-
01 February 2024 | Policy Analysis
Challenges for the Italian National Health Service in 2024. How to plan the future health workforce?
4.2. Human resources
4.2.1. Planning and registration of human resources
Since 2015, the health system has strengthened the flexibility of its health workforce capacity by allowing yearly modifications to the “three-year needs assessment plans” developed by SSN providers based on their capacity, organizational models, volumes and performance goals. However, changes are conditional on them remaining budget-neutral. There is no longer-term planning within the system.
The number of students allowed to enter the courses in Medicine and Surgery, and other health professions’ graduate programmes, is calculated nationally at the State-Regions Conference, based on an assessment of social and productivity needs and the capacity communicated by each university. The number of residency vacancies, in contrast, is determined every three years first by the regions, taking into account the employment scenario and their populations’ health needs and communicated to the Ministry of Universities and Research and to the Ministry of Health. The final number is then determined by these ministries in agreement with the Ministry of the Economy and Finance, according to the SSN’s capacity and that of the health facilities included in the training network by the National Observatory of Specialist Medical Training.
With funds from the NRRP, the number of medical specialization contracts for a full cycle of studies (five years) has increased by approximately 4200 since the academic year 2020/2021. In October 2021, the Council of Ministers approved the 2022 Budget Law, which provides for a progressive increase in the funds allocated to the contracts of doctors in specialist training. In particular, an additional expenditure of over €2 billion by 2027 is forecast.
Overall, Italy has not been able to undertake comprehensive planning for the training of health professionals, especially doctors and nurses. For doctors, the main problem is the presence of inadequate planning across specialties, in some cases due to an insufficient level of training capacity (e.g. in anaesthesiology). For GPs, where the future shortage appears to be dramatic in most regions, the main problem is that they are not trained through a university specialty programme, but rather by programmes administered by each region. These programmes are not attractive due to the quality of the curricula and the lack of interest in family medicine. The latter is probably due to the status of GPs in the SSN and, more generally, to professional arrangements that are deemed inadequate to face technological and social changes (e.g. most GPs work in solo practice with scarce IT infrastructure and medical equipment, and limited professional interactions) (Fattore et al., 2009). The shortage of nurses is difficult to justify in a country with a high unemployment rate. Here, professional status and level of compensation contribute to insufficient applications to nursing programmes. To overcome these problems, substantial changes in the distribution of tasks between doctors and nurses and better salaries are the solution. Furthermore, the resources provided through the NRRP to community care will open up more opportunities for GPs and community paediatricians to benefit from greater integration, multidisciplinarity and digitalization.
All qualified professionals are obliged to register with their professional registry in order to be licensed to practise. As provided for by EU Directive 2005/36/EC, health professionals wishing to have their title recognized in another EU country must obtain approval from the Ministry of Health.
Context
The shortage of healthcare professionals in Italy remains a major concern for the National Health Service (NHS). This shortage is a result of cost containment decisions and poor planning over the past decade.
Although the Budget Law 2024 has allocated an additional EUR 3.3 billion for contract renewals, it is important to consider long-term strategies for managing and satisfying the expectations of healthcare workers. This is crucial for ensuring the provision of quality care and the overall sustainability of the NHS.
The latest data indicates a decrease in personnel units until 2019 due to personnel expenditure ceilings set by previous budget laws and sometimes difficulties in recruiting. However, there was an increase in staff of approximately 13 000 units following the COVID-19 pandemic.
According to the OECD’s 2023 indicators, Italy has 4.1 practising doctors per 1000 population (compared to the OECD average of 3.7) and 6.2 practising nurses (compared to the OECD average of 9.2) in both the public and private sectors. It is challenging to comprehend the shortage of nurses in a country with high unemployment rates. This could be due to lower salaries and job satisfaction of Italian nurses compared to their European colleagues.
Impetus for the policy developments
Physicians and nurses have expressed their dissatisfaction with being “few, poorly paid and mistreated” and are striving to achieve decent working conditions, such as manageable workloads, adequate payment, and career advancement opportunities.
