-
21 March 2025 | Country Update
Electronic medical records data to be shared across more organizations to improve integrated care -
10 May 2023 | Country Update
New dashboard with real-time data on quality of hospital care and COVID-19 -
26 November 2019 | Policy Analysis
Greater access, transparency and uniformity of personal medical records for all residents -
28 February 2019 | Country Update
Improving accessibility to digital medical records
2.7. Health information management
In 2023, the Ministry of Health has launched a dashboard called “World of Data” (https://datadashboard.health.gov.il/portal/dashboard/health). The website presents various indicators on the performance of the health system, both current and historic. It provides a centralised, interactive platform that brings together previously scattered information. Additionally, it makes data more easily accessible to the public and can help inform choice of provider decisions.
The dashboard includes data on COVID-19 such as incidence, prevalence, morbidity and treatment (for example, number of daily hospitalizations and vaccinations). The dashboard also presents interactive data on clinical treatment and hospital quality of care for general, mental health and geriatric hospitals and well-baby clinics. Rehabilitation hospitals are excluded. The data includes PROMs and PREMs, and can be disaggregated by hospital and region. It also includes statistic aggregated data about complaints to the ombudsman, who addresses public complaints. This data can be disaggregated by type of complaint and health plan.
Authors
References
Ministry of Health. (31 May 2023). The Ministry of Health is expanding the accessibility of data to the public (in Hebrew). Retrieved from https://www.gov.il/he/departments/news/10052023-01.
According to the Israeli Patient's Rights Law, all patients are entitled to have easy access to their personal medical records (PMR). All four health plans (HPs) already provide their members with access to their digital PMR – which are accessible online via the HPs’ websites and mobile apps. However, information is sometimes incomplete, only includes services provided by the HP, and the scope of information varies among the HPs. The ministry of health (MoH) has regulated (in November 2019) the way and type of information that all HPs have to make available electronically for their members about their PMR, which includes structured data (text, tables, numbers) and unstructured data (such as images or video). In addition, the MoH will provide the HPs with data about their members’ PMR for services provided directly by the MoH such as hospital care, mental health care, and prevention care. Access to PMRs will be granted to all HPs’ members free of charge.
This initiative aims to enhance access, transparency and uniformity regarding the way and type of data that HPs have to make available online. It will increase transparency between health professionals and patients, and potentially encourage the involvement of patients in managing their own care.
Authors
References
In 2018, the Parliament updated the law that entitles patients to receive their medical records (MR) following treatment or hospitalization. Previously, patients had to pay out-of-pocket (OOP) for their MR - from NIS 48 (€12) for a printout to NIS 113 (€27) for an electronic copy. The new regulation substantially decreases the OOP payment for patients, such that they can now receive their digital MR for free immediately after care. To obtain their MR retrospectively for up to five years, patients pay a maximum of NIS 10 (€2.50), and the charge for multiple MRs should not exceed NIS 50 (€12). Yet, commercial insurers need to pay the full amount for MRs. Since this measure intends to improve patients’ accessibility to their digital MRs, and not lower costs for commercial insurers, the MoH will need to monitor this new legislation to prevent insurers from requesting that patients acquire their MR to avoid full payment.
Authors
References
MoH (2018) The payment amount for production of digital medical records was limited to only 10 shekels (in Hebrew):
https://www.health.gov.il/NewsAndEvents/SpokemanMesseges/Pages/27122018_1.aspx
2.7.1. Information systems
All HPs and the hospitals have sophisticated information systems that include electronic medical records, data on activity levels, services provided and quality of care (see section 4.1.4). Each of these organizations makes extensive use of their own data systems at both the individual care level, and to make broader policy decisions.
In addition, there are several systems for aggregating data across providers so that the data can be used to monitor and analyse overall national developments, including:
Infectious disease surveillance system. By law, any provider coming into contact with a patient who has any one of a long list of infectious diseases must report this information to the Ministry of Health.
