-
21 March 2025 | Policy Analysis
National benefits package (LEA) performance and regional disparities -
10 April 2024 | Policy Analysis
AGENAS multidimensional system of performance evaluation of Hospital Trusts -
19 April 2023 | Policy Analysis
The first step in differentiated regionalism in healthcare is approved by the government -
19 April 2023 | Country Update
The Italian government approves the first step to operationalize differentiated regionalism in health care
7.1. Health system governance
In terms of the Corruption Perceptions Index, Italy ranks 42nd out of 180 (Transparency International, 2022). Accounting for 13% of corruption cases (ANAC, 2019), the health sector is known to be particularly exposed to the risk of corruption, due to the large amount of public resources at its disposal and its network of national distribution channels, with an estimated loss of €23.6 billion every year due to health expenditure waste, inefficiencies and corruption (the impact of the latter amounts to €6.4 billion) (ISPE Sanità, 2014). According to the ISPE Sanità report, the main areas involved are medicine supplies, medical equipment and cleaning services. Thus, the Ministry of Health’s three-year plans for prevention of corruption and transparency (the latest one released for 2021–2023) identify interventions aimed at preventing corruption risk factors, on the basis of the National Anticorruption Plan (Piano Nazionale Anticorruzione, PNA). According to the Plan, the main areas at risk are workforce recruitment, career progressions of health personnel, the assignment of public tenders, inspection of facilities, administrative surveillance and monitoring (Ministero della Salute, 2021k). Furthermore, the National Anticorruption Authority (Autorità Nazionale Anticorruzione, ANAC), the Ministry of Health and AGENAS have developed a monitoring system and a detailed roadmap to promote transparency in health care to reinforce the PNA. Specifically, the collaboration between AGENAS and ANAC has led to the establishment of a transparency portal, in which transparency indicators will be incorporated into the PNE which serves as one of Italy’s health system performance measurement programmes (see below) (AGENAS, 2017).
Moreover, to safeguard citizens, if citizens (even a European citizen accessing Italian health care facilities according to EU Directive 24/11) are unsatisfied with the quality and safety of the treatment received, they can file a complaint directly with the facility’s Public Relations Office (URP) and consult the Health Service Charter that each health facility is required to have (Ministero della Salute, 2019g). In addition, there are Consultative and Conciliatory Commissions (Commissioni miste conciliative) (Natangelo, 2006) and Ombudsmen at regional level (Garante per il diritto alla salute) introduced by the Gelli Law. However, these authorities have only a role in steering health care facilities with weak advocacy powers.
Some policy measures that already have been implemented, such as simplifying bureaucracy and centralizing the procurement of medical devices or public tenders, also seek to increase transparency and accountability as well as to avoid duplication of tasks and reduce waste. The main example here is the concentration of purchasing activities in regional or supra-organizational entities through the establishment of UPCs, the enlargement of several local health authorities or the establishment of a new authority, an Authorities Zero, in charge of a number of administrative tasks, including central purchasing (see Chapter 2).
Finally, the national policy agenda has become increasingly aware of the importance of performance monitoring and accountability, implementing several initiatives in these areas, including improving existing information systems and making data available to the public. Health system performance measurement strongly relies on the PNE and on the NSG (see also Chapter 2) which is complemented by quarterly monitoring and evaluation of the adequate delivery of the national benefits package (LEA).
The National Health Service in Italy (Servizio Sanitario Nazionale, SSN) is highly decentralized. The central government holds mostly a stewardship role and is responsible for defining health policy strategies, the national benefits package and the per capita budget in collaboration with the regions. The regions have legislative and executive powers, and are in charge of financing, planning, and provision of services at the local level through their Local Health Authorities, independent public hospitals and accredited private providers. Thus, an important challenge in the health system’s governance concerns the relationship between the national and regional levels of government.
Article 116 of the Italian Constitution confers the possibility to attribute particular conditions and forms of autonomy to the Italian Regions. This is known as “differentiated regionalism” or “asymmetric regionalism” and it enables Regions to enhance their powers in particular policy areas, distinguishing themselves from other Regions which may not wish to exert the same powers. While certain Regions have availed themselves of these powers in the past (see below), on 16 March 2023 the Italian government formally approved the first step, through a draft law, to more concretely operationalise and extend, in practice, the autonomy of Regions, potentially in as many as 24 matters that currently have legislative powers that are concurrent with the central government, including in areas that shape the delivery of health care across the country.