In addition, the Italian NHS faces several workforce management challenges, including the emigration of doctors and surgeons, an aging physician population, and inadequate residency training programs in certain critical medical specialties and subspecialties.
Main purpose and content
To address these issues, the central government has increased the number of specialist training contracts and available positions for medical students.
The allocation of medical residency positions is determined by Italy’s regional governments, based on employment needs. The number of medical residency vacancies is decided every three years by the regions, based on the employment scenario and the health needs of the regional population, and in accordance with funds from the National Recovery and Resilience Plan (NRRP).
The total number of specialist training contracts has increased over the last three academic years. However, there continues to be a discrepancy between job openings and qualified candidates. Recent enrolment data indicates that only about one-third of the 16 165 contracts were filled in 2023–2024. Shortages in the workforce are particularly severe in certain specialties, including Community Medicine, Pharmacology and Toxicology, Emergency Medicine, and Microbiology.
Implementation challenges
The recruitment criteria for the total number of students in Medicine and Surgery have been the subject of intense political debate and technical considerations. The national calculation of the number of students in Medicine, Surgery, and health professions’ graduate programmes is based on the teaching capacity communicated by each university at the biannual intergovernmental meetings, the State-Region Conferences.
Ministerial Decree n. 1107/2022 provides instructions on participation requirements, admission processes, rules, and the structure of the national online application exam for entry to a medical degree programme. High school graduates can take the test twice a year and are ranked based on an equalized score whereby a coefficient reflecting the deemed level of difficulty is allocated to the specific set of questions given to a candidate for their test. The allocated coefficient determines the maximum score a candidate can achieve in the test and thus impacts on their overall ranking in the admissions exam.
On 17 January 2024, the Regional Administrative Court of Lazio (TAR of Lazio) stated that the equalization methodology was flawed. This ruling does not annul the previous ranking established for the 2023/2024 test, as it only suggests directions for the selection process in the future, when it will be necessary to abolish equalized scores to ensure equal conditions among candidates.
Meanwhile, the legal battle, supported by certain politicians and lawyers, over the process of enrolling larger numbers of medical students is still under scrutiny, with the main challenges being how to overcome the hurdle of restricted access to medical degree programmes and how to protect the right of medical students to choose a desired educational programme. Medical associations are urging appropriate and timely planning, starting with forecasting epidemiological health needs and trends in healthcare demand. Apart from addressing needs, this would assist medical students in choosing an appropriate speciality and could help to guide them away from pursuing a specialization where there is an oversupply of doctors.
While the problem of expected shortages of doctors is being debated and partly addressed, nursing shortages and related policies are currently not on the political agenda; and they need to be, as Italy risks a dramatic lack of nurses in the near future.
References
Arcano R, Turati G. Osservatorio Conti Pubblici Italiani dell’Università Cattolica del Sacro Cuore. C’è un mismatch anche nel comparto socio-sanitario? 1 December 2023. Avaliable at: https://osservatoriocpi.unicatt.it/ocpi-Mismatch%20nel%20comparto%20sociosanitario.pdf.
de Belvis AG, Meregaglia M, Morsella A, Adduci A, Perilli A, Cascini F, Solipaca A, Fattore G, Ricciardi W, Maresso A, Scarpetti G. Italy: Health System Review. Health Syst Transit. 2022 Dec;24(4):1–236. PMID: 36951263.
Fassari L. Per la sanità il 2024 sarà l’anno delle riforme? Quotidiano sanità. 2022. Available at: https://www.quotidianosanita.it/studi-e-analisi/articolo.php?articolo_id=119298&fr=n.
