Update
A review of hospital levels and networks is ongoing
6.1. Analysis of recent reforms
Latvia was among the countries that were hit hardest by the economic crisis of 2008. In analysing the reforms that took place in Latvia from 2007 to today, it is useful to define the reforms according to pre- and post-crisis period, as these periods mark a very different pace and scope of reforms. Just before the crisis (2007–2008) Latvia underwent a period of relatively few changes in the health care system. As the magnitude of the economic crisis had not yet emerged, there was no urgent need for reform. At the same time, politics and personal relationships obstructed a number of necessary (but painful) reforms to the health system’s institutional structures or hospitals. Nevertheless, several small agencies under the MoH were incorporated into the Public Health Agency and the availability of specialized ambulatory care and day-hospital services was improved.
The post-crisis period (2009–2012) was kicked off by the enormous financial constraints resulting from the financial and economic crisis in 2009, when the GDP contracted by almost 18% (see section 1.2). The subsequent reform process was very quick and was pushed through, almost without discussions and scientific analyses, within approximately one year: waiting times were extended; cost-sharing was expanded; and wages for health workers were cut (van Ginneken et al., 2012). The financial crisis provided the impetus to implement structural reforms that had been on the agenda for a long time but had not been carried out because of local opposition, such as the downsizing of the hospital sector (Mitenbergs et al., 2012).
Below are the main reforms from the second stage, which still have implications today:
- 2009: Cabinet Approval of the Safety Net Strategy – to avoid harming the most vulnerable populations during the economic crisis (in the health sector it entailed the exemption of people on low incomes from user charges);
- 2010: Start of the e-Health project funded by EU funds and continued until 2013;
- 2011: Cabinet Approval of Public Health Strategy 2011–2017;
- 2011: Creation of the NHS as a result of merging the Health Payment Centre (HPC) with the Centre of Health Economics;
- 2012: Creation of the CDPC as the new National Institute of Public Health; and
- 2012: Political decision to introduce the Nord-DRG system for hospitals: preparatory work for implementation.
For more details on the reforms between 2007 and 2012, please consult the previous Latvia HiT (Mitenbergs et al., 2012).
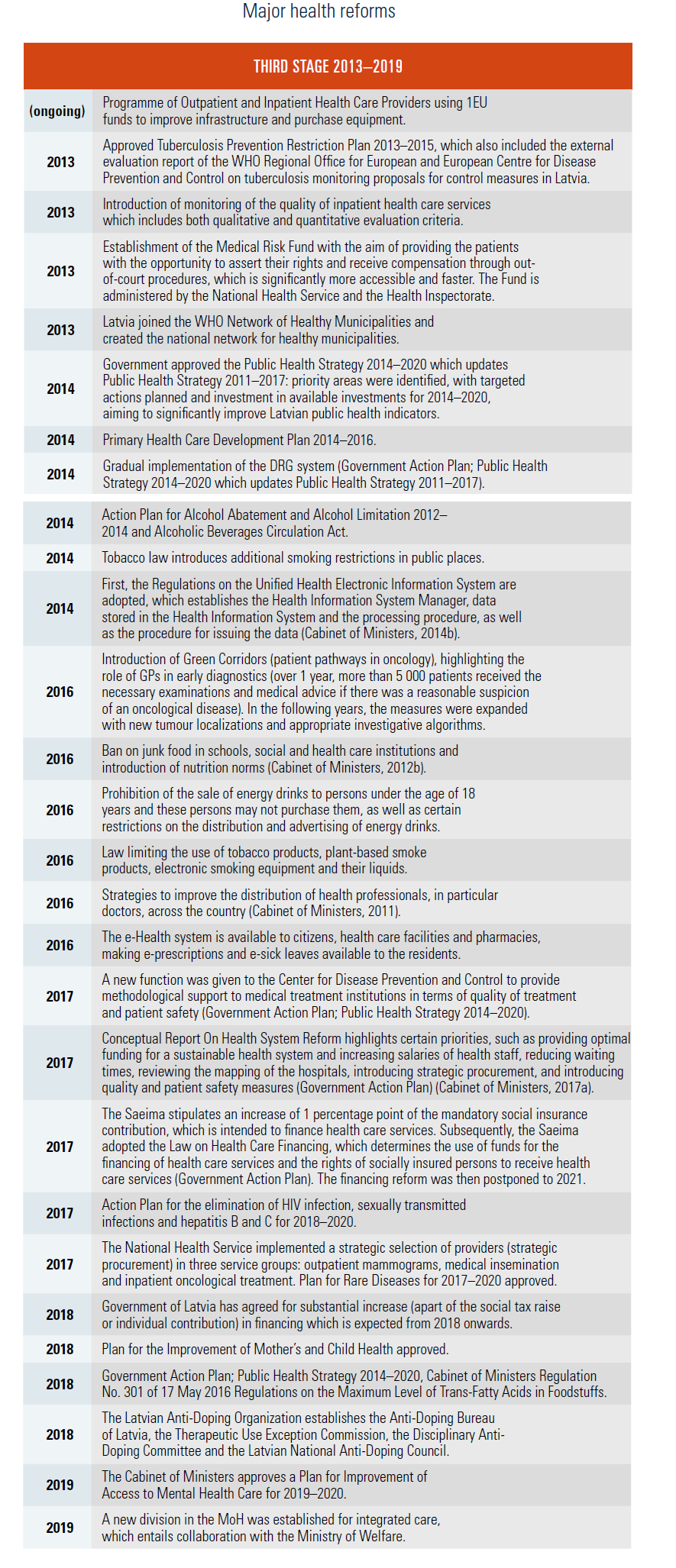
After the radical reforms of the immediate post-crisis period, the following years from 2013 until 2019 have been characterized by reforms that address priority areas linked to the burden of morbidity and mortality (Table6.1). In particular, these reforms aim to address cardiovascular diseases, oncology, maternal, newborn and child health, mental health, as well as a broader focus on tackling behavioural risk factors to improve the health of the population.
Table6.1
One key document is the Public Health Strategy 2014–2020, a medium-term policy-planning document based on the WHO Regional Office for Europe Health 2020 Strategy (Ministry of Health, 2014). The main objectives of the Strategy are: 1) to increase the number of healthy life years of inhabitants of Latvia (to reach 57 years for men and 60 years for women in 2020); and 2) to reduce the indicator of potential years of life lost by 11%. Steps in this direction are reflected in the overall view of the reforms that took place since 2013, and, overall, a few areas of focus can be identified as described below.
