-
07 November 2023 | Policy Analysis
Shifting medical inpatient payments from per diem to global budgets -
17 May 2017 | Policy Analysis
New cap on hospital revenues which distinguishes between different types of activity
3.7. Payment mechanisms
Context
Over the past few decades, the number of hospital beds per population in Israel has reduced from 3.79 beds per 1,000 population in 2000 to 2.99 beds per 1,000 in 2022 (OECD, 2023). This decrease was a result of population growth, rather than deliberate policy action. It has raised concerns about the quality of care on internal medicine (IM) wards, demonstrated by the high percentage of readmissions (27% in 2015 (Tur Kaspa, 2019)). IM bed occupancy rates are also high, reaching a yearly average of 88.6% in 2022 (Information Division of the Ministry of Health, 2023). High occupancy rates are especially common during the winter season and can cause patient flow issues. Patients are also increasingly complex, with multiple chronic conditions that need to be managed.
In Israel, hospitals sell services to health plans (HPs), payments methods and prices are regulated by the MoH through a legally binding (maximum) price list (the Health Services Payment Law). This reform changes the legislative framework for provider payments.
Impetus for the reform
In response to the high occupancy rate of IM wards, the Ministry of Health (MoH) initiated a healthcare reform, aimed at shifting care from inpatient to other settings and to enable quicker discharge to geriatric institutions or nursing homes (Tur Kaspa, 2019).
In 2019, the MoH established a committee to propose solutions for improving the quality of inpatient care in general hospitals. This reform was formulated based on the recommendations put forth by the committee.
Main purpose of the reform
This reform is expected to create incentives for hospitals to reduce the volume of patients in internal medicine wards, while maintaining high-quality care standards. It incentivizes HPs to shift care to outpatient and home-based settings, particularly for patients waiting to be discharged.
Content/characteristics
The legislative reform consists of four main changes:
- Promoting home care: Hospitals are required to enter into agreements with HPs to provide hospital-at-home services. Payment for hospital-at-home is included in the global budget, with hospitals facing a 1% reduction in the global budget if they do not expand this service. This is expected to reduce the number of patients arriving to IM wards, as they will be treated at home.
- Shift in payment method: Payment for IM wards was shifted from a per-diem base to global budgets. HPs now pay predetermined budgets to hospitals based on the IM’s previous years’ activity volume and cost. This is expected to create incentives for hospitals to reduce the number of “unnecessary” inpatients and reduce lengths of stay.
- Pay for performance model: Payment beyond the global budget is contingent on adherence to “quality of care” indicators measured through various tools, including patient-reported satisfaction collected through a survey, staffing levels per bed and readmissions rates. This measure aims to avoid hampering quality of care and counteract the financial incentive to contain costs created by the introduction of global budgets.
- Penalty for delayed patients: Once a patient is discharged, the HP are responsible for their care. Hospitals can charge extra payments from HPs for each day of hospitalization once a patient is categorized as “medically fit for discharge”. This change creates financial incentives for HPs to find alternative settings of care for patients that can leave IM wards, but are not suitable for home discharge.
Authors
References
Information Division of the Ministry of Health. (2023, 2 21). Hospital bed occupancy by department and month (in Hebrew). Retrieved from gov.il: https://www.gov.il/he/departments/publications/reports/hospital-beds.
OECD (2023), Hospital beds (indicator). doi: 10.1787/0191328e-en (Accessed on 20 September 2023)
Ministry of Health. (2023, 2 15). Accounting law between hospitals and health funds for the years 2021 to 2025 (accounting for health services in general public hospitals) 2021 (in Hebrew). Retrieved from gov.il: https://www.gov.il/he/departments/legalInfo/hityaalut01.
Tur
Kaspa, R. (2019). Committee report on improving inpatient care in
internal medicine wards in the state of Israel (in Hebrew). Jerusalem:
Ministry of Health. Retrieved from https://www.health.gov.il/PublicationsFiles/internal_dept_treament_improvment_report_2019.pdf.
Since 2005, the Israeli Ministry of Health (MoH) has been setting annual caps (floor and ceiling) on hospitals' revenues from each health plan (HP) to each hospital. The latest cap on hospital revenue (2017-2019) specifies a minimum payment amount (lower cap) set as 93% of the previous year’s expenditure from each health plan (HP) to each hospital. If an HP consumes services which have an aggregate cost of less than this lower cap, then they still pay 93% of the previous years' expenditure. If the upper cap is exceeded, then HPs pay a percentage of the full cost (less than 100%).
The innovation for this update is that it sets different discounts and rules for three different types of hospital activities: 1) “inpatient non-procedural activities” paid by per diem; 2) “inpatient procedural activities” paid mainly through procedure-related groups (PRGs); and 3) “other” activities, which include outpatient procedural activities and diagnostic exams, paid mainly through fee-for-service (FFS) and PRGs and inpatient procedures paid by per diem.
For procedural activities there are two upper cap thresholds. When HPs spend 100-108% of the previous year’s expenditure, they pay only 55% of the costs of the 8% of the exceeding consumption (step 1). If they exceed 108%, they pay only 33% of the expenditures beyond the 108% (step 2).
For inpatient non-procedural activities there is one upper cap: if HPs exceed the previous year’s expenditure for this activity, they pay 60% of the costs of the exceeding expenditures, but the hospital receives only 20% of these costs. The remaining 40% is funneled to the National Insurance Institute to be reallocated to the HPs, contingent on them developing home care as a substitute for inpatient non-procedural care.
These different discount rates align the economic incentives of hospitals and HPs. This new arrangement disincentivizes hospitals in treating non-procedural patients, because they receive only 20% of the income. It also discourages HPs to hospitalize non-procedural patients, because they receive a modest discount of only 60% of the costs (compared to the generous discounts they receive for procedural patients).
Emergency room cases are exempt from the cap in order to incentivize HPs to avoid unnecessary emergency visits and to develop emergency care in the community at lower costs.
The main objectives of splitting the cap into activity types are to: 1) incentivize hospitals to allocate more efforts to procedural activities (instead of non-procedural activities); and 2) encourage HPs to develop community care (particularly homecare and community-based emergency care) as a substitute for hospital care.
References
Government decision number 1871, 11 August 2016 (http://www.pmo.gov.il/Secretary/GovDecisions/2016/Pages/dec1871.aspx, accessed 17 May 2017)
3.7.1. Payment for health services
This section discusses in turn payment for health services in general hospitals, psychiatric hospitals or psychiatric wards in general hospitals, public mental health clinics in the community, public health services, dental care and pharmaceutical care (Table3.6).
Table3.6

General hospitals
Approximately 80% of general hospital revenue comes from sales of services to HPs. Other sources of revenue include the IDF Medical Corps, private insurers, the NII, the Ministry of Health and OOP payments. This section focuses on revenue from the sale of services to the HPs and on arrangements in what are referred to in Israel as “public hospitals”, comprising both government and non-profit-making hospitals (these include Clalit HP hospitals, non-profit-making “mission” hospitals, and others such as the Hadassah Medical Organization).
