-
31 July 2025 | Policy Analysis
Initiatives to expand the medical workforce -
12 December 2024 | Country Update
Physicians’ remuneration agreement to improve working conditions and prioritize care related to armed conflict -
18 September 2023 | Policy Analysis
Shorter medical residents’ night shifts: The reform process -
18 September 2023 | Policy Analysis
Shorter medical residents’ night shifts: The reform content -
23 January 2023 | Country Update
Integrating specialist nurses into primary care clinics -
19 December 2022 | Policy Analysis
Replacing foreign medical students with domestic medical students -
13 March 2019 | Country Update
Additional positions for physician interns in hospitals -
23 October 2018 | Policy Analysis
Further expansion of the role and responsibilities of specialist nurses in the community -
01 February 2018 | Country Update
Expanding the role of specialist nurses in the community -
25 July 2016 | Policy Analysis
The full-timer initiative: additional hours and only public sector work
4.2. Human resources
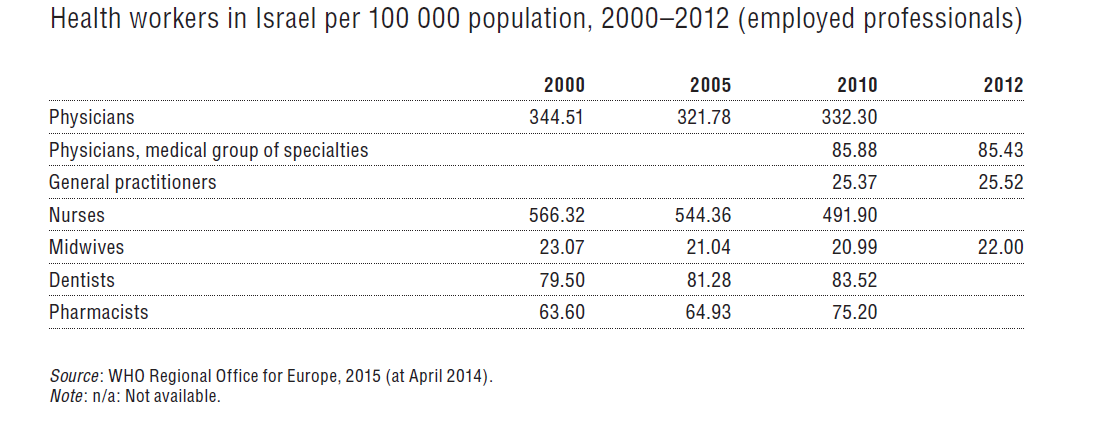
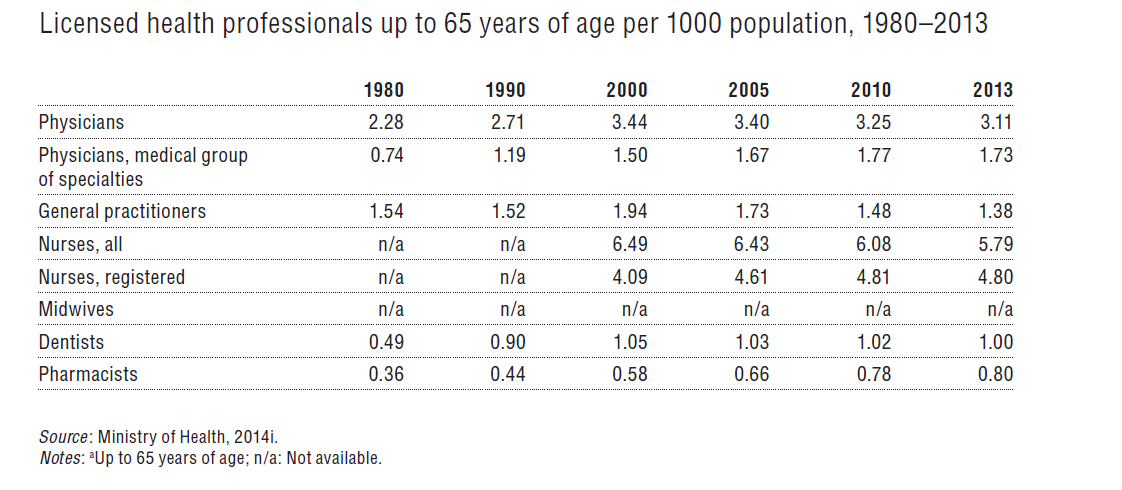
This section presents trend and comparative data for a variety of health professions. The trend data rely primarily on Israeli sources, which relate to licensed professionals up to age 65 (as in Table4.4), while the comparative data rely primarily on Health for All database (WHO Regional Office for Europe, 2015) regarding employed professionals (as in Table4.3). Naturally, there are differences between these two variables, as not all licensed professionals under age 65 are employed, and some licensed professionals continue to work beyond age 65.
Table4.4

Table4.3

Context
Projections indicate a shortage of physicians in Israel in the coming years. The density of physicians in Israel in 2022 was 371 per 100 000 population, lower than in most EU countries (Waitzberg, 2025). Around 47% of physicians were aged 55 years or more in 2021, and will reach retirement age soon. In addition, the ongoing armed conflict since 2023 continues to strain the system, disrupting medical education and increasing demand for healthcare (MoH, 2025).
Israel’s healthcare system has over-relied on foreign-trained doctors. In 2024, only 28% of newly licensed physicians were trained in Israel. There have been concerns about the quality of medical education abroad and from 2026, physicians trained in select countries will no longer be allowed to practice in Israel. This is expected to substantially reduce the influx of physicians into the system.
In 2023, the MoH appointed a committee to plan and reform the medical workforce. The committee published its recommendations to expand the cadre of physicians in 2024. The recommendations have been sequentially implemented from September 2024.
Impetus for the reform
The reform was driven by several converging factors:
- A growing dependence on foreign-trained doctors, especially from institutions that will not be recognized from 2026.
- Geographic disparities in physician distribution, with underserved regions relying heavily on lower-quality medical personnel.
- The war’s impact on medical training and service delivery.
- Recommendations from two national committees (2021–2022) calling for a significant expansion of domestic medical education.
Main purpose of the reform
The reform seeks to:
- Increase the number of physicians trained in Israel.
- Improve the quality and regulation of medical education.
- Reduce reliance on physicians that have attended unrecognized foreign medical schools, and attract more immigrant physicians from recognized institutions.
- Strengthen healthcare provision in underserved regions.
Content and characteristics
The reform includes several key components:
- Establishing three new medical schools, following decisions of the Council for Higher Education, set to open in February 2025, October 2025 and an unconfirmed future data.
