-
06 October 2025 | Policy Analysis
Italy introduces new law to regulate AI in healthcare -
28 May 2025 | Policy Analysis
The new national platform for managing and monitoring waiting lists -
28 May 2025 | Country Update
The new national platform for monitoring waiting lists in Italy
4.1. Physical resources
4.1.1. Infrastructure, capital stock and investments
Infrastructure
In Italy in 2017, 51.8% of health care facilities were public, while accredited private facilities accounted for the remaining 48.2%, with a high concentration in the regions of Lazio, Lombardy, Campania and Sicily (ANAAO-ASSOMED, 2020).
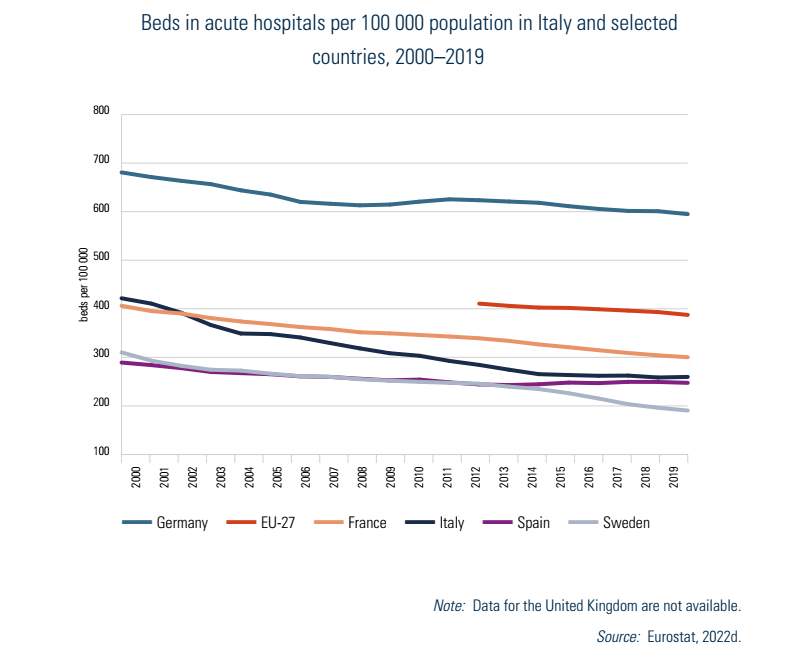
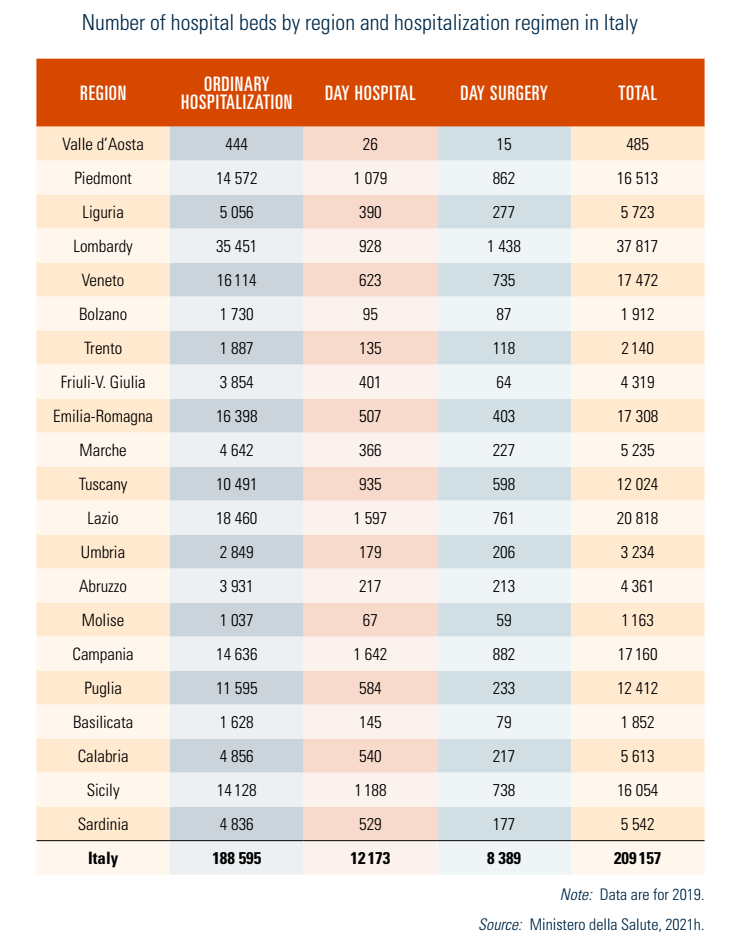
In 2019, the SSN had almost 190 000 ordinary hospital beds, 21.4% of which were in accredited private facilities. In addition to these, there were 12 173 day hospital beds, which are almost entirely public (83.8%), and 8389 day surgery beds, which are mostly public (76.2%). At the national level, 0.6 beds per 1000 inhabitants were allocated to rehabilitation and long-term care, with considerable regional variability. Following similar trends in OECD and EU countries, the number of acute beds in Italy has decreased, falling by 39% since 2000 (from 422 per 100 000 people to 260 in 2019) (Fig4.1; see also Table5.1).