Disease registries. These are maintained by the Israel Centre for Disease Control (ICDC) and other units of the Ministry of Health and cover such topics as cancer, trauma, low birth weight, diabetes and heart disease.
National Hospitalization Database. This Ministry of Health database includes micro-level demographic, diagnostic and treatment data for almost all hospitalizations.
Hospital activity data. The Ministry of Health has a system of monitoring and disseminating aggregate hospital activity data (at the level of the hospital and the department).
Specific information systems on areas that benefit from government financial support. The Ministry of Health collects data on psychiatric hospitalizations, visits to emergency departments (EDs) and institutional LTC.
Cause of death statistics. The Central Bureau of Statistics (CBS)/Ministry of Health have a system for monitoring and reporting causes of death.
The National Quality Measures Programme. This collects information from the HPs on over 50 measures of the quality of community-based care (section 6.1.3).
Deaths and other adverse events in hospitals. Data are collected by the Ministry of Health for reporting and investigation.
Hospital-acquired infections. The Ministry of Health has an information system for monitoring and analysing infections in hospitals.
Disease registry systems. The Ministry of Health has registries for a number of diseases including for cancer, tuberculosis HIV/AIDS.
Workforce registry systems. These cover physicians, nurses, dentists, pharmacists and others.
In addition, there are several important national population surveys that periodically collect nationwide data:
The Health Survey. This is carried out by the CBS and the Ministry of Health and collects information on self-perceived health status, health behaviours, utilization of services and so on. The most recent survey in the series was carried out in 2009.
The CBS Family Expenditure Survey. This annual survey provides information on spending for many different categories of health care.
The CBS Labor Force Survey. This ongoing survey always includes a set of questions regarding health and health care.
The MJB’s biannual survey into the public’s perceptions of the level of services provided by the HPs. The topics covered include satisfaction with various dimensions of care, access/barriers to care, waiting times, and the nature of the interactions with providers of care.
ICDC surveys. Various surveys are carried out by the ICDC, including the KAP surveys, which look at knowledge, attitudes and practices related to health behaviours (ICDC, 2015); the MABAT series, which look at nutritional patterns in various age groups (ICDC, 2014); and the European Health Interview Surveys (ICDC, 2012), which collect information on health status and service utilization in a manner that is comparable to similar surveys carried out in various European countries.
2.7.2. Health technology assessment
In 1998, Israel established a formal process for setting priorities for adding new services to the benefits package. Each year, the government decides how much money it will allocate for these additions. In parallel, the Ministry of Health solicits recommendations for which new technologies/medications (henceforth referred to as technologies) should be prioritized for inclusion in the benefits package. HPs, pharmaceutical companies, the IMA, patient organizations and other groups submit recommendations, along with supporting analytic material. These proposals are reviewed by a staff unit within the Ministry of Health, which analyses the likely costs and benefits of each proposal. This background material is brought before a public commission that recommends to the Ministry and the government which new technologies should be adopted, given the previously determined budget constraints (Chinitz et al., 1998; Shani et al., 2000; Shemer, Abadi-Korek & Seifan, 2005).
In 2005, a subcommittee was established, consisting of representatives of the HPs, the Ministry of Health and the Ministry of Finance, to review and refine the more technical components of the background information (such as the price and volume projections), thereby allowing the full committee to focus its efforts more on values and priorities. While this explicit priority-setting process does have various problems and limitations, it has been considered by many health policy analysts in both Israel and abroad to be ground breaking on an international scale (Chinitz & Israeli, 1999).
In analysing the costs and benefits of proposed new technologies, the professional staff of the Ministry of Health examine various factors:
- health problems and conditions that the new technology would address;
- extent to which the benefits package already includes treatments for those problems and conditions, and the efficacy of those treatments;
- number of patients whose care would be improved;
- extent of the improvement in terms of duration and quality of life;
- health risks associated with the new technology;
- number of units of the new technology that would be likely to be consumed if the new technology were to be adopted;
- projected unit price of the new technology;
- total cost to the system of adopting the new technology; and
- potential savings from reduced consumption of existing technologies, for which the new one serves as a substitute.