- A national initiative to recruit immigrant physicians through regulatory easing, bridging courses, personal support, and employer incentives.
- Research grants and fellowships for medical residents working and living in underserved regions.
- Training physicians as future health managers in underserved regions. Providing courses on management and leadership with a focus on local epidemiology and medical needs, engagement with local communities and other health stakeholders (for example, health plans).
- In planning: subsidized loans and incentives for Israeli students studying at approved foreign medical schools, including partial loan forgiveness for returning to Israel and working in high-need areas such as geriatrics. Total loan forgiveness for physicians that work and live in underserved regions.
Impact
The number of new medical licenses issued in 2024 stood at 2 637, a 7% increase from 2023 and 48% from 2020. The full impact of the reforms is expected to materialize from 2026 onward, particularly in reducing reliance on unrecognized foreign institutions and improving geographic distribution of physicians.
Authors
References
Ministry of Health (Israel). New Doctors and Ministry Policy – 2024 Summary. Strategic and Financial Planning Division, Human Resources Planning Department. Published May 20, 2025. Available at: https://www.gov.il/he/pages/new-doctors-2024 הרופאות והרופאים החדשים ומדיניות המשרד סיכום 2024
Waitzberg R (2025). Health Systems in Action (HSiA) Insights – Israel, 2024. Copenhagen: European Observatory on Health Systems and Policies, WHO Regional Office for Europe. Licence: CC BY-NC-SA 3.0 IGO
Context
Israeli medical residents complete regular overnight shifts during their residency, which seamlessly follow their daytime responsibilities (of eight hours), totalling 26 hours of continuous work. Israel has recently implemented several initiatives to improve the working conditions of medical residents (Breuer, Waitzberg, Breuer, et al. 2023).
Impetus for the reform
In 2020, residents’ working conditions were expected to be included in the salary negotiations between the Ministry of Health (MOH) and the Israeli Medical Association (IMA). However, this agreement was put on hold by the COVID-19 pandemic. Projections of medical workforce shortages (Lafortune, Dedet, Balestat, et al., 2023) and the difficult working conditions during the pandemic subsequently sparked a sizable wave of protests by residents advocating for shorter overnight shifts. This promoted the issue of residents’ working hours to the public policy discourse and the policy agenda.
Content/characteristics
In 2021, the Minister of Economy issued an amendment to the law that reduced overnight shifts to a maximum of 18 consecutive working hours, thereby revoking the previous exemption that allowed residents to work for up to 26 continuous hours (Isbruch, 2021). Please see “Shorter Medical Residents’ Night Shifts: The Reform Content” for more details on the reform content.
This decision faced opposition from various parties: the Ministry of Finance (MoF) expressed concerns on the financial aspects of this reform; it was unclear who would bear the costs of additional staff positions to compensate for the reduced worked hours. Resident representatives raised concerns that reduced overnight working hours would lower salaries, which heavily depend on night shifts. The IMA voiced concerns that the reduced training hours could negatively affect medical education. Hospitals were worried about their ability to manage the workload and maintaining quality of care considering that many hospitals were already understaffed.
In response to this, the MoH established an expert committee to assess resident work schedules and overnight shifts in hospitals. The committee’s objectives were to find ways to reduce the duration of medical residents’ shifts, while evaluating different work schedules across various hospital departments, recognizing that various hospital departments such as surgery, internal medicine, and emergency, have distinct requirements and limitations. The committee proposed several recommendations to enhance residents’ quality of life and alleviate burnout. These suggestions included changing the skill-mix and adding physician assistants and medical secretaries (Ministry of Health, 2022).
Implementation steps taken
The proposed legal amendment to shorten resident working hours was taken to court, where it underwent an extensive year-and-a-half-long deliberation. The deliberation involved the Health Plan responsible for peripheral hospitals where the reform was due to be piloted, as well as the MoF, MoH, Ministry of Economy and Industry, and the IMA.
In March 2023, the MoH, MoF and IMA reached an agreement to implement the reform, adopting most of the recommendations put forth by the MoH’s committee. Shortened residents’ working hours are being piloted since September 2023.
Authors
References
Breuer, R. M., Waitzberg, R., Breuer, A., Cram, P., Bryndova, L., Williams, G. A., Kasekamp, K., Keskimaki, L., Tynkkynen, L. K., van Ginneken, V., Kovács, E., Burke, S., McGlacken-Byrne, D., Norton, C., Whiston, B., Behmane, D., Grike, I., Batenburg, R., Albreht, T., Pribakovic, R., Bernal-Delgado, E., Estupiñan-Romero, F., Angulo-Pueyo, E., Rose, A. J. 2023. Work like a doc: A comparison of regulations on residents’ working hours in 14 high-income countries. Health Policy 130, 104753.
Isbruch, D. 2021. 18-hour shift in 10 hospitals, and one pressure lever: Questions and answers about shortening shifts for interns. Retrieved from Davar: https://www.davar1.co.il/337870 (in Hebrew).
Lafortune, G., Dedet, G., Balestat, G., Gellie, V., Turatto, F., and Dagistan, E. 2023. OECD report on medical education and training in Israel. Paris. Retrieved from OECD: https://www.oecd.org/health/OECD-report-on-medical-education-and-training-in-Israel.pdf.
Ministry of Health. 2022. The interim report for the implementation of the outline for shortening shifts was submitted to the Minister of Health. Retrieved from gov.il: https://www.gov.il/he/departments/news/23032022-02 (in Hebrew).
Context
Israeli medical residents complete regular overnight shifts during their residency, which seamlessly follow their daytime responsibilities (of eight hours), totalling 26 hours of continuous work. Israel has recently implemented several initiatives to improve the working conditions of medical residents (Breuer, Waitzberg, Breuer, et al., 2023).
Resident night shift hours were shortened from a maximum of 36 hours to a maximum of 26 hours in the 90s and last changed in 2012, when they were limited to eight night shifts a month. The working hours are limited to a maximum of 71.5 hours per week, which is a deviation from the Israeli labour law, which currently restricts work hours to a maximum of 42 hours per week (Ministry of Economy, 2015). Nevertheless, approximately one-third of residents still report working 71.5 hours or more on average each week.
Reducing residents’ working hours is difficult without a concurrent increase in the workforce; this change may potentially harm the quality of care, elevate workloads during shifts, jeopardize the continuity of patient care and have potential adverse impact on the education and training of residents (Breuer, Waitzberg, Breuer, et al. 2023).