The initiatives undertaken by the Regions of Lombardy, Veneto and Emilia-Romagna in 2017 triggered a continuous political debate on the autonomy that can be achieved within various policy domains. Several innovative items in key areas concerning the health system that have already been implemented in these regions demonstrate the potential wider impact on the operation of the SSN of the draft law should it be approved:
- Increased autonomy in order to remove specific personnel-related budgetary constraints.
- Greater autonomy regarding the application for medical residency programs: scholarships’ programming and professional integration in the SSN.
- The possibility to enter into fixed-term work/training employment contracts for medical doctors, as well as to conclude agreements with universities for the work/training programs of resident doctors.
- Greater autonomy on economic functions concerning the payment system for health service tariffs, reimbursement, remuneration and co-payments (limited to residents in that Regions).
- Greater autonomy in defining governance and management of healthcare organizations, with limits on the selection of healthcare managers.
- The possibility to submit technical-scientific evaluations for the demonstration of therapeutic equivalent drugs to the Italian Medicines Agency (AIFA).
- Planning autonomy on the building stock and technological facilities of the SSN through an adequate multiannual resource plan.
- Increased legislative, administrative and organizational autonomy on additional healthcare funding.
- Greater autonomy regarding the management of SSN personnel (incentives, financial support and bargaining) and the regulation of freelance activity.
- Changes to the distribution and delivery of medicines for particular categories of patients (recurrent follow up, after hospital discharge, home care etc.) in order to ensure the continuity of care.
The abovementioned activities must be in accordance with budgetary restrictions, the current legislation concerning AIFA’s institutional functions and, above all, in accordance with guaranteeing the delivery of the nationally defined health benefits package (Livelli Essenziali di Assistenza, LEA).
The path towards more regional autonomy is still ongoing. Given the importance of guaranteeing equity in access and quality of care across the entire country, and citizens’ right to health, it is clear that the current decision-making processes connected to this new draft law are complex and very uncertain.
References
de Belvis AG, Meregaglia M, Morsella A, Adduci A, Perilli A, Cascini F, Solipaca A, Fattore G, Ricciardi W, Maresso A, Scarpetti G. Italy: Health system review. Health Systems in Transition, 2022; 24(4): pp.i–203.
Schema di disegno di legge disposizioni per l’attuazione dell’autonomia differenziata delle regioni a statuto ordinario [Text of the Draft Law on “Provisions for the implementation of the differentiated autonomy of the Regions with Ordinary statute”] approved by the Italian Government on 16 March 2023. Available at https://www.quotidianosanita.it/allegati/allegato1679045423.pdf.
Senato della Repubblica. XVIII legislatura 2018). Il regionalismo differenziato e gli accordi preliminari con le regioni Emilia-Romagna, Lombardia e Veneto. Dossier n. 16, maggio 2018. Available at: www.senato.it/service/PDF/PDFServer/BGT/01067303.pdf.
Fondazione GIMBE (2023) Il regionalismo differenziato in sanità. Bologna, Febbraio 2023. Available at: www.gimbe.org/regionalismo-differenziato-report.
On 16 March 2023 the Italian government formally approved the first step (through a draft law) to more concretely operationalise and extend, in practice, the autonomy of Regions within a range of policy matters, including in areas that shape the delivery of health care across the country. See the separate Policy Analysis dated 19 April 2023.
References
Schema di disegno di legge disposizioni per l’attuazione dell’autonomia differenziata delle regioni a statuto ordinario [Text of the Draft Law on “Provisions for the implementation of the differentiated autonomy of the Regions with Ordinary statute”] approved by the Italian Government on 16 March 2023. Available at https://www.quotidianosanita.it/allegati/allegato1679045423.pdf.
7.1.1. Monitoring and evaluating the delivery of the national benefits package
The Permanent LEA Committee, known as the National Commission for the Update of the LEAs and for the Promotion of Appropriateness of Care in the SSN, is composed of:
- four representatives of the Ministry of Health (one of whom is the coordinator);
- two representatives of the Ministry of Economy and Finance;
- one representative of the Department for Regional Affairs of the Council of Ministers; and
- seven representatives of the regions.