| Fig4.1 | Table5.1 |
 |  |
Such numbers result from a progressive reorganization of the hospital network in response to rising financial constraints and the search for quality improvements. With Ministerial Decree 70/2015, which set targets based on “catchment areas” and regulated hospital care standards, the government entrusted regions to identify hospitals or wards to be closed and incentivized the provision of outpatient care (see Chapter 6). However these efforts to reinforce outpatient networks of care were heterogeneous among the regions. In 2020, the declining trend in hospital beds was reversed as the number of intensive care unit (ICU) beds almost doubled in a few months due to the COVID-19 emergency.
Current capital stock
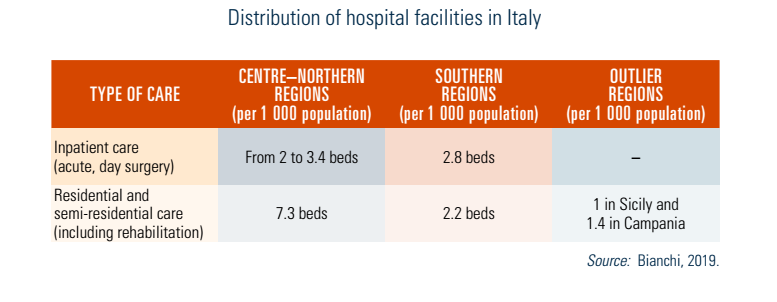
In 2019, Italy’s health care infrastructure comprised 995 hospitals, 8801 outpatient centres, 1145 rehabilitation facilities, and 16 270 residential and semi-residential establishments. Hospitals and outpatient care facilities are mostly public (51.8% and 87%, respectively) whereas establishments that provide residential, semi-residential and rehabilitation assistance are mostly private for-profit and not for-profit accredited organizations (Ministero della Salute, 2020c).
Italian hospitals have a mean age of 70 years (de Belvis et al., 2012) and their sizes are as follows: 39% of inpatient facilities have less than 120 beds and only 13% have over 600 beds, with the largest hospitals exceeding 1500 beds, mainly located in the large metropolitan areas of Rome and Milan (see Table4.1 and Box4.1). Generally, the smallest hospitals cover less than 14 specialties, whereas the largest ones cover at least 15 specialties.
| Table4.1 | Box4.1 |
 | 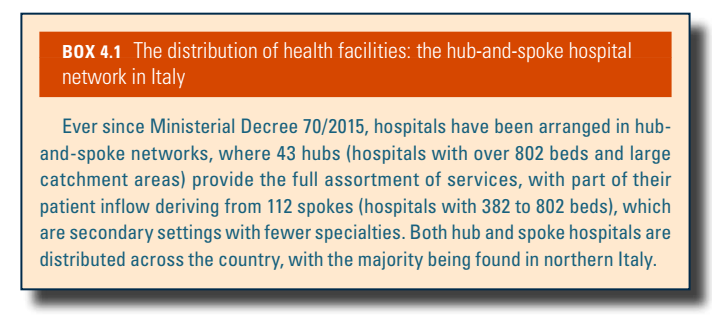 |
Local health authorities provide inpatient care through their own hospitals in most cases. The rest are autonomous hospitals that may also be connected to a university (known as polyclinics). Italian legislation also distinguishes 40 scientific and research institutes, IRCCS nominated by the Ministry of Health if they meet standards of excellence in services and biomedical research (see Chapter 2). These entities, which can include hospitals, are entitled to special public funding earmarked for research. With Ministerial Decree 70/2015, Italy’s health care facilities were reorganized to integrate services and reinforce networks as a means of enhancing appropriateness, effectiveness, efficiency, quality and safety of care (Box4.1).