Impetus for the reform
The Ministry of Health (MoH) established a joint professional committee for planning this reform and finding ways how to implement a reform to shorten residents’ working hours. The committee published its recommendations in March 2022 and in March 2023, the parties (MoH, MoF, IMA) reached a consensus on how to implement the reform, adopting most of the recommendations put forth by the MoH’s committee. Please see “Shorter Medical Residents’ Night Shifts: The Reform Process” for more details on the reform process.
Content/characteristics
Hospital residents’ working hours per night shift were reduced from 26 hours to a maximum of 21 hours. Working hours on the day of an overnight shift will begin at 13:00 (instead of at 8:00) and finish at 8:00 or 10:00 on the following morning. Residents who want to maintain the same salary will be able to add four-hour evening shifts (16:00–20:00), which pay three times as much per hour than a regular shift, to their working day.
As part of the reform, 180 staff positions were added to compensate for the reduced working hours. The calculation was based on an estimated additional 1.3–1.4 staff positions for each resident (Ministry of Health, 2022) (Knesset, 2023a). An additional budget of 30 million NIS was allocated from the government budget to hospitals for this reform, which will enable hospitals to add more staff positions (Knesset, 2023b).
Implementation steps taken
This change will initially be implemented in ten peripheral hospitals located in the North and South regions of Israel, during weekdays only. It is worth noting that some medical specialities, particularly surgical, are not included in the first implementation phase. The expansion of this reform to other hospitals, weekends or specialities remains uncertain at this stage.
Authors
References
Breuer, R. M., Waitzberg, R., Breuer, A., Cram, P., Bryndova, L., Williams, G. A., Kasekamp, K., Keskimaki, L., Tynkkynen, L. K., van Ginneken, V., Kovács, E., Burke, S., McGlacken-Byrne, D., Norton, C., Whiston, B., Behmane, D., Grike, I., Batenburg, R., Albreht, T., Pribakovic, R., Bernal-Delgado, E., Estupiñan-Romero, F., Angulo-Pueyo, E., Rose, A. J. 2023. Work like a doc: A comparison of regulations on residents’ working hours in 14 high-income countries. Health policy 130, 104753.
Knesset. 2023a (30 May). The special committee for youth affairs (in Hebrew).
Knesset. 2023b (15 March). The special committee for youth affairs (in Hebrew).
Ministry of Economy. 2015. Notice of amendment of the general permit for employment during the weekends and overtime in medical institutions and care homes for the elderly or children (temporary instruction) (in Hebrew). Available at: https://rfa.justice.gov.il/SearchPredefinedApi/Documents/GNvGUMFalf63ZGWys4mgsVugQkWsuLu7GsVIrttqgCk=. Accessed 20220812.
Ministry
of Health. 2022. The interim report for the implementation of the
outline for shortening shifts was submitted to the Minister of Health.
Retrieved from gov.il: https://www.gov.il/he/departments/news/23032022-02 (in Hebrew).
What: After a few years of planning (Analysis: Further expansion of the role and responsibilities of specialist nurses in the community (2019 update), Update: Expanding the role of specialist nurses in the community, Analysis: Further expansion of the role and responsibilities of specialist nurses in the community), 10 specialist nurses (SNs) will finally join primary care clinics starting January 2023. They will work alongside and under the guidance of GPs and carry out tasks previously completed by doctors. SNs will not be able to diagnose patients, but will be able to write referrals for tests, consult medical specialties and welfare services and renew prescriptions. In addition, they will be able to manage chronic patients including their assessment, monitoring and treatment.
Why: Israel has a low rate of physicians per population compared to the OECD average (3.3 and 3.7 per 1 000 population, respectively in 2019), particularly of GPs (0.29 per 1 000). The Ministry of Health has created new roles such as physician assistants and SNs to shift tasks and relieve pressure on physicians.
How: Since the creation of SNs in 2013, 550 nurses have trained as SNs in 10 fields: geriatrics, surgery, diabetes, premature infants, rehabilitation, emergency medicine, wounds, pain, policy and management, and end-of-life care. Nurses that wish to become primary care SNs need to complete an additional year of theoretical and practical university training.
Authors
References
Isbruch, D. (2022, 12 22). The nurses who will prescribe medications and referrals: 10 community clinics will receive the first specialist nurses. Retrieved from davar: https://www.davar1.co.il/412879
Ministry of Health. (2019, 08 07). Director General’s Circular 7/2019: Nurse Practitioner in the community. Retrieved from https://www.gov.il/BlobFolder/policy/mk07-2019/he/files_circulars_mk_MK07_2019.pdf
What: Medical degree programs for foreign students will discontinue as of October 2023 and will be replaced by domestic medical school places.
Why: Israel has a low rate
of physicians per population compared with the OECD average (3.3 and
3.7 per 1000 population, respectively in 2019). Of these, 25% are aged
67+, and 40% are aged 45–66 and are due to reach retirement age soon
Currently, there are three international medical degree programs for overseas students. Overseas students mainly come from the USA, and most international students return to their home country upon graduation. At the same time, most Israelis study medicine abroad, as there are limited spots at Israeli medical schools.
In addition, a 2019 reform of the Ministry of Health (MOH) limits the recognition of foreign medical degrees
How: The council for higher education has created a plan to increase the number of domestic medical students in Israel to respond to the anticipated workforce challenges. As of October 2023, universities in Israel will cease to operate medical degree programs for foreign students. The change is expected to increase the number of domestic medical students by 130. The additional students will raise the total number of domestic medical students to 1000 a year.
The international medical degree programs have been a source of revenue for universities, as study fees for foreign students are substantially higher than those for Israeli students. Therefore, to compensate the universities for the relative loss and to incentivize them to accept more Israeli students, the government will be providing 30 million NIS for this plan.
Another bottleneck in the medical training process
is the limited number of hospital departments that can train residents.