Lazio, il Tar annulla il test di medicina. Salve le posizioni di chi ha superato le prove. Available at Rai-News: https://www.rainews.it/articoli/2024/01/lazio-il-tar-annulla-il-test-di-medicina-salve-le-posizioni-di-chi-ha-superato-le-prove-ec825532-11e2-47f3-ab46-97cec463f826.html and at Sole 24 Ore: https://ntplusdiritto.ilsole24ore.com/art/test-medicina-tar-lazio-annulla-provvedimenti-base-prove-202324-AFOaVuNC?refresh_ce=1
Ministero dell’Università e della Ricerca. Università, accesso programmato a medicina, odontoiatria e veterinaria: ecco i TOLC. 2022. Available at: https://www.mur.gov.it/it/news/mercoledi-28092022/universita-accesso-programmato-medicina-odontoiatria-e-veterinaria-ecco-i and at: Ministero dell’università e della Ricerca. https://www.mur.gov.it/sites/default/files/2022-09/Decreto%20Ministeriale%20n.%201107%20all.%202_valutazione%20delle%20prove%20e%20attribuzione%20dei%20punteggi.pdf
OECD Health at a Glance. Italy country note. Available at: https://www.oecd.org/italy/health-at-a-glance-Italy-EN.pdf.
4.2.2. Trends in the health workforce
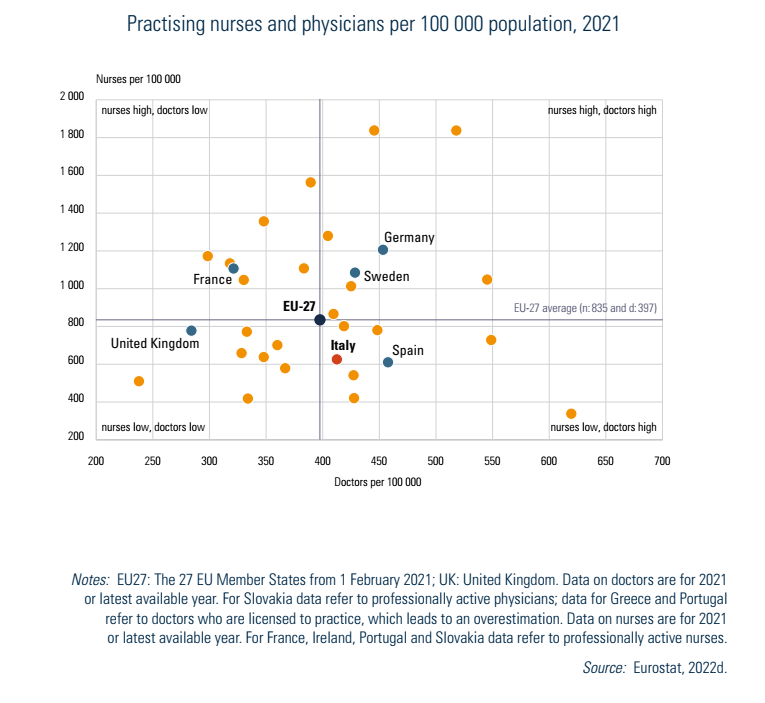
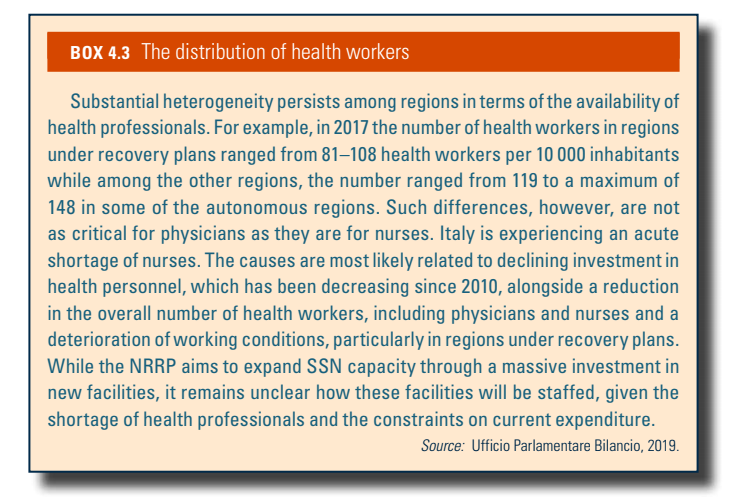
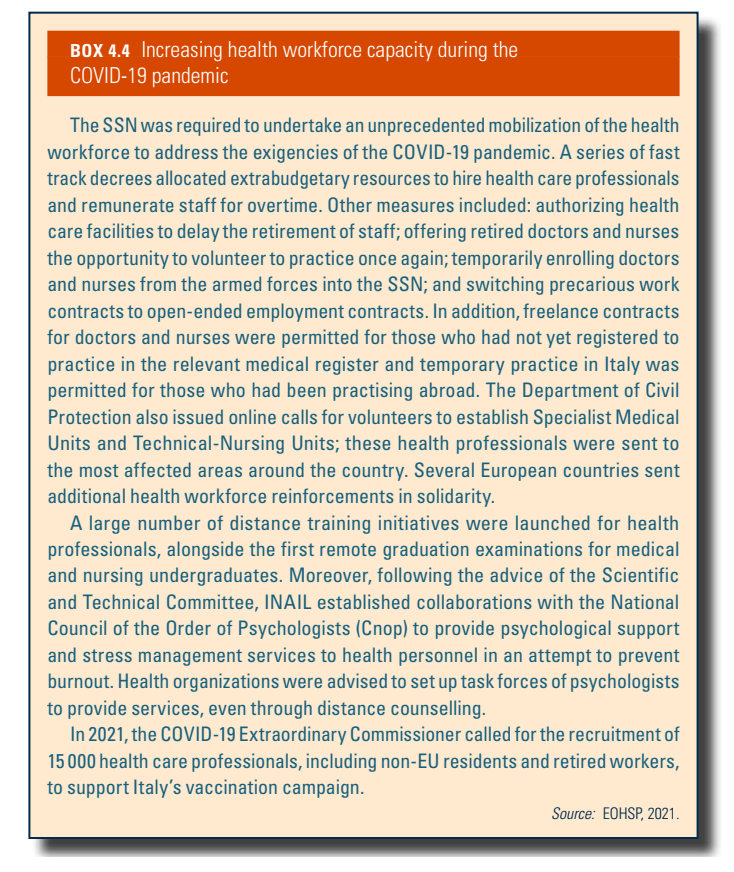
National data show that in 2018, the SSN employed over 600 000 workers (almost 50 000 less than in 2010) of which 72% were health professionals, 17.4% technicians, 10.4% in administrative roles and 0.2% engineers, lawyers, architects and other graduates (Ministero della Salute, 2020c). Generally speaking, Italy has a relatively high number of doctors but a scarcity of nurses (Fig4.2). The ratio of nurses to doctors is 2.5:1 (see also Chapter 7). The geographical distribution of health personnel is uneven, reflecting the locations of health facilities across the country and also the budgetary constraints that have been impacting the health sector (Box4.3). In 2020 and 2021, the COVID-19 pandemic necessitated measures to rapidly increase the recruitment of medical and other support staff to meet the needs of the emergency (Box4.4).