Regulation of capital investment
Since 2018, a new unit within the Ministry of Health dedicated to the Evaluation and Verification of Public Investments has been responsible for evaluating compliance of capital investment with national health policies and their sustainability in relation to regional economic–financial contexts. Moreover, regional autonomy allows for other sources of funding for health infrastructures, such as using ad hoc regional funds, EU funds and self-financing through hospitals or local health authorities. Health capital spending decreased significantly from 2010 to 2019, but the 2019 Budget Law and the 2019–2021 Health Pact reversed this trend by allocating €4 billion for construction and technological modernization programmes.
Investment funding
Public capital investment funds are assigned in the annual health budget. In 2016, Italian legislators began simplifying tendering procedures to facilitate renovation and innovation initiatives. During 2020 and 2021, the necessity to respond promptly to the demands of the COVID-19 pandemic led to procurement processes (for example, for PPE, medicines, medical devices to be used in ICUs, and vaccines) being radically shortened; this experience may lead to a permanent simplification of the system. Between 2009 and 2018, the health care sector was also reliant on private–public partnerships to fund capital investment, with a slight decrease in this trend more recently.
Starting from 2021, the country’s capital investment, infrastructural modernization and digitalization funds for the health care system are being complemented by the designated NextGenerationEU budget. Reflecting stated policy priorities, the aim will be to strengthen primary and specialist outpatient services, community care and telemedicine services. Additional efforts are also being made towards the energy efficiency of public health care infrastructure with the support of EU funds, the funding under the Kyoto Protocol Convention[10] and private initiatives.
- 10. The Kyoto Protocol operationalizes the United Nations Framework Convention on Climate Change by committing industrialized countries and economies in transition to limit and reduce greenhouse gases (GHG) emissions in accordance with agreed individual targets. ↰
4.1.2. Medical equipment
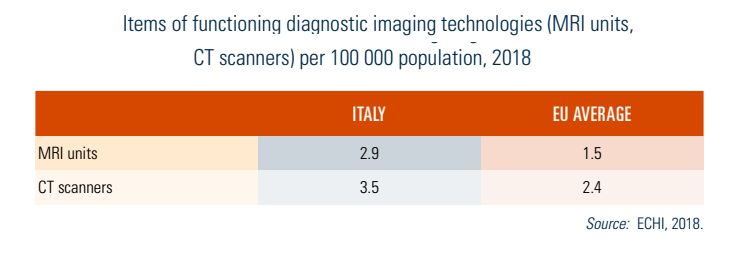
The use of technical-biomedical equipment is increasing in the public sector and Italy now ranks among the EU countries with the highest volume of MRI units, CT scanners and PET units per capita. For example, together with Cyprus and Belgium, Italy had the most imaging equipment of all EU Member States in 2018, well above the EU average (Table4.2).
Table4.2
Since 2015, the medical devices procurement process can be launched individually by facilities or via a more centralized procedure carried out by the UPCs, under regional guidelines and their decision-making support. Regions’ medical devices procurement databases feed into the Regional Observatories that send the information to UPCs to manage negotiations with facilities (see also section 2.7.5). When awarding the call for tenders, the criteria provide for the evaluation of both quantitative (price) and qualitative elements attributable to the entire life-cycle of the equipment; the most economically valid offer is prioritized. The ongoing centralization process has been shown to hasten procurement processes, especially with larger medical devices, and to contain expenditure. However, purchasing choices appear to be more focused on price considerations than on the quality of the services or clinical benefits (Vecchi et al., 2019). Since 2014, the expenditure cap for medical devices has been set at 4.4% of a region’s annual health care funding.
4.1.3. Information technology and e-Health
The NSIS is the SSN’s primary information system to support national and regional governance, health expenditure monitoring and to guarantee the uniform application of the national benefits package (LEA) (see Chapters 2 and 6). In Italy, the services that traditionally fall under this category are single appointment centres (Centri Unici di Prenotazione, CUP), which enable patients to book appointments online and by telephone; electronic health records (EHRs), electronic medical certificates, e-Prescriptions and telemedicine. Online booking and payments connected to regional platforms and EHRs are present in over 75% of facilities. Through the EHRs, citizens can trace and consult their entire health history and share it with health professionals; however, only a minority of people have heard of them. The information in each citizen’s EHR is provided and managed by the regions. It is currently active in all the regions, yet its full potential still needs to be operationalized as only 21% of the population actually use it.