The MOH is planning another reform to enlarge resident training
capacity. The plan is to transfer part of the residents’ training to
community settings, specifically for residents in gynecology,
pediatrics, and geriatrics
Authors
References
Council for Higher Education. (2022, 8 5). A revolution in the medical studies system in Israel – starting from the 2023-2024 school year – an addition of 130 medical students. Retrieved from CHE: https://che.org.il/%D7%9E%D7%94%D7%A4%D7%9B%D7%94-%D7%91%D7%9E%D7%A2%D7%A8%D7%9A-%D7%9C%D7%99%D7%9E%D7%95%D7%93%D7%99-%D7%94%D7%A8%D7%A4%D7%95%D7%90%D7%94-%D7%91%D7%99%D7%A9%D7%A8%D7%90%D7%9C-%D7%94%D7%97
Cramer, P. (2022, 8 23). Israel to close medical schools for foreign students. Retrieved from Jewish Standard: https://jewishstandard.timesofisrael.com/israel-to-close-medical-schools-for-foreign-students
Haklay, T., Cohen, R., Kreger, C., Gordon, S., Goldberger, N., Goldberg, S., . . . Pertez, G. (2021). Personnel in the health professions. Jerusalem: the Ministry of Health (in Hebrew)
Mendelovich, S., Belinsky, A., Angel, Y., Maoz, S., & Tzuker, I. (2022, 03 22). The interim report for the implementation of the outline for shortening shifts. Retrieved from gov.il: https://www.gov.il/he/departments/publications/reports/shifts-reduction-joint-team-intermediate-conclusions-report (in Hebrew)
Yatziv, S. (2019, 1 21). The Ministry of Health regulates medical studies abroad. Retrieved from Ministry of Health Israel: https://www.health.gov.il/NewsAndEvents/SpokemanMesseges/Documents/21012019_3.pdf (in Hebrew)
In December 2018, the Ministry of Health and Finance opened 150 new
positions for interns in non-profit hospitals. The ministries determined
the clinical fields in which these positions were allocated giving
preference to fields with physician shortages, such as Pediatric
Hematology-oncology, Emergency Care, Oncology, Rehabilitation and
Radiotherapy. The ministries also gave preference to hospitals in the
periphery, where shortages are greater. The next step will be to add
positions for interns in geriatrics and in primary community care.
This
measure intends to tackle physician shortages, particularly in
underserved clinical fields as well as the periphery. The drawback is
that it does not provide hospitals with enough flexibility to manage and
plan their resources, which is sometimes needed to serve their local or
specific needs.
Authors
References
MoH (2018) 150 new positions for interns were allocated to hospitals (in Hebrew):
https://www.health.gov.il/NewsAndEvents/SpokemanMesseges/Pages/25122018_3.aspx
In May 2018, the MoH further expanded the role, responsibilities and autonomy of nurses in the community with incremental implementation. The objectives of these changes are to empower nurses, attract more people to the profession (as there is a shortage), improve continuity of care, and reduce work pressure on physicians.
The new responsibilities for specialist nurses include: ordering various diagnostic exams, referring patients to specialist care, performing additional clinical procedures, changing medication dosage, and becoming case managers for patients. In addition, three new specialization courses will be launched to enable nurses to provide enhanced care for specific types of patients:
1. From early 2019, nurses who undertake a “stroke course” can perform additional clinical procedures in order to shorten the time of treatment for stroke patients in an attempt to deter brain damage and improve treatment outcomes.
2. In 2019, nurses who undergo “rehabilitation training” will have extended responsibilities for making decisions about, and providing, rehabilitation and medical long-term care. This change will potentially better meet the needs of the ageing population, characterized by widespread chronic conditions and disabilities in activities of daily life.
3. Beginning in early 2020, nurses who undertake a “gastroenterology course” will be able to provide more care for patients with gastroenterological conditions, either chronic or acute. The objective if this change is to improve continuity of care between inpatient and outpatient care, and better integrate care for these patients.
Authors
References
The MoH has extended the responsibilities and scope of practice for
specialist nurses in the community in order to relieve some of the
pressure on primary care physicians. The newly-recognized competencies
are in four main areas of activity:
- treating mild, acute diseases and cases that are urgent but simple to treat;
- treating and monitoring patients with chronic diseases;
- preventative care and health promotion; and
- granting health certificates and representing patients before statutory authorities.
Additionally,
specialist nurses can now prescribe medications and contraceptives.
They can also provide palliative care and refer patients to diagnostic
tests, specialists, and emergency departments.
Although this policy change has the potential to improve primary care in the community, a further challenge is the low number of nurses per population. Israel has one of the lowest rates of nurses among OECD countries (at 4.9 per 1,000 population compared to the OECD average of 9 in 2015).
Authors
References
MoH (2018) Circular "Specialists Nurses in the Community", 136/17 (in Hebrew) (https://www.health.gov.il/hozer/ND136_2017.pdf, accessed 1 February 2018)
OECD (2018) Key health indicators. (http://www.oecd.org)
In mid-2016, the MOH launched an initiative in which voluntarily selected physicians in public (i.e. governmental and non-profit) hospitals will receive significantly enhanced pay in return for: a) working additional hours in a public hospital and b) agreeing not to work in the private sector.
In the years preceding the initiative, Israel's for-profit hospitals had grown significantly, particularly in the surgical area. Between 2007 and 2011, the number of elective operations increased by 58% in the for-profit hospitals, compared with an increase of only 4% in the public hospitals; with 38% of elective procedures carried out in for-profit hospitals in 2013. By 2014, 23% of hospitalizations and 60% of operations involved private financing.
The shift in volume from public to for-profit hospitals raised a number of concerns including: a two-class system of care; loss of revenue for public hospitals; many senior physicians undertaking private work in for-profit hospitals in the late afternoons and evenings, raising concerns about quality of care at those times; and longer waiting times for elective operations in public hospitals.
The overall objective of the full-timer initiative is to strengthen Israel's publicly financed health care system by improving its availability, quality and safety. Specific objectives are to:
- increase the availability of senior physicians in public hospitals outside of regular work hours thus improving quality and safety of care
- improve the image of the publicly financed system and related public trust
- increase the volume of care provided by public hospitals
- reduce waiting times for elective operations and ambulatory treatments
- contribute to the development of the next generation of clinical leaders in public hospitals, and develop physicians who look to the publicly financed system as a sole and satisfying source of income.
To finance the initiative, the government has allocated 30 million shekels in 2016, 60 million (2017), 75 million (2018) and 85 million (2019) (€7M, €14M, €17.6, €20M, respectively). In addition, up to 80 million shekels (€19M) per year will be allocated to the initiative via the "reducing waiting time project". All Israeli public hospitals are eligible to participate, and it appears that all will join.
After a preliminary pilot phase, the MOH will determine how the funds will be divided and individual hospitals will develop a plan for how they will use the money allocated to them, including the mix of newly-certified specialists (centre of the country) and more established specialists (in the periphery) to be included, the distribution of full-timer positions across departments, etc. Individual hospitals will also need to specify expectations of increased output, at the level of both the individual full-timer and their department.
Authors
4.2.1. Health workforce trends
Table4.3 and Table4.4 summarize the changes in the health worker-to-population ratios since the 1980s.
| Table4.3 | Table4.4 |
 |  |
Physicians
The physician-to-population ratio has been relatively stable during the 1990s at 3.6–3.7 physicians up to age 65 per 1000 population, followed by a gradual decline to 3.3 per 1000 in 2012 (Fig4.4). This is in contrast to major changes that took place in this ratio during the previous decades and the changes being projected for the years ahead. There is substantial variation in the practising physicians-to-population ratio across regions; it ranges from 2.2 per 1000 in the north of the country to 4.4 in Tel Aviv.
