-
11 August 2025 | Policy Analysis
Towards a new model of mental health care in Italy: The National Mental Health Plan 2025–2030 -
11 August 2025 | Country Update
Italy launches its National Mental Health Plan 2025–2030 -
17 July 2023 | Country Update
Mental health initiative, “Psychologist Bonus”, made permanent -
17 July 2023 | Policy Analysis
Response to the mental health crisis in Italy: the “Psychologist Bonus”
5.11. Mental health care
In 1978, with Law 180/1978 (“Legge Basaglia”), Italy was the first country in Europe to abolish psychiatric hospitals (or asylums) (around 100 were active at that time) and compulsory mental treatments on psychiatric patients, establishing the basis for a new mental health care and philosophical model (Fattore et al., 2000). The inspiring principle was that mentally ill people should have the same rights as other patients and be integrated into the community, instead of admitting them and coercively treating them in isolated facilities. Compulsory health treatment (Trattamento Sanitario Obbligatorio, TSO) became acceptable only in cases of clinical urgency or under justified circumstances, and as an exception to the constitutional principle (art. 32) that no one should be treated against their will. Psychiatric hospitals were gradually replaced by domiciliary assistance, outpatient mental health centres, hospital psychiatric wards, long-term psychiatric residential structures, and residences for the implementation of security measures (Residenza Sanitaria per l’Esecuzione delle Misure di Sicurezza, REMS), the latter dedicated to mentally ill offenders. Two different medical specializations are available in the mental health area: “psychiatry” for adult patients and “child neuropsychiatry” for paediatric patients, which also deals with neurological disorders.
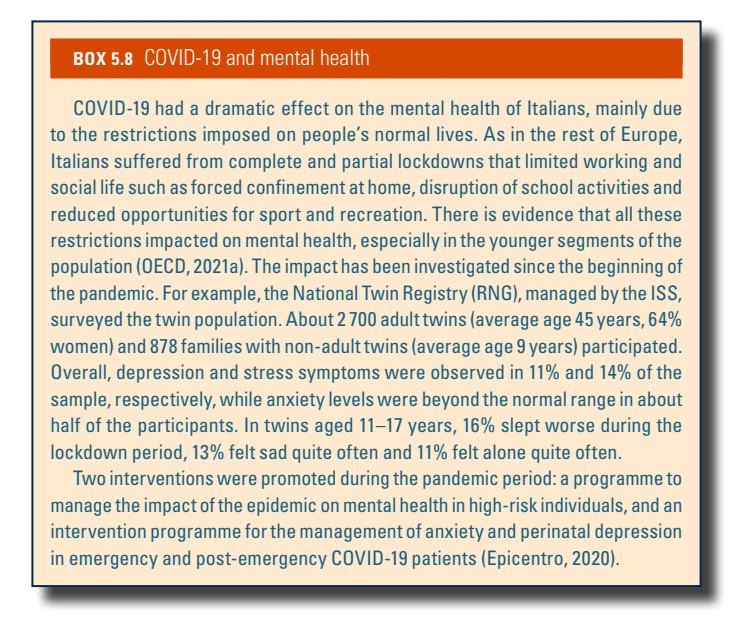
Italy’s hospitalization rate for psychiatric disorders decreased steadily from 2001 to 2018, in line with the trend for all hospitalizations, and with the objective of shifting the management of mental disorders mostly to community care. Uneven distribution of mental health care services and the lack of a standardized monitoring system account for some level of regional variability in this hospitalization rate. Further, services for individuals with addiction (Servizi per Dipendenze, SERT or SERD) are multidisciplinary outpatient services dedicated to the treatment, prevention and rehabilitation of people abusing narcotic substances (drugs or alcohol) or affected by other types of addictions (e.g. gambling, compulsive shopping, social media, food). SERT/SERD are multi-professional organizational units within local health authorities led by a clinician (often a psychiatrist). In the context of the COVID-19 pandemic, research and policy initiatives were promoted in the mental health area (Box5.8).
Box5.8
Context
Mental health is one of the main challenges for healthcare systems worldwide. In 2021, in Europe and Italy, about one in six people suffer from mental disorders, which affect not only individual health but also the socio-economic fabric. In particular, anxiety and depression are among the most common disorders in Italy. These conditions have a strong impact on the working-age population (20–64 years) and result in a number of years lived with disability almost 10 times as high as those caused by cancer. There is also great concern due to the increase of mental health problems since COVID-19 and the increase in incidence of psychological problems in the adolescent and young female population (Ministry of Health, 2024).
A further concern is the probable underdiagnosis of mental disorders in many Italian regions, as shown by marked differences in treated prevalence, which vary significantly from area to area. This disparity suggests uneven healthcare services and diagnostic capacity across the country.