In carrying out these analyses, the Ministry of Health staff rely on a number of sources, including:
- background materials submitted by the person/organization that proposed the adoption of the new technology;
- recent scientific evidence from published articles, testimony and correspondence;
- analyses carried out by health technology assessment units in other countries;
- assessments of panels of clinical experts, such as the various national medical councils, regarding the expected clinical benefit and the number of affected patients;
- epidemiological data available from government sources, such as the ICDC and various disease registries; and
- relevant data on consumption and pricing from the HPs, hospitals and other provider organizations.
The Ministry of Health staff employ a two-stage annual funding cycle. First, from a preliminary assessment of the added medical value, costs and benefits, and in light of the amount of new money available that year, they weed out those technologies that are not of sufficient promise to be discussed in the public commission. Second, they carry out in-depth analyses for those technologies that have made it through the first phase. For each technology, a detailed analysis (typically 10–20 pages) is prepared. The analyses for all candidate technologies are published in a book prepared for the public commission. This book is not distributed to the general public but is distributed to the key interested parties and is also made available to academic researchers studying relevant issues. Table2.1 indicates the number of new technologies considered and added to the benefits package in each funding cycle since 1999 (mostly new medications for cancer, heart disease, etc.).
Table2.1
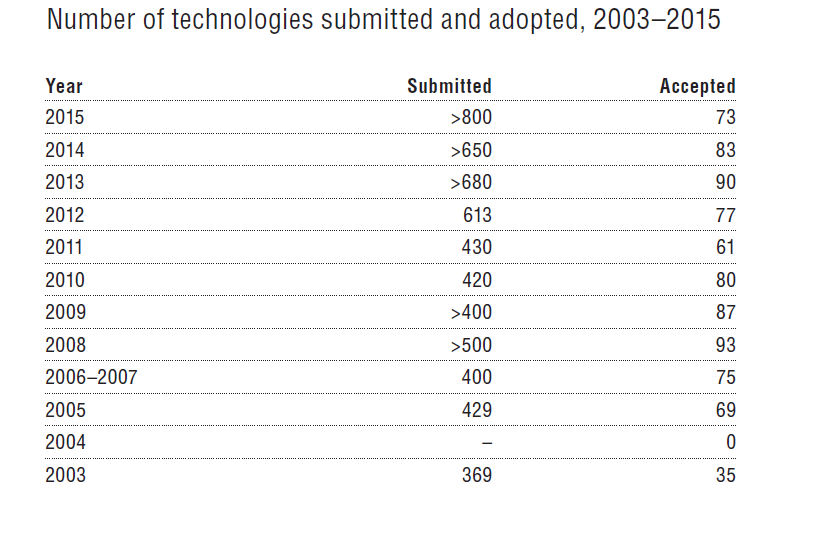
There is general consensus that the Ministry unit dealing with this process is understaffed relative to the number of health technology assessments they need to prepare (650–700 annually in recent years), the tight annual time frame in which they must prepare them, and the sought-after levels of analytic depth. Additional professionals with the relevant skills do exist in Israel, but budget constraints prevent the Ministry of Health from hiring them for this purpose.
In evaluating the new technologies, the unit makes use of relevant clinical trials, systematic reviews, and submissions from those proposing that the technology should be added to the benefits package, plus additional information on expected volume and/or price from national disease registries, HPs, hospitals and pharmaceutical companies.
In its 15 years of operation, the items approved by the public committee include both preventive as well as curative services, as well as those intended to extend life along with those intended primarily to improve the quality of life. The relative emphases given to these have varied over time.
The system has proven to be an effective one for national decision-making and has earned the support of the public, the relevant government ministries, the courts, and the key health care providers.