Fig4.4
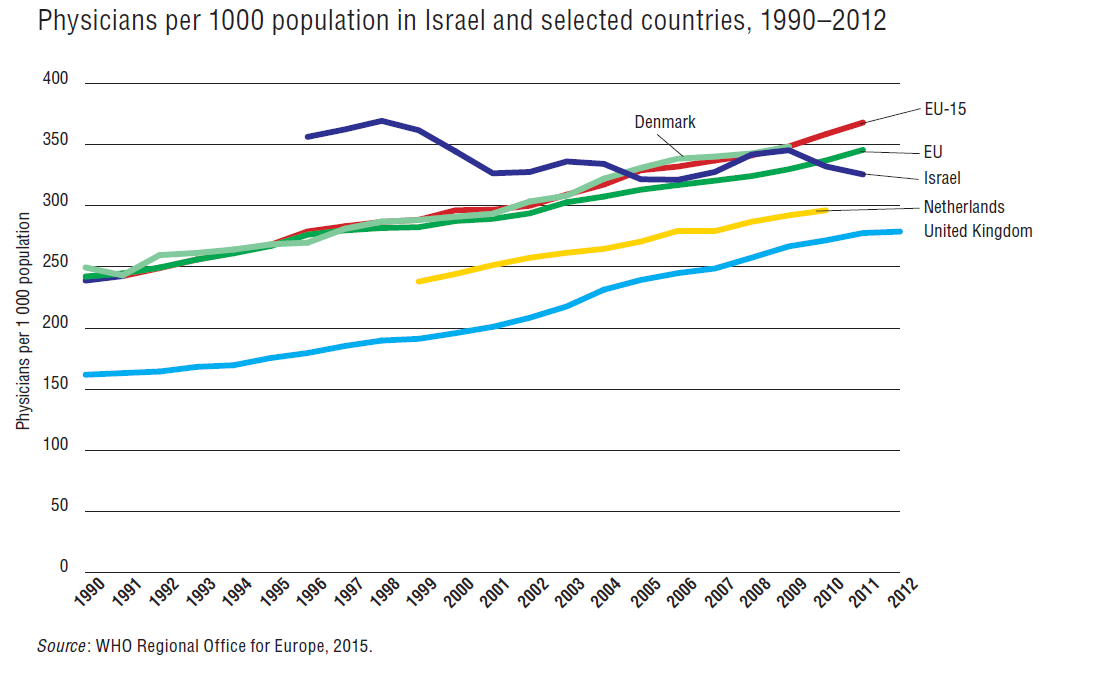
Until recently, Israel had one of the highest physician-to-population ratios in the world; even in 2006, it was still approximately 20% higher than the OECD average. After 2006, while the ratio continued to decline in Israel, it continued to increase in most OECD countries. By 2012, Israel’s rate (3.30) and the OECD average (3.25) had essentially converged. When compared with EU15 countries the physician-to-population ratio is somewhat low (Fig4.5); it has been trending downward in Israel, while it has been increasing among EU15 countries. Recently, Israel has taken several concrete steps to expand the overall supply of physicians and to channel more physicians into peripheral regions and distressed specialties (see section 6.1.4). In 2014, the number of newly licensed physicians reached a record high, and Israel’s rate has not fallen below the OECD average.
Fig4.5
With regards to specialist numbers, a Ministry of Health-appointed committee of experts found severe shortages of physicians in 2010 in the following specialties: anaesthesiology and critical care, neonatal care, child psychiatry, child development/neurology, geriatrics and physical/rehabilitation medicine. It also projected future shortages in the following specialties: pathology, internal medicine, family medicine and general surgery.
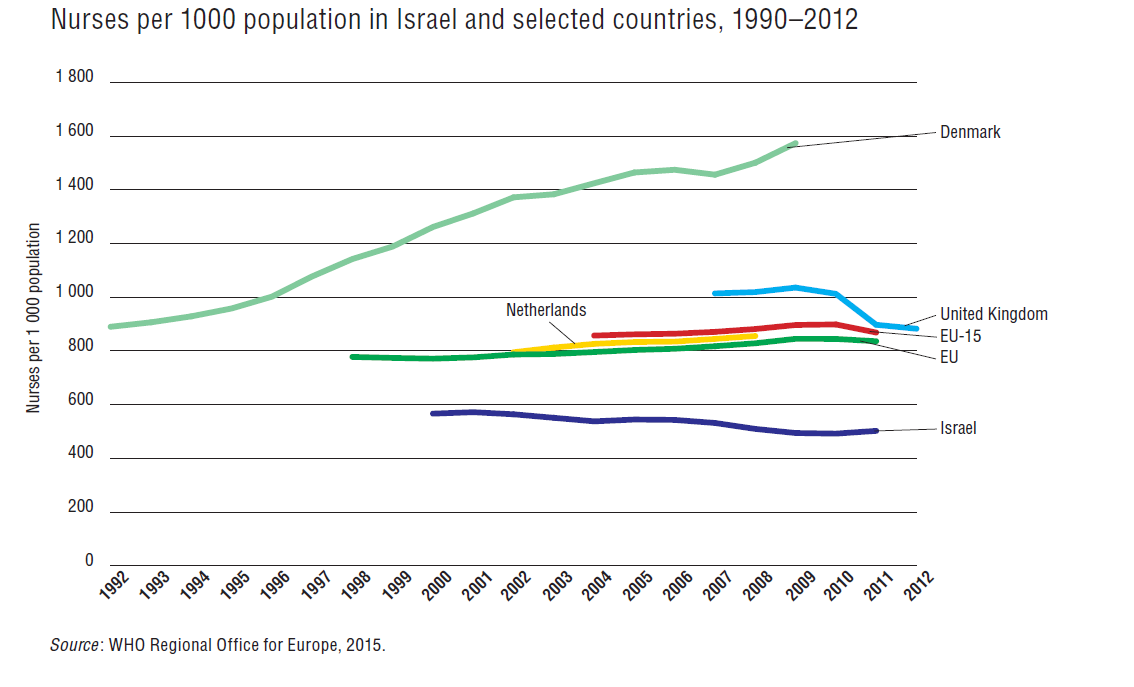
Nurses[18]
The nurse-to-population ratio is declining. In 2013, the ratio of nurses under age 65 to population declined to 5.79 per 1000 population, compared to 5.85 in 2012 and 6.43 in 2005 – a decline of 10%. At the end of 2013, the ratio of state-registered nurses (RNs) under 65 years of age was 4.80 per 1000 population, an increase of 4% from 2005. The percentage of RNs among all nurses in Israel below 65 years of age is on the increase – 83% at the end of 2013 compared with 63% at the end of 2000.