The economic burden of mental health conditions is also substantial. They account for 3.3% of Italy’s GDP, with over EUR 20 billion in losses tied to reduced productivity and labour market participation (Ambrosetti, 2025).
Despite this, mental health received only 3.3% of total healthcare expenditure in 2022 – well below the European average of 5% (Ambrosetti, 2025).
The framework for mental health care in Italy still largely rests on the Basaglia reform (Law 180 of 1978), which marked a paradigm shift by closing psychiatric hospitals and promoting a community-based care model. In the following years, targeted initiatives defined by national health planning were implemented – such as the Objective Project for Mental Health Protection (1998–2000), the development of Community Mental Health Centers, and dedicated programs for early intervention in youth – and certain services were incorporated into the Essential Levels of Assistance.
However, significant regional disparities persist, along with a notable shortage of resources, staff and monitoring tools.
Main measures
The new National Mental Health Plan 2025–2030, approved by the State-Regions Conference in July 2025, is set within this context with the aim of strengthening and innovating Italy’s mental health care system. The plan promotes an integrated, multi-layered approach focused on prevention, inclusion and timely interventions.
The document is based on three key pillars:
- It adopts a bio-psycho-social model that goes beyond the traditional clinical approach by considering social, environmental and relational factors influencing mental health.
- It embraces the One Health/One Mental Health concept, aligned with WHO and European Commission guidelines, recognizing the interconnection between physical, psychological, environmental and social health.
- It places the individual at the centre, viewing them not just as a patient but as an active participant in their care, supported by families, caregivers and professionals in a collaborative and participatory manner.
The plan is structured around six key strategic areas:
- Promotion, prevention and care
- Childhood and adolescence
- Justice and security measures
- Risk management and safety
- Social and healthcare integration
- Training and research
It also introduces a four-level care model designed to provide progressive and flexible access to services. A major innovation is the introduction of the primary care psychologist within community centres, who will offer free, non-medicalized support for mild to moderate mental health issues, helping with guidance and easing the burden on specialized services. Special attention is given to severe and complex mental disorders through the introduction of a “case manager” responsible for personalizing and coordinating the therapeutic pathway, ensuring continuous support especially for marginalized individuals or those involved in the justice system.
Finally, the plan acknowledges the importance of digital technologies, such as tele-visits and teleconsultations, which are already well-established in other countries, promoting their use as a complement to traditional services. In this context, the potential of artificial intelligence to innovate medicine and mental health care is also highlighted.
The 2025–2030 National Plan lays the foundation for structural and cultural change, but a collective effort is needed to turn intentions into reality: adequate resources, trained personnel and continuous attention to local needs will be crucial to restoring dignity and rights to people living with mental distress.
References
Ministero della Salute (2025) Piano di Azione Nazionale per la Salute Mentale PANSM 2025–2030, https://www.quotidianosanita.it/allegati/allegato1752566348.pdf
Ministero della salute (2024) Rapporto salute mentale Analisi dei dati del Sistema Informativo per la Salute Mentale (SISM) Anno 2023. https://www.salute.gov.it/new/sites/default/files/imported/C_17_pubblicazioni_3502_allegato.pdf
Quotidiano sanità (2025) Dallo psicologo di primo livello all’integrazione dei servizi socio-sanitari. Ecco il nuovo Piano nazionale per la Salute Mentale 2025-2030. 15 July 2025. https://www.quotidianosanita.it/governo-e-parlamento/articolo.php?articolo_id=130940
The European House Ambrosetti (2025) Headway – A new roadmap in Brain Health in Italia: Focus Mental Health. La salute mentale come motore della crescita socio-economica dell’Italia, 4 February 2025. https://healthcare.ambrosetti.eu/it/incontri/view/14863#lg=1&slide=0
In July 2025, the State-Regions Conference approved Italy’s new National Mental Health Plan 2025–2030. The plan is structured around six key strategic areas (promotion, prevention and care; childhood and adolescence; justice and security measures; risk management and safety; social and healthcare integration; training and research).
A major innovation is the introduction of primary care psychologists within community centres to provide support for mild to moderate mental health issues and the role of “case managers” responsible for personalizing and coordinating care for severe and complex mental conditions (see the policy update “Towards a new model of mental health care in Italy: The National Plan 2025–2030”, 11 August 2025).
References
In December 2021, the Italian government introduced the “Contribution to support expenses related to psychotherapy sessions” (commonly known as the “Psychologist Bonus”). The measure, which is means tested in order for individuals to qualify, was initially designed to help people suffering from anxiety, stress, depression, and psychological fragility due to the COVID-19 pandemic and the resulting socio-economic crisis.
The measure only became operational from 25 July 2022, and funding was set to expire after 31 December 2022. However, the 2023 Budget Law has made it a permanent part of the benefits package, allocating EUR 5 million for 2023 and EUR 8 million from 2024 onwards.
See also the accompanying policy analysis dated 17 July 2023.