| Fig4.2 | Box4.3 |
 |  |
Box4.4
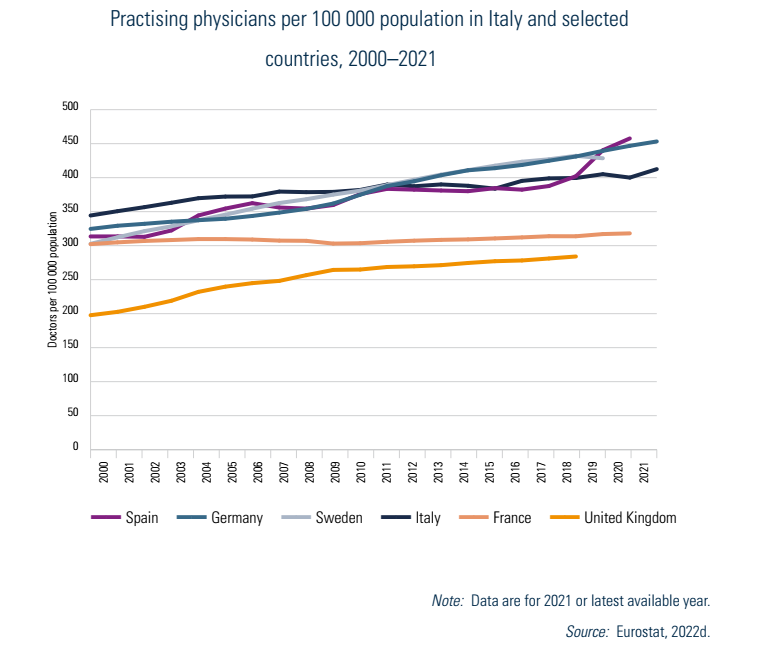
On average, Italy has a higher number of doctors than the EU average (Fig4.2). The number of practising physicians has grown steadily since the 2000s, reaching 412 per 100 000 population in 2021 (Fig4.3) which is above the EU average of 397. However, the number of public hospital physicians and GPs is now decreasing, potentially causing future shortages. It is noteworthy that more than half of the doctors working in the public system are aged over 55, which is among the highest figures in the EU. In 2019 there was a total of 42 428 GPs working in Italy (the equivalent of one for every 1409 inhabitants, compared with the EU average of 1430) and representing 17.5% of the total number of physicians (ISTAT, 2019). Alongside the crucial role they play in primary care, a major function of GPs is to be gatekeepers to higher levels of care and SSN services: they are responsible for patient referrals, and also play an essential role in ensuring continuity of care, prevention, early detection of diseases and monitoring (see Chapter 5).
Fig4.3
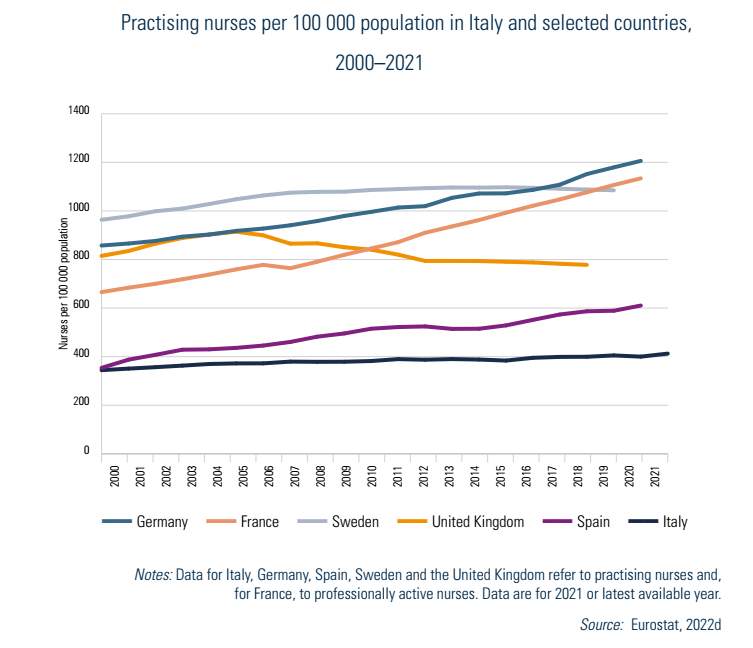
In contrast, the density of nurses per 100 000 population is among the lowest in EU Member States – 626 per 100 000 in 2021 (Fig4.4) compared with the EU average of 835 – despite the nursing profession experiencing an expansion of its tasks, especially with regard to the management of patients with chronic conditions. In 2019, there were 17 253 midwives and 367 684 nurses working in Italy (ISTAT, 2020b), placing Italy 15th in the EU ranking for the proportion of nurses and midwives in the total workforce, with a value of 1.8% (against 2.2% EU average). The number of nurses and midwives has increased by only 15 000 over the last decade, which contrasts with much larger increases in Germany and France (147 000 and 125 000, respectively) (Eurostat, 2020a).