The National Waiting Lists Plan 2019–2021 (Piano Nazionale Governo delle Liste di Attesa, PNGLA) requests regional CUP, which centrally manage the timetabling of appointments of all SSN facilities, to provide online services allowing people to view and cancel appointments, pay for services, print memos and also view waiting lists in real time. In addition, IT supports over 60% of health facility activities, mostly for diagnostic imaging – particularly for radiology, tests and surgical operating rooms. Digital treatments to remotely monitor adherence to therapy are mostly used for the management of chronic diseases such as diabetes and heart failure (Sanità Digitale, 2019).
In recent years, digital health spending for electronic medical records in health care facilities has been growing (by 2% in 2017 and 7% in 2018), with the largest share being sustained by facilities and regions. Until 2019, digital innovation expenditure mostly focused on the aforementioned services, with the rest funding pilot projects. With the COVID-19 outbreak, legislative changes inserted telehealth services into the list of reimbursable services, with new codes and tariffs being issued to formally integrate remote services into the SSN. Nevertheless, the pace of innovation in this area generally has been slow (Sanità Digitale, 2019). Although the number of tenders for digital innovations has been increasing since 2016, health care companies have found the process difficult, mainly due to the rigid structure of the tendering framework and complex legislation. At the EU level, the significant resources invested with the NextGenerationEU budget present an opportunity to drive the digitalization of health care processes and e-Health, with room for policy development also offered by the NRRP. The latter channels investments into the digitalization of care, further promoting the development of EHRs and telemedicine in both health care and preventive services. Box4.2 outlines some of the barriers to innovation in this area.
Box4.2

From the consumers’ point of view, access to digital services, including apps and wearables, has significantly increased despite such data seldom being communicated to doctors. While Italian citizens increasingly resort to the Internet and digital tools to find health information, the opinions of GPs are still considered to be fundamental when choosing a specialist, followed by those of relatives and friends. When it comes to information on institutional websites, online opinions and reviews are considered not to be relevant (Sanità Digitale, 2019). Since the COVID-19 pandemic (2020), use of the Internet for information on pharmaceuticals/therapy, health issues, diagnoses based on symptoms and healthy lifestyles has increased, mainly extracted from institutional websites and medical portals. Apps, blogs and social networks are used mainly for information on lifestyles and nutrition.
Context: Potential advantages and risks of AI and the Italian regulatory framework
Artificial Intelligence (AI) is reshaping healthcare by addressing systemic challenges and enhancing care delivery. Key potential benefits include improved diagnostic accuracy, reduced medical errors, increased efficiency through task automation and expanded access via telemedicine and decision-support tools. AI can also strengthen public health by enabling data-driven epidemic forecasting and policy evaluation.
However, economist Daron Acemoglu and colleagues caution that AI’s impact depends on its trajectory. If used primarily for automation (“so-so automation”), it may replace human labour without boosting productivity, leading to stagnating job growth and rising inequality. In contrast, “reinstating AI” – which complements human skills – can foster inclusive growth and better service quality.
Four major risks emerge:
- Labour substitution: AI may reduce demand for healthcare workers, especially if focused on replacing rather than augmenting tasks.
- Excessive automation: Economic incentives might drive inefficient adoption of AI, prioritizing cost-cutting over clinical improvement.
- Inequality: Automation could widen gaps between high- and low-skilled workers and between urban and rural patients.
- Skills mismatch: Rapid technological shifts may outpace training systems, leading to underuse or resistance among healthcare professionals.
To maximize AI’s potential, healthcare systems should invest in complementary innovations, equitable access and workforce development, ensuring technology enhances rather than undermines care.
In Italy, the approval of Law No. 132 of 23 September 2025 (“Provisions and Delegations to the Government on Artificial Intelligence”) represents the country’s commitment to integrating AI responsibility into the healthcare system and aligning with EU Regulation 2024/1689 (the AI Act). The law introduces measures expected to promote ethical and responsible use of AI in healthcare: a ban on discriminatory applications, protection of privacy and the right to information, and a requirement that AI support rather than replace human clinical judgment (for example, in radiology). It also establishes a national AI platform, managed by Agenas, integrated with the Electronic Health Record (Gazzetta Ufficiale, 2025).