The Committee’s activities, technically supported by AGENAS, comprise the verification of the provision of the LEAs, their appropriateness and efficiency in the use of resources in delivering the benefits package in each region. Once the LEA Committee certifies the level of compliance of the regions, a technical evaluation board at the Ministry of Economy and Finance provides the final assessment. Such assessments then allow regions to access a premium quota of the National Health Service Budget.
The assessment is performed through the NSG, which was introduced on 1 January 2020 (Ministero della Salute, 2019h), updating the previous Guarantee System from 2000. The NSG is the tool that, with the multidimensional data available through the NSIS (see Chapter 2), evaluates the dimensions of equity, effectiveness and appropriateness of the care received by all Italian citizens through 88 indicators, including social, well-being and integrated care indicators as outlined in Table7.1.
Table7.1
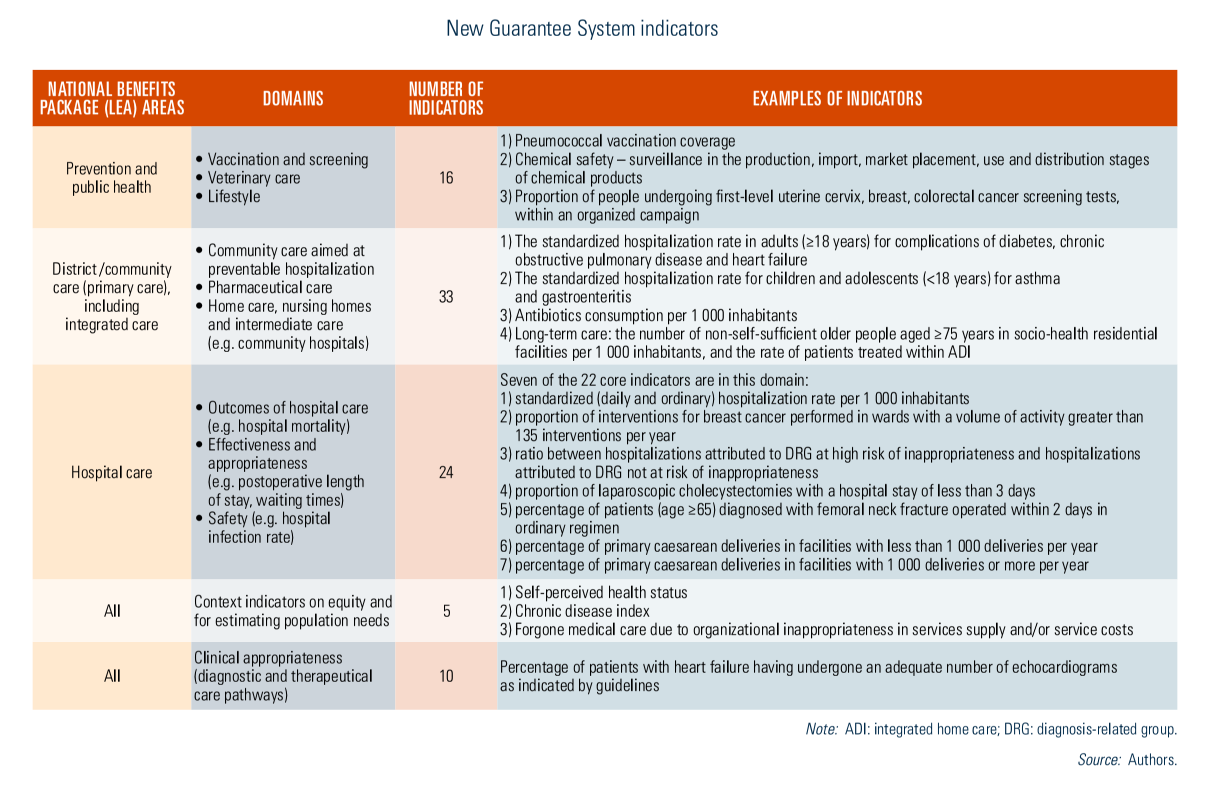
In order for regions to be compliant, each area of care, separately assessed, must score at least 60 out of 100. For underperformers, recovery plans are launched (see Chapter 3). Within each LEA it is possible to identify critical areas where performance is not meeting the required standards, time trends and, if significant, local deviations.