In 2012, the number of new nursing licences began to increase for the first time in a decade, following the intensive recruitment of nursing students and the awarding of grants. It is expected that the results of these efforts will continue to be evident in the coming years.
The percentage of young nurses has declined in the past decade. At the end of 2013, 40% were under 45 years, compared with about 48% in 2005; 39% were aged 45–64 years (38% in 2005), and 21% were over 65 years (14% in 2005). The percentage of male nurses is rising: 11.3% of the RN workforce were men in 2013, compared with 9.6% in 2005.
According to the CBS’s Labor Force Survey (CBS, 2015c), in 2012, 38 000 nurses were employed in the civilian sector in Israel – 4.8 per 1000 population – compared with 5.3 in 2005. The rate of employed nurses is low in the Southern District (3.3 per 1000 population) and Northern District (3.9) compared with the Haifa District (7.1), the Tel Aviv District (5.8), the Jerusalem District (4.7) and the Central District (4.6) (averages for 2009–2011). Three quarters of all nurses are employed in hospitals and one quarter in the community. This rate has been stable for the past two decades.
The nurse-to-population ratio in Israel is lower than the average for EU15 countries (Fig4.5) and has been decreasing in recent years (Fig4.6). Several policy measures have been undertaken recently to increase the supply of nurses, including the expansion of accelerated nursing degree programmes for people with bachelor’s degrees in other fields.
Fig4.6
Dentists
The ratio of dentists (up to age 65) to the population has declined somewhat since the early 2000s, with the number of working age dentists per 1000 dropping from 1.12 in 2000 to 1.00 in 2013. Approximately 40% of working-age dentists are women.
At the end of 2013, 9% of all working age dentists were specialists in Israel and 30% of these were women. The three largest groups of dental specialties are prosthodontics (19% of all specialists); orthodontics (18%); and oral and maxillofacial surgery (16%). Recognition as a specialist is granted by the Scientific Council of the Israeli Dental Association. Other dental professionals include dental hygienists (whose numbers are increasing), dental assistants and dental laboratory technicians.
The vast majority of dentists in Israel work in private clinics or in group practices (Nefesh B’Nefesh, 2008). Some dentists work in school dental services and are paid by the local municipality. The army employs dentists and conducts periodic dental examinations and a wide range of free treatments for soldiers. Dentists also practise in public clinics run by charitable societies. Other employment opportunities include kibbutzim and moshavim, where the dentist is not a member of the community but an employee (Nefesh B’Nefesh, 2008).
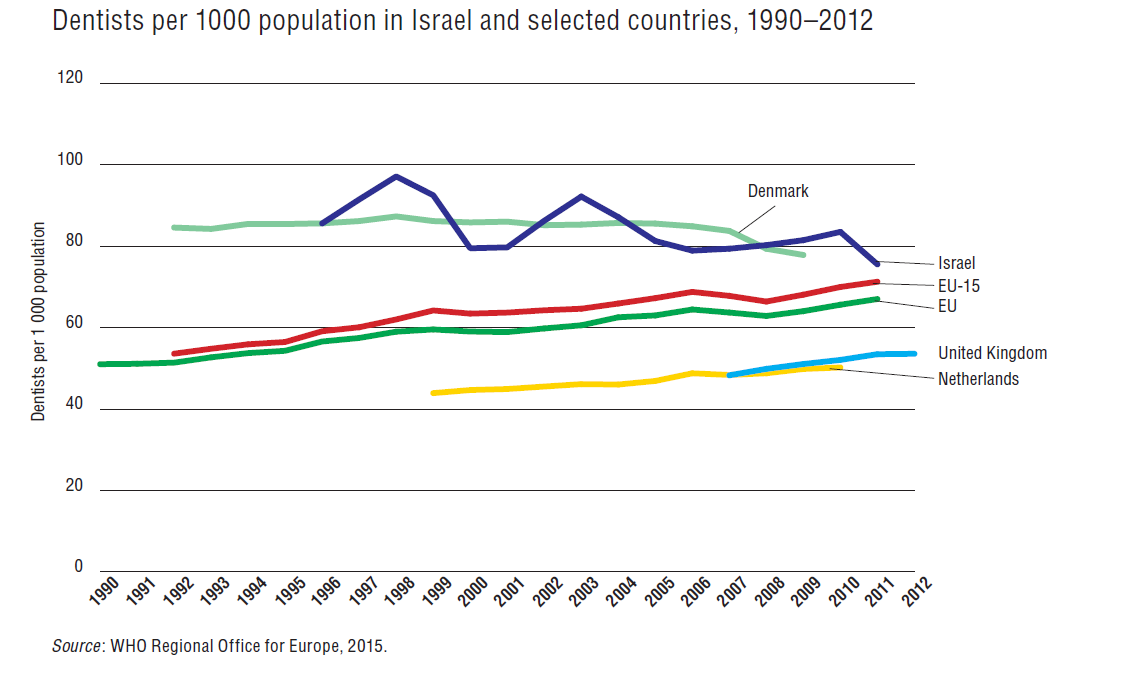
Fig4.7 presents trend data on the dentist-to-population ratio in various countries. It is worth noting that Israel’s ratio is relatively high and that the ratios have been fairly stable for all the countries covered. The dentist-to-population ratio in Israel is slightly above the average for EU15 countries. That gap has been narrowing over time, primarily through an upward trend among EU15 countries.
Fig4.7
Pharmacists
The ratio of pharmacists (up to age 65) to 1000 population has grown from 0.61 in 2000 to 0.80 in 2013. The percentage of pharmacists below the age of 45 years has been growing since the mid-1990s. At the end of 2013, Israel had approximately 8000 licensed pharmacists, of whom 57% were under the age of 45 and approximately 15% were over 65 years. At the end of 2013, 58% of the pharmacists in Israel were women. Pharmacist’s scope of practice is expanding (see section 5.6).