A substantial effort to address behavioural risk factors in the population
In Latvia, lifestyle-related risk factors (smoking, alcohol consumption, poor nutrition) are implicated in over 50% of deaths. Resources have been allocated for health promotion activities and legislation has been enacted. For instance, for tobacco, the aim of the 2014 Law is to protect public health, including the right of people to live in clean and unpolluted environment. The law regulates the circulation and control of tobacco products, plant-based smoking products, electronic smoking equipment and their filling containers, as well as advertising, sponsorship and packaging conditions, smoking restrictions and other related issues. Also, since 2018, foods that exceed the prescribed maximum levels of trans-fatty acids cannot be distributed in Latvia. Further, Latvia enforced prohibition of alcoholic beverages in environmental advertisements, and enforced prohibition of the retail sale of alcoholic beverages at the premises and territory of social care institutions, educational institutions, service hotels, state and local government offices.
Efforts to improve the financing of the health care system
A major health financing reform was approved in 2018, aiming to address the chronic underfunding of the system and proposing a two-basket system. The purpose of the law was to define the general principles and structure of the health financing system and to regulate the financial and organizational structure of the state compulsory health insurance. This new law could affect universal coverage for all citizens, introducing limitations to the eligibility to receive state financed health care services depending on participation in payment of social insurance contributions. The law defined two baskets of services: minimum and full. To be eligible to receive the full basket of services, individuals should make social insurance contributions or be in one of several exemption groups (such as children, the unemployed, retired, etc.), or make voluntary payments to the NHS set at 1 percentage point of minimum salary in 2018 (totalling to €51.6 per year) and 3 percentage points of minimum salary in 2019 (totalling to €154.80 per year). Those who do not make social insurance payments and do not belong to an exemption group would have access to only limited state-paid health care services, the so-called minimum basket of services, including emergency care, GP services, care for pregnant women and care for some diseases having potential major influence on the health of the population (see section 3.3.1 for more details). The Law was highly criticized both internationally and domestically, and in 2019 the newly appointed Minister of Health suggested postponing the introduction of differential eligibility based on payment of social contributions. In June 2019, the Saeima approved the amendments to the Law proposed by the MoH, postponing the introduction of the two service baskets until 2021.
The Health Care Financing Law does not include any measures to decrease OOP payments. The estimated total increase in health care financing from 1 percentage point of the social insurance tax was about €80 million in 2018, i.e., almost 10% of the state health care financing in 2017. According to the reform plan, the first priority is to increase salaries of health care professionals (physicians, nurses and support personnel). Therefore, it is foreseen that OOP payments through formal user charges and direct payments for services will continue to provide a substantial amount of total health care financing (see section 3.4).