In the context of monitoring important areas of regional performance, since 2007, recovery plans have been used as tools to maintain a balance between regional health care expenditure and quality of services (see Chapter 3). At present, there are seven regions subject to recovery plans (Abruzzo, Calabria, Campania, Lazio, Molise, Puglia and Sicily), two of which are under the supervision of a national-level Extraordinary Commissioner (Molise and Calabria) (see Chapter 6). Such plans have been effective in decreasing regional financial deficits: now very few regions exceed budgets and deficits are modest. However, cost-containment measures have mainly been driven by reductions in workforce capacity, cuts in the number of beds and, in some cases, an increased role for private sector providers. There is also some evidence that these policies had adverse effects on health outcomes (Arcà, Principe & Van Doorslaer, 2020).
Context
The “essential levels of assistance” (LEA in Italian) define the healthcare services that the National Health Service (NHS) is required to guarantee to all citizens, ensuring equitable and uniform access across the entire country. These services are evaluated based on indicators measuring the quality and effectiveness of care across three macro-areas: hospital services, district (community, primary) care, and prevention. Indicators are based on a scale of 0 to 100, with a score of 60 corresponding to the minimum guarantee threshold (that is, “sufficiency”).
The data published at the end of February 2025 illustrate a mixed picture: while some regions show steady progress, persistent territorial inequalities and structural weaknesses in district care and prevention remain critical. These gaps not only hinder equitable access to healthcare but also increase pressure on hospital facilities, threatening the overall sustainability of the system.
Main results
The analysis of the 24 core indicators (a subsample of the total 88 indicators) reveals contrasting trends between 2019 and 2023. Hospital care shows improvement, while district care and prevention services continue to decline. Failures in these areas are classified as non-compliances, blocking access to incentive funds from the National Health Fund.
In 2023, regions such as Piedmont, Lombardy, the Autonomous Province of Trento, Veneto, Friuli–Venezia Giulia, Emilia-Romagna, Tuscany, Umbria, Marche, Lazio, Campania, Puglia and Sardinia scored above the sufficiency threshold of 60 across all macro-areas (see Figure 1). Notably, no region or autonomous province scored below the threshold in all three areas, yet several struggled in one or more sectors:
Below the threshold in two macro-areas: Valle d’Aosta (District and Hospital), Abruzzo, Calabria, Sicily (prevention and District).
Below the threshold in one macro-area: Autonomous Province of Bolzano, Liguria and Molise (prevention), Basilicata (district).

Figure 1 visually represents regional performance, emphasizing the territorial disparities and highlighting areas requiring urgent intervention. The COVID-19 pandemic underscored the fragility of local healthcare networks, yet this remains an unresolved weakness in many regions. The lack of robust prevention strategies contributes to higher incidences of avoidable diseases, exacerbating hospital overcrowding, inflating costs and worsening long-term health outcomes.
Analysis
Despite the ambitious investment of over EUR 7 billion allocated by the National Recovery and Resilience Plan (NRRP) to strengthen and reorganize primary care – with initiatives ranging from the creation of community health centres and community hospitals to the enhancement of territorial and digital healthcare – significant doubts remain about the feasibility of achieving the objectives by the June 2026 deadline. The challenges related to infrastructure implementation timelines, healthcare staff shortages, and the varying capacities of Regions to carry out reforms could undermine the overall effectiveness of the investment.
Overall, the NHS shows an improving trend in the hospital sector, while the areas of district care and prevention continue to worsen, albeit with a less “robust” trend. Particular attention should be paid to the trend in district/primary care. In fact, in 2023 the first effects of the adoption of the standards referred to in Ministerial Decree 77/2022 were expected, but did not materialize. That decree provided for the implementation of what was envisaged and financed by the NRRP for the revitalization of services, starting with community health centres, community hospitals, and integrated home care. These data, on the other hand, seem to signal a new alarm bell, indicating that the main problem of the NHS remains the fragility of district care that was exposed during the COVID-19 emergency period, especially in some districts, despite the interventions and investments put in place in recent years.
In conclusion, the LEA results provide valuable insights into regional healthcare performance, revealing both progress and persistent vulnerabilities. Strengthening district care and prevention systems is essential to balancing the system, alleviating hospital strain, and enhancing health outcomes. These results point to the need to address structural and organizational barriers, ensuring that the opportunities presented by the NRRP translate into sustainable, long-term improvements in healthcare equity and access.