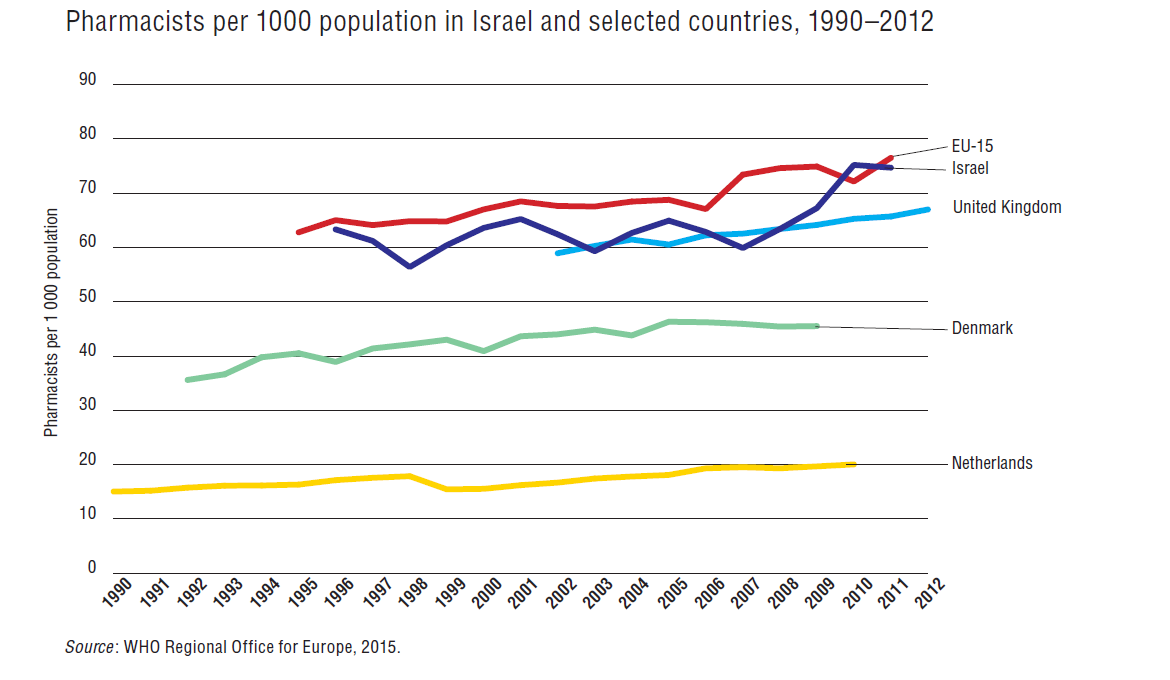
Fig4.8 presents trend data on the ratio of pharmacists (up to age 65) to population in various countries. Note that Israel’s ratio is similar at the time of writing to that in most of the other countries covered; whereas in 1990 it was lower than most of those countries. Israel’s pharmacist-to-population ratio is similar to that of the average for EU15 countries, after increasing markedly in recent years.
Fig4.8
Other health workers
In 2008, the Knesset passed laws regulating the work of physical, occupational and communication therapists; dieticians/nutritionists; clinical criminologists; chiropractors; podiatrists and surgical podiatrists.
Physiotherapists. There are about 0.5 physiotherapists up to age 65 per 1000 population in Israel. Numbers are increasing and in 2013 the ratio was 1.6 times that in 2000. Many physiotherapists are employed in private frameworks, such as health care institutes, community centres, businesses and factories, sports teams and therapeutic swimming pools. Over 2000 physiotherapists are employed in all the health funds, of them some 1500 in Clalit. Around 700 are employed in general, rehabilitative and geriatric hospitals. The number of physiotherapists per 1000 population is similar to the rate in other Western countries.
Nutritionists. There are about 0.19 nutritionists up to age 65 per 1000 population. Again numbers are rising and in 2013 there was 1.4 times the ratio in 2000. This ratio does not differ substantially from the situation in other Western countries.
Speech therapists. There are about 0.35 speech therapists up to age 65 per 1000 population; the 2013 ratio was 2.1 times that in 2000.
Occupational therapists. There are about 0.42 occupational therapists up to age 65 per 1000 population; the 2013 ratio was 1.6 times that in 2000. In recent years, the demand for occupational therapy has grown, following its expansion into a variety of newer areas such as respiratory rehabilitation wards, subacute wards for young people, palliative care wards and national burn centres.
Psychologists. The number of psychologists is increasing. At the end of 2013, there were 1.16 psychologists up to age 65 per 1000 population (compared with 0.87 at the end of 2000); 73% are women. About a quarter (23%) of all psychologists are certified to work as instructors. In 2013, 54% of all psychologists were specialists and their number is rising. Specializations in psychology include clinical (57%), educational (27.7%), social–occupational–organizational (4.2%), rehabilitative (4.2%), developmental (4%) and medical (3%).
CAM practitioners. The estimated workforce in CAM in Israel is more than 20 000 practitioners who have completed a systematic training programme. Overall, half of all alternative treatments make use of traditional Chinese medicine, while the others use different methodologies. Some caregivers in Chinese medicine, in both the public and private sectors, are conventional physicians but many others are not.
Other accredited professions. These include medical laboratory workers (0.8 per 1000 population), clinical geneticists (0.012) and optometrists (0.189).
In 2012, the Ministry of Health prepared projections of needs for several health professions. For physiotherapists, dieticians, speech therapists and occupational therapists, it appears that, overall, the supply is expected to increase substantially in the coming years and that there is no need to significantly expand training. However, in general, the availability of health professionals relative to the size of the population is lower in the north and south than in the centre of the country. Furthermore, some of these professions have seen movement from the public to the private sector, because of better income opportunities. The projections show that nationally there is no shortage but it is recommended that more attention be paid to certain geographical regions that have experienced difficulty in recruiting some types of health professional.
Further information on these health care professionals appears in the sections below and also in sections 2.5 and 2.8.3.
- 18.This section and others about nurses were prepared in consultation with Shoshana Riba and Ruth Rotstein.
4.2.2. Professional mobility of health workers
At the end of 2013, graduates from Israel constituted 41% of all physicians up to age 65 (up from 37% in 2006); other substantial groups were from eastern Europe (40%), western Europe and North America (15%) and Asia/Africa (3%). In 2013, there were 1011 new licences given, with the following distribution of place of graduation: Israel 41%; eastern Europe 34%; western Europe 10%; Asia/Africa 10%; and United States 4%.
About half of all working-age dentists are immigrants. In addition, many Israeli-born dentists travelled abroad for training, so that only 29% of all working-age dentists were trained in Israel, with 49% trained in eastern Europe, 8% in western Europe, 7% in the United States and 7% in Africa/Asia in 2013.
Among licensed pharmacists up to age 65, 53% were trained in Israel, 19% in Asian or African countries, 17% in eastern Europe, 8% in western Europe and 3% in the United States. Since the early 2000s, there has been a major increase in the number of Israelis who go abroad to study pharmacy and then return to practise in Israel. Many of them are Israeli Arabs who study pharmacy in neighbouring Arab countries (particularly Jordan, Egypt and Syrian Arab Republic).