Main measures
We report here in more detail some articles of the law:
- Article 7 establishes that AI technologies must support medical professionals in prevention, diagnosis and treatment, without replacing human clinical judgment. An example is in radiology: AI applications cannot completely replace human reading. The law also places special emphasis on people with disabilities, promoting AI systems that enhance autonomy, accessibility and social inclusion.
- Articles 8 and 9 recognize the public interest in the use of health data for research, allowing the processing of sensitive and pseudonymized data under strict safeguards, and introduce provisions for experimental AI projects under Ministry of Health oversight.
- Article 10 mandates the creation of a national AI platform, managed by Agenas, designed to support healthcare professionals with clinical guidance and provide citizens with interactive services. This platform will be integrated with the Electronic Health Record, leveraging intelligent data analysis while fully respecting GDPR and supervised by relevant authorities. However, it is likely that the implementations of these applications will take time and may be heterogeneous across territories.
References
Acemoglu, D., Autor, D., Hazell, J. & Restrepo, P. (2022). Artificial Intelligence and Jobs: Evidence from Online Vacancies. Journal of Labor Economics, 40(S1), S293–S340. https://doi.org/10.1086/718327
Acemoglu, D. & Restrepo, P. (2019). Artificial Intelligence, Automation, and Work. In A. Agrawal, J. Gans & A. Goldfarb (Eds.), The Economics of Artificial Intelligence: An Agenda (pp. 197–236). University of Chicago Press. https://www.nber.org/chapters/c14027
Acemoglu, D. & Restrepo, P. (2019). The wrong kind of AI? Artificial intelligence and the future of labour demand. Cambridge Journal of Regions, Economy and Society, 12(1), 25–35. https://doi.org/10.1093/cjres/rsz022
Gazzetta Ufficiale. (2025). Legge 23 settembre 2025, n. 132: Disposizioni e deleghe al Governo in materia di intelligenza artificiale. Available at https://www.gazzettaufficiale.it/eli/id/2025/09/25/25G00143/sg
https://www.quotidianosanita.it/governo-e-parlamento/articolo.php?articolo_id=132091
https://www.quotidianosanita.it/allegati/allegato1758293037.pdf
Context
In July 2024 Italy enacted Law 107/2024 to curb persistently long waiting times for publicly funded health services. This urgent‐measures legislation (aligned with the health component of the Recovery and Resilience Plan) mandates a new Piattaforma Nazionale delle Liste di Attesa (PNLA – National Platform for Waiting Lists), to be hosted and managed by AGENAS (the National Agency for Regional Health Services). Its stated aims are to interconnect the regional booking systems with a national portal, thereby centralizing data on waiting times and appointments. At the national level the PNLA is to provide real‐time monitoring of key metrics – such as waiting times by priority class and available appointment slots under both the public system (the National Health Service (NHS) and private accredited providers which are contracted to provide services under the NHS. By aggregating this information, the platform is intended to make system-wide trends visible: it permits a clear and detailed picture of healthcare services across all regions, supporting targeted planning.
Objectives of the PNLA
Officials emphasize four strategic objectives:
- to monitor and manage waiting lists (collecting comprehensive regional data);
- to guarantee transparency (through a national transparency portal giving citizens real-time access to wait-time indicators);
- to support decision-making (enabling administrators to plan resources based on data); and
- ultimately to reduce waiting times by improving efficiency and central coordination.
Technical infrastructure, data integrity and stakeholder access
The PNLA is designed as an advanced interoperability hub linking existing regional systems into a unified framework. According to official guidelines, it uses international data standards to ensure secure, reliable exchange with each region’s booking systems. Data flows from regional servers into a central node; each region must continuously feed the platform with up-to-date information on schedules, completed bookings and appointments. The system is explicitly non‐personalized: it does not process individual personal health data but only aggregated service metrics, in compliance with data privacy rules. To ensure integrity and trustworthiness, the PNLA incorporates strong security measures (such as encrypted data files). This transparency feature means the system can trace who viewed or changed any information, helping to prevent tampering and in compliance with GDPR requirements.
Functionally, the platform serves multiple user groups. Patients and advocacy groups will be able to view summarized, real-time indicators (for example, average wait times by service and region) via the national transparency portal. Meanwhile, health managers and policymakers (regional health directors, hospital directors general and top management, ministry officials, etc.) gain a unified dashboard of performance data, enabling them to identify bottlenecks and allocate resources where they are most needed. Official documents stress that the PNLA’s interoperability standards and data flows were chosen to integrate with regional systems, facilitating uniform data sharing and supporting service improvement.