While the new parliament postponed the health financing reform to 2021, one element has been implemented since 2018; i.e. additional revenues from the increase of the social insurance contributions rate by 1 percentage point are allocated for the financing of the health system.
The increase in financing brought by the 1 percentage point rise of the social insurance tax will support the improvement of accessibility and quality of the health care services. Further, to implement new measures to improve access to health care services in line with health care reform, at the end of 2017 the government granted an additional €113.4 million to the health sector for 2018. The budget of the MoH increased from €820 million in 2017 to €1.01 billion in 2018, the largest increase in the health care sector budget since Latvia regained its independence (European Commission, 2017).
Efforts to improve access and quality of care
Increasing access and quality of care has been a major area of focus. In particular, for mental health, there are plans to increase the competence of family doctors, nurses and doctors’ assistants in psychiatric care, to establish cooperation between family doctors and the outpatient team of psychiatrists and child psychiatrists, as well as to involve psychologists and functional specialists in the team of psychiatrists, promoting non-pharmacological treatment. Further, there are plans to introduce preventive examinations for children aged 1.5 to 5 years at the practices of family doctors for the evaluation of mental development, etc. Efforts to improve quality in primary care also include the introduction of quality criteria in the reimbursement of GPs (see section 3.7). A set of performance assessment indicators is also being developed for hospitals. In order to address the unequal distribution of health care professionals, especially doctors and specialists, since 2016 priority is given to those applicants for a residency who have an agreement with the municipality outside Rīga for an employment relationship starting in a medical institution outside Rīga after the end of residency.
Efforts to improve treatment of infectious diseases
Several infectious diseases are still main contributors to the disease burden in Latvia, and steps have been taken to address this issue. For example, the introduction of 100% reimbursement of hepatitis C medicinal products lead to a significant improvement in hepatitis C treatment, resulting in 80% virus-free patients, compared with 50–60% in previous years; early treatment of HIV-infected patients has started, and the proportion of HIV-infected persons who received treatment in 2016 has increased to 35–37% of the total number of HIV-infected persons.
An ongoing effort to downsize hospital care and support primary care
Strengthening primary health care is an ongoing priority to achieve a more affordable, effective and comprehensive health care system (see section 4.2.1, and section 5.3). The objective is increasing the role of primary care in prevention, diagnosis and treatment, and providing information and empowerment for patients. Between 2010 and 2016 the number of health care institutions providing outpatient services increased from 1127 to 4192, the number of primary care practices (GP, paediatricians, internists) went from 361 to 1275, and the number of other outpatient health care institutions grew from 75 to 729. Revised quality criteria for the evaluation of the family doctor’s annual activities were also introduced.
Starting 5 May 2024, the advisory phone number of the Center for Disease Prevention and Control will expand its services, providing telephone consultations for residents, facilitating inquiries about available addiction treatment services, and providing psychological support for residents with alcohol use disorders.
The helpline aims to provide anonymous psychological assistance, motivate and support residents in changing their habits or those of others, and offer information about available resources and services for addiction treatment.
Residents will receive counselling on quitting smoking, addressing alcohol and drug abuse problems, gambling and co-dependency issues.
The use of addictive substances is a widespread problem in Latvia. In 2023, almost a third of the population aged 18–74 used a product containing tobacco or nicotine daily. Additionally, Latvia ranks first among OECD countries in registered absolute alcohol consumption for individuals aged 15 or older. A growing trend can also be observed in drug experimentation.
Authors
In 2020 and 2021, the MoH established a working group to review the ability of hospitals to provide healthcare services corresponding to the level assigned. The review aims at ensuring a fair distribution of complex healthcare services in tertiary hospitals and the widest possible availability of basic healthcare services to citizens within the region.
A national-level implementation plan is in place, and a draft informative report has been submitted to the Cabinet of Ministers for approval and is available on the TAP (draft legislation) public portal.
Once approved, implementation will start with a review of hospital levels and health care service profiles, and improvement of the quality system. In cooperation with clinical university hospitals, the requirements, quality criteria and measurable performance indicators for the mandatory health care service profiles for each level of inpatient service will be specified, based on the Cabinet of Ministers’ regulations of August 28, 2018 No. 555 “Organization and payment procedure for health care”.
Authors
References
https://tapportals.mk.gov.lv/legal_acts?search%5Bquery%5D=22-TA-2097&quicksearch=
Ministru kabineta 2018.gada 28.augusta noteikumos Nr.555 “Veselības aprūpes organizēšanas un samaksas kārtība” 6.pielikums