7.1.2. National Outcomes Programme
The National Outcomes Programme (PNE) is a parallel system managed by AGENAS aimed at measuring the clinical performance of SSN organizations and private-accredited providers. It provides a comparison at the national, regional and provider levels by assessing effectiveness, equity, appropriateness and safety. It makes available indicators using micro-data (at patient level) and risk adjustment procedures (for example, adjusted mortality at 30 days for acute myocardial infarction, re-hospitalization rates after hip replacement and caesarean section rates) (see section 7.4).
Context and background
Performance measurement and evaluation systems are important governance tools within health care systems: they support decision-making, planning and control processes, and they stimulate and guide continuous quality improvement. Both at the international level (for example, OECD) and at the national level (for example, the National Outcomes Programme in Italy), there is a wealth of experience and approaches for developing multidimensional evaluation systems. These encompass a variety of objectives that can be measured by specific indicators.
Evaluating the performance of health services is one of the institutional tasks of AGENAS (National Agency for Regional Health Services), serving as the technical-scientific agency of the Italian National Health Service (Servizio Sanitario Nazionale, SSN). The Agency carries out research and support activities for the Minister of Health and the regions.
With the 2019 budget law (Law 30 December 2018, no. 145), AGENAS was tasked with developing a new multidisciplinary monitoring system to support the Ministry of Health, the regions and the autonomous provinces, specifically “[... A system for analysing and monitoring the performance of public Local Health Authorities and Hospital Trusts, which, by means of a specific warning mechanism, will signal, in a preventive manner, any significant deviation in the economic-management, organizational, financial and accounting, clinical-support, clinical-effectiveness and diagnostic-therapeutic process components, the quality, safety and outcome of care, as well as the equity and transparency of processes [ . . . ]”.
The new system of performance evaluation
The new system introduced by the Agency started with the evaluation of (public) Hospital Trusts from an organizational-management and economic-financial perspective, in addition to the evaluation of the quality of healthcare from a clinical-support standpoint, which is already monitored by the National Outcomes Programme. Assessing these new dimensions can help healthcare organizations improve patient safety, ensure clinical and organizational appropriateness, and reduce both errors and wasted resources.
Inspired by Donabedian’s quality measurement model, the evaluation includes three key areas of performance measurement: structure, process and outcome. While the process and outcome dimensions reflect the National Outcomes Programme summaries, the structure dimension introduces a new element of analysis. Specifically, it encompasses five performance areas: i) accessibility; ii) organizational process governance; iii) financial sustainability; iv) workforce; and v) investment. Each is further broken down into sub-areas and related indicators (Randazzo & Guerrieri, 2023).
The Agency’s monitoring model, in compliance with Legislative Decree No. 171 of 2016, also strengthens the importance of healthcare management and organization. It stipulates that public Hospital Trusts’ General Managers must be evaluated on the basis of the achievement of the health and service operation objectives set by regional planning. This new system will be essential both for the regions and their governance toolkits, enabling the evaluation of Hospital Trust management performance, and at the Hospital Trust level, for internal management purposes, facilitating monitoring the performance of its operations, identifying critical areas and areas for development, all of which feed into the continuous process of management improvement.
AGENAS has developed an easily accessible online portal to promote adoption of the monitoring model. This platform facilitates the evaluation of the performance of healthcare organizations on several levels with different “views”, over time and space. It also allows organizations to monitor their performance trends.
References
Guerrieri A, Farelli V, Paris A, Perrini MR, Randazzo MP, Cicala SD, Gioia F (2024) La valutazione della performance delle aziende sanitarie: il contesto del sistema di monitoraggio sviluppato da Agenas. 2024. Available at: https://www.agenas.it/images/2024/monitor-49/articoli-singoli/Monitor-49_9-16_Contesto.pdf
Randazzo MP, Guerrieri A (2023) Modello di valutazione multidimensionale della performance manageriale nelle Aziende Ospedaliere. Available at: https://www.sanita24.ilsole24ore.com/pdf2010/Editrice/ILSOLE24ORE/QUOTIDIANO_SANITA/Online/_Oggetti_Correlati/Documenti/2023/05/25/Agenas_performanceAziende_Ospedaliere_24_maggio_2023.pdf?uuid=AE7MBQXD
AGENAS. La valutazione delle Aziende Ospedaliero-Universitarie. Report 2019. Available at: https://www.agenas.gov.it/images/headers/1_REPORT_AOU_Agenas_2019_Completo.pdf
Legislation
(Budget) Law 30 December 2018, no. 145: https://www.senato.it/service/PDF/PDFServer/BGT/01097775.pdf