Criticisms and challenges
Although proponents tout efficiency gains, the PNLA has drawn significant criticism from regional authorities, clinicians and consumer and patient groups. A chief concern is data integrity: critics warn that if performance metrics directly affect resource decisions or sanctions, regions might be tempted to artificially manipulate waiting lists to show better compliance. In fact, audit reports have documented manipulation in the past – for example, the Tuscany Court of Auditors found that local methods (so-called “pre-lists” and frozen lists) had altered the official waiting‐time data. Such experiences fuel fears that under a national monitoring regime, data could again be skewed, undermining trust in the platform’s accuracy.
Another key criticism is the lack of clarity on enforcement. The waiting-list law empowers the central government to intervene if regions fail to comply, but details remain vague. Regional leaders have demanded explicit rules: for instance, they have asked that clear indicators and thresholds be defined to trigger government intervention, in order to guarantee “certainty and transparency” in the process. Without such specifics, governors worry that sanctions could be applied arbitrarily.
More broadly, critics decry an overly performance-driven logic that ties outcomes strictly to sanctions or rewards. Consumer advocates (for example, the association Altroconsumo) argue that merely penalizing underperformance ignores underlying problems. They note that the government has introduced measures such as fines and even takeover of regional health authorities, but without parallel investment in staff or funding, this risks merely shifting problems onto regions that already lack resources. In their view, focusing on annual wait-time targets and punishing gaps can be counterproductive: the literature suggests that sanctions alone rarely yield lasting improvement, and may breed gaming of metrics. Thus, some experts call for a more balanced strategy (for example, combining incentives with genuine capacity-building) rather than a strict scorecard mentality. In sum, stakeholders caution that a narrow emphasis on targets and oversight – without addressing chronic underfunding and staff shortages – could distort priorities and fail to solve the real causes of long waits.
References
Ministero della Salute. Linee guida di realizzazione, funzionamento e interoperabilità della Piattaforma Nazionale Liste di Attesa (PNLA), allegato A al decreto ministeriale, January 2025.
Quotidiano Sanità. “Liste d’attesa. Approvato il decreto per la piattaforma nazionale unica: ‘Così sarà possibile il confronto fra le Regioni’”, 15 February 2025. Available at: https://www.quotidianosanita.it/governo-e-parlamento/articolo.php?articolo_id=127704
Osservatorio Conti Pubblici Italiani – Università Cattolica del Sacro Cuore. La questione aperta delle liste d’attesa, 18 January 2024. Available at: https://osservatoriocpi.unicatt.it/ocpi-pubblicazioni-la-questione-aperta-delle-liste-d-attesa
Il Sole 24 Ore. “Dal ‘salta-code’ alla piattaforma nazionale: così lo scontro con le Regioni affonda le liste d’attesa”, 26 January 2025. Available at: https://www.ilsole24ore.com/art/dal-salta-code-piattaforma-nazionale-cosi-scontro-le-regioni-affonda-liste-d-attesa-AGwbHPyD
In July 2024, Italy enacted Law 107/2024 to tackle excessive waiting times for public healthcare services. The law established the Piattaforma Nazionale delle Liste di Attesa (PNLA), a national digital platform managed by AGENAS, aimed at centralizing data from regional booking systems. The PNLA provides real-time indicators on waiting times and appointment availability across both public and accredited private providers, supporting transparency, performance monitoring and data-driven planning.
Designed as an interoperability hub, the PNLA aggregates anonymized, non-personal health data using international standards. It features strict security and traceability measures to ensure GDPR compliance. Patients can access summary indicators via a national portal, while policymakers and health managers use the platform to monitor performance and guide resource allocation.
Despite its potential, the PNLA has faced criticism. Concerns include risks of data manipulation – especially if metrics are tied to sanctions – and unclear enforcement mechanisms. Regional leaders are demanding clearer rules for state intervention. Critics also challenge the platform’s performance-driven logic, arguing that penalties without investment may worsen regional inequalities. Consumer groups advocate for a more balanced strategy that combines oversight with systemic support. While promising, the PNLA’s success will hinge on data integrity, clear governance and sustained investment in capacity-building.
For further details, please refer to the policy analysis “The new national platform for managing and monitoring waiting lists” of 28 May 2025.