Fig4.4
Most of the SSN’s employees are women (68%). Whereas 78% of nurses are women, female physicians constitute less than half of their category and only a minority are directors of health facilities or hospitals. Notably, however, 60% of physicians under the age of 40 are women. With women earning 24% less than men, Italy ranks eighth among the worst EU countries for overall working conditions of female health professionals and is far from achieving gender equality (Lenstore, 2020).
In terms of other health professionals, the number of practising dentists in 2021 was 86 per 100 000 inhabitants, increasing from 78 in 2013. Similarly, the number of pharmacists rose from 114 in 2013 to 124 per 100 000 inhabitants in 2021 (Eurostat, 2022d).
4.2.3. Professional mobility of health workers
In Italy, the mobility of health professionals is regulated by EU Directive 2005/36/EC. There are not many data sources at the national level that map outflows and inflows of health workers especially for those working outside hospital settings; however, existing evidence suggests that there has been an increase in outflows, especially among young practitioners.
The country is home to 77 500 qualified foreign health professionals, mostly nurses; however, only 10% of these health workers are employed by the SSN, with the remaining working in the private sector. Rigid turnover schemes, particularly in SSN facilities, that impede new hiring, accentuate the difficulty for both foreign and domestically trained foreign professionals to find stable employment.
Between 2016 and 2020, Italian doctors who requested to practise abroad (numbering more than 5000) came from regions all over the country. They were pensioners, active physicians or from cooperatives and networks of NGOs or not-for-profit associations that work in international aid. In the same period, requests from foreign doctors who wish to practise in Italy increased, alongside attempts to ease entry processes, especially in relation to rapidly addressing workforce shortages during the COVID-19 pandemic (Box4.4).
Box4.4
In 2012 (the latest data available), foreign nurses constituted 10% of the total nursing workforce and mostly worked in the northern and central regions (Fortunato et al., 2012). The majority were from eastern European countries, India, Brazil, Peru, Germany and Switzerland. Nursing shortages in Italy have contributed to high inflows, especially in care and nursing homes. The share of foreigners for less qualified health professions, such as social and health care workers (Operatori Socio-Sanitari, OSS), who provide basic personal and auxiliary care, is much larger, although not officially documented. Social care and, to a certain extent, basic nursing care are also delivered by personnel who do not have specific qualifications, often working without regular contracts in patients’ homes. The number of these workers, by definition difficult to track, is estimated to be about three times the number of nurses (Chaloff, 2008). Bilateral international agreements have been flourishing at the regional and local levels. Regions and health care providers have bilateral programmes with foreign nursing institutes, especially with eastern European partners, to guarantee the recruitment of qualified professionals (e.g. through distance learning programmes). Legislation has sought to regularize care workers’ immigration status – which also is a means of recognizing the importance of long-term care.
4.2.4. Training of health personnel
For physicians, the six-year Medicine and Surgery degree, provided primarily by public universities, consists of preclinical/basic science studies followed by clinical rotation. Graduates are effectively considered medical doctors but must enrol in the National Register to be licensed to practise. Postgraduate study and training cover 51 specialties, but until very recently have not included general practice or family medicine as a specialization.[11] Postgraduate specialization schools are supervised by the Ministry of Universities and Research and by the National Observatory of Specialist Medical Training and Regional Observatories which, in 2017, introduced accreditation standards, requirements and indicators to monitor and evaluate the quality of medical schools. Training for GPs is offered by the regional health authorities. Training lasts three years and includes internship periods in health care facilities.