Most (76%) psychologists up to age 65 were trained in Israel, with 12% trained in the United States, 5% in western Europe, 5% in eastern Europe and 2% in Asia/Africa.
4.2.3. Training of health workers
Physicians
Israeli medical schools currently offer several pathways to a doctor of medicine degree. The most common pathway entails six years of study, of which the first three focus on the basic sciences and the latter three focus on clinical knowledge and skills, with one year of rotating internship and a submission of a scientific thesis. Entrance to that pathway does not require a bachelor’s degree. Another pathway is open to university graduates (with a bachelor of science degree) who have done significant coursework in the basic sciences, and it entails only four years of study in medical school. A third pathway is available to students who completed basic science studies in a medical school outside of Israel. These students can receive their medical degrees after completing an additional three years of clinical studies in an Israeli medical school. The distribution of students between the three pathways is currently approximately 80%, 15% and 5%, respectively.
Most students enter medical school after completing their compulsory army service (two years for women and three years for men) or other voluntary assignments (i.e. a period of a “National Service”).[19] A small number of students who have signed on to serve as physicians in the army after completing their medical studies can begin those studies immediately after high school.
Israel has a well-developed system of specialty training, with residencies lasting four years on average (with significant variation across specialties). Board certification is handled by the IMA’s Scientific Council in cooperation with the Ministry of Health and the various specialty societies. Typically, residents take their specialty examinations in two stages, with the first stage taking place after two years of residency and the second taking place after completion of the residency. Most residency places are funded by the hospitals out of their regular operating revenues; there is sometimes special government funding for a certain number of places, for example in the effort to encourage employment of immigrant physicians in the early/mid-1990s. Israel also has a well-developed system of subspecialty training and fellowships. Many promising Israeli physicians pursue fellowship training abroad, typically in the United States or Europe.
In recent years, there has been growing interest in moving a greater proportion of residency training from hospital settings to community settings. This is because a growing proportion of medical care is taking place in the community, and it is important to prepare young physicians for this changing reality. This effort has had some success in family medicine training programmes, but significant barriers to change remain in other specialties.
Nurses
By the end of 2015, all nursing studies will be to a bachelor of science in nursing and will be carried out under the auspices of universities and colleges. This is expected to include 2800–2900 students.
The government is acting vigorously to increase the number of nurses being trained. Over five years, the number of nursing students has doubled with 2850 students beginning their studies in 2014 compared with 1692 in 2010. However, this is still not enough to reach the nurse-to-population ratio declared in government policy.
The number of RNs under 65 years who have graduated from advanced courses is increasing, from 39% in 2005 to 43% in 2013. At the end of 2013, 16 869 RNs under 65 years had completed advanced courses: 2.1 per 1000 population.
The advanced courses are intended for RNs with academic degrees who are interested in working in specialized areas such as emergency medicine, intensive care, nephrology or operating rooms. In order to provide high levels of professional care in these units, the RNs are required to undertake additional training. The advanced courses last approximately one year, at the end of which the nurses receive a diploma and this is recorded in their file in the official registry of nurses.
All the universities and several of the colleges offer master’s degree programmes in such areas as nursing, health care management, epidemiology, occupational medicine and gerontology. It is estimated that the number of nurses with master’s degrees is in the thousands and 300–400 nurses hold academic doctorates (PhDs).
Dentists
Regardless of place of training, since 1992 it is necessary to pass a government licensing examination in order to work as a dentist in Israel. Almost all those trained in Israel pass the examination, and approximately half of those trained abroad do so.
Pharmacists
In 2013, 167 new licences were granted to pharmacists, of whom 56 had trained in Israel. In previous years the numbers were significantly higher: 300 overall of whom over 150 had been trained in Israel.
Other health workers
Physiotherapists. Physiotherapy studies last four years and graduates receive a bachelor’s degree in physiotherapy. In recent years, the average number of diploma recipients was a little over 200 a year.
Nutritionists. Nutrition studies last three years with an internship of up to six months (in hospitals and/or in the community). On overage, 260 nutritionists graduate and receive a diploma each year.
Speech therapists. Speech therapy studies last three and a half years, including supervised practical period, and lead to a bachelor’s degree. These studies are currently available in two universities and five colleges. Every year, about 200 new graduates enter the system.
Occupational therapists. Occupational therapy studies last four years and lead to a bachelor’s degree. Three universities provide an option of doctorate study, which last three and a half years. Every year, some 225 new occupational therapists enter the market.
Psychologists. To work as a clinical psychologist, the requirements are a master’s degree in psychology in a clinical area, which usually takes two years, and a four-year half-time internship (partly in hospital and partly in a community setting). In recent years, approximately 550 new licences were granted to psychologists, of which approximately 400 were granted to those trained in Israel.
CAM practitioners. There are nearly 100 CAM training programmes, including brief courses (several months long) by private individuals and institutional schools of varying quality. None of them gives an academic degree in this area. Some meet international standards and are accompanied by a strict supervision mechanism, while others are unsupervised. Training at some of the bigger schools entails 3000 hours of study over four years.
- 19.Israelis exempt from military service can begin their medical studies immediately after graduation from high school.
4.2.4. Career paths for physicians
There are several career paths available to physicians in Israel. One is the academic path and both full academic and clinic appointments are available. A second pathway is to advance up the organizational hierarchies in the HPs, hospitals or government (Kokia, Siegal & Shemer, 2008). A third pathway is professional through increasing skill level and/or extent of specialization. This last is often combined with efforts to rise on the academic or organizational ladders, but this is not always the case.
4.2.5. Career paths for nurses
As part of the transformation of the nursing profession to an academic profession with broad authority, the academic level of those entering the profession is rising and the wish and potential to develop a career is growing. Israel offers nurses three main career paths: clinical, academic and management.
Clinical. Professional development is in the context of direct care of a patient at various levels, from specialist in-service training in selected units such as intensive care, emergency medicine, oncology, through to the status of specialist nurse with the authority to provide independent treatment for a variety of clinical problems experienced by the patient in the nurse’s care.
Academic. The basic academic training pathway for nurses requires the development of academic staff within the training institutions. This is a teaching and research pathway for nurses, from a master’s degree to an academic doctorate in nursing and through to the status of professors, as required by each academic institution.
Management. The management pathway allows for the development of a hierarchical management scale in nursing, from nurses in charge of their unit through to the head nurse at a medical institution. In recent years, many positions have opened up in the field of health system management. For several years, these positions have been open to nurses with advanced degrees, master’s degree or higher. These positions include quality assurance, responsibility for the service, risk management, spokesperson, internal audit and so on.