References
Decree Law 228/2021: https://www.gazzettaufficiale.it/eli/id/2021/12/30/21G00255/sg
Budget Law 2023: https://www.gazzettaufficiale.it/eli/id/2022/12/29/22G00211/sg
Context
Mental disorders present a significant hurdle for Italy’s National Health Service (Servizio sanitario nazionale), with the average onset age generally falling between 15 and 35, an age range that is (unfortunately) getting younger. The incidence rates have nearly doubled in recent times, including a notable surge attributed to the impact of the COVID-19 pandemic.
The latest Mental Health Report from the Ministry of Health shows a 6.9% increase in individuals seeking assistance for psychiatric issues in 2021 compared to 2020. More than half of these cases (53.6%) were women, and emergency room visits for psychiatric conditions accounted for 3.3% of total national visits. The most common conditions include depression, bipolar disorders, anxiety disorders, and schizophrenia. While personality disorders, substance abuse, and intellectual disabilities are more prevalent among men, neurotic, mood, and anxiety disorders are predominantly seen in women.
Italy has 126 Departments for Mental Health (Dipartimenti di Salute Mentale – DSM) and 1299 local mental health facilities, averaging 2.6 facilities per 100 000 inhabitants nationwide. In 2021, the total staff in public psychiatric units amounted to 29 785 individuals. Among them, medical professionals (including psychiatrists) made up 17.9% and psychologists 6.9%. The nursing staff was the largest group at 42.9%, followed by healthcare workers at 11.6%, professional educators and psychiatric rehabilitation technicians at 8.6%, and social workers at 4.1%. Part-time employees constituted 6.2% of the workforce.
The Ministry of Health’s Statistical Yearbooks (Annuari Statistici del Ministero della Salute) show an overall decrease of 506 psychologists between 2013 and 2017, with the national average declining from 9.5 psychologists per 100 000 inhabitants to 8.5. However, between 2017 and 2020, the number of psychologists working within the National Health Service stabilized, with a decrease in permanent employees and an increase in psychologists working under contractual agreements. In Family Counselling Centres (Consultori familiari), the recommended ratio of psychologists to inhabitants, as set by Law 405/1975 (which established Family Counselling Centres), is 2.38 per 100 000. However, only a few regions meet this standard.
Impetus for the policy measure
The progressive reduction of resources, both structural and non-structural, within the National Health Service, coupled with a substantial increase in the demand for mental health care, has made it increasingly challenging to provide the necessary psychological treatment pathways outlined in the national benefits package (known as the Essential Levels of Care/Livelli Essenziali di Assistenza – LEA). Additionally, the provision of mental health services is unevenly distributed, with patchwork implementation across various regions. Consequently, people are increasingly seeking assistance from the private sector due to the limited availability of these services.
Policy measure and implementation
In this context, the Italian government introduced the “Contribution to support expenses related to psychotherapy sessions” (commonly known as the “Psychologist Bonus”) in December 2021. This measure was initially designed to help people suffering from anxiety, stress, depression, and psychological fragility due to the COVID-19 pandemic and its resulting socio-economic crisis, who are eligible for psychotherapeutic treatment.
To qualify for this fund, individuals seeking help from professionals registered with Italy’s Register of Psychologists must have an ISEE (a calculation of relative household income and wealth) of less than EUR 50 000. Initially introduced with Decree Law 228/2021, this measure only became operational from 25 July 2022.
The funding was set to expire after 31 December 2022, but with the 2023 Budget Law, it has been made permanent, and the maximum amount payable to each recipient has increased from EUR 600 to EUR 1500. However, the number of beneficiaries has been reduced compared to 2022, as the total available resources have been lowered to EUR 5 million for 2023 (compared to EUR 25 million in 2022) and will be EUR 8 million from 2024 onwards.
References
Mental Health Report: Analysis of the Data from the Information System for Mental Health (SISM). Year 2021: https://www.salute.gov.it/portale/documentazione/p6_2_2_1.jsp?lingua=italiano&id=3282
Civic Report on Health 2022 (Cittadinanzattiva): https://www.quotidianosanita.it/allegati/allegato1651735626.pdf
Psychologists’ Proposals for the Revitalization of the National Health Service 2021 (National Council of the Order of Psychologists): https://www.psy.it/wp-content/uploads/2021/02/Documento-REVISIONE-SSN-E-PSICOLOGIA.pdf
The Italian Ministry of Health’s Statistical Yearbooks: https://www.salute.gov.it/portale/temi/p2_5.jsp?lingua=italiano&area=statisticheSSN&menu=annuario
Decree Law 228/2021: https://www.gazzettaufficiale.it/eli/id/2021/12/30/21G00255/sg
Budget Law 2023: https://www.gazzettaufficiale.it/eli/id/2022/12/29/22G00211/sg