To be qualified as a nurse, a three-year nursing university degree alternates compulsory in-class activities with practicums and internships. Graduates are required to pass a state examination to be enrolled in the National Registry of Nurses. As for doctors and other personnel, nurses must pass a public competition to be employed by the SSN, whereas private organizations autonomously organize recruitment. Some nurses may specialize in public health, paediatrics, mental health and psychiatry and geriatrics through two-year Master of Science programmes. The education of nurses is delivered by medical schools. Ancillary staff are generally trained through specialized courses delivered by professional schools.
Medical qualifications are mutually recognized if earned in other EU Member States, Switzerland, Norway, Iceland and Liechtenstein.
All health care professionals are required to participate in lifelong continuous medical education (CME) programmes, collecting at least 150 CME credits every three years. Such credits are awarded by course providers based on the educational activity’s level and the amount of time dedicated (e.g. participation of the health professional in meetings/congresses/seminars or conferences allows the acquisition of training credits: 0.3 credits per hour (not divisible) up to a maximum of 6 credits). Training programmes are managed by the National Commission for Continuous Training (CNFC), whereas health care professionals’ credits are overseen by the Health Professions Management Consortium (COGEAPS).
- 11. Some universities are starting to offer Family and Community Medicine as a specialization. ↰
4.2.5. Physicians’ career paths
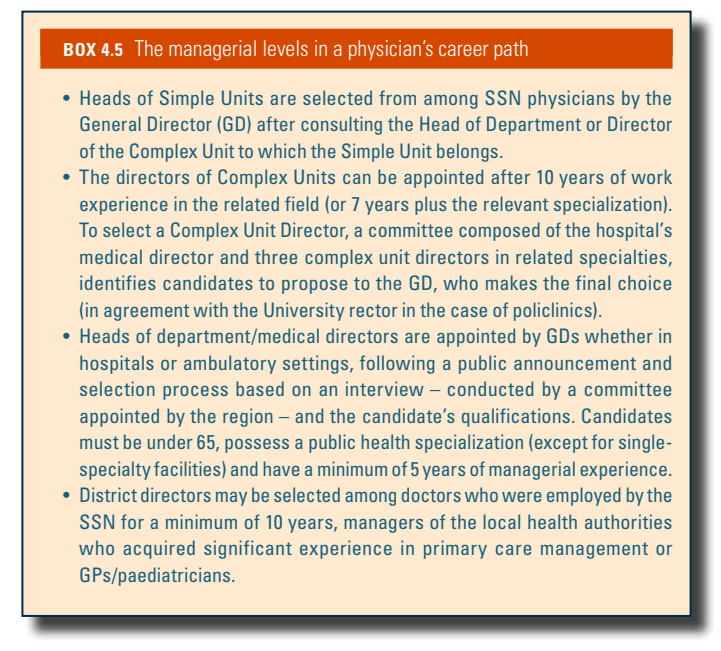
A Technical Council set up by the General Director of each health care facility evaluates health care professionals’ activities, results and participation in CME on an annual basis. A positive evaluation in training outcomes is linked to salary and determines whether physicians can maintain their positions in the health facility or hospital. Doctors employed by the SSN can be appointed to three different management positions: Head of Simple Units, Head of Complex Units, and Head of Department/Medical Directors (Box4.5).
Box4.5
4.2.6. Other health workers’ career paths
Nurses
Nurses may become experts within an area of care and be considered reference points and teachers in related training. These nurses are also assigned the most complex clinical cases. Coordinating nurses, a position gained through a public competition, manage human resources and equipment, synchronizing all functions within their department. Today, nurses are covering more managerial positions involving increasing responsibilities. Such positions are accessible after a Master’s in Management and Coordination of Health Professions and public competition.
Dentists
The main career prospects of a dentist involve specializing. Dentists can opt for managerial roles in dental practices or clinics.
Pharmacists
After a five-year degree in pharmacy or chemistry and pharmaceutical technology, pharmacists can work in hospitals or local (community) pharmacies. To be employed in community pharmacies it is necessary to follow a two-year seniority pathway, which comes with slight wage increases. Hospital pharmacists have a very slow career path and may eventually become directors of the hospital’s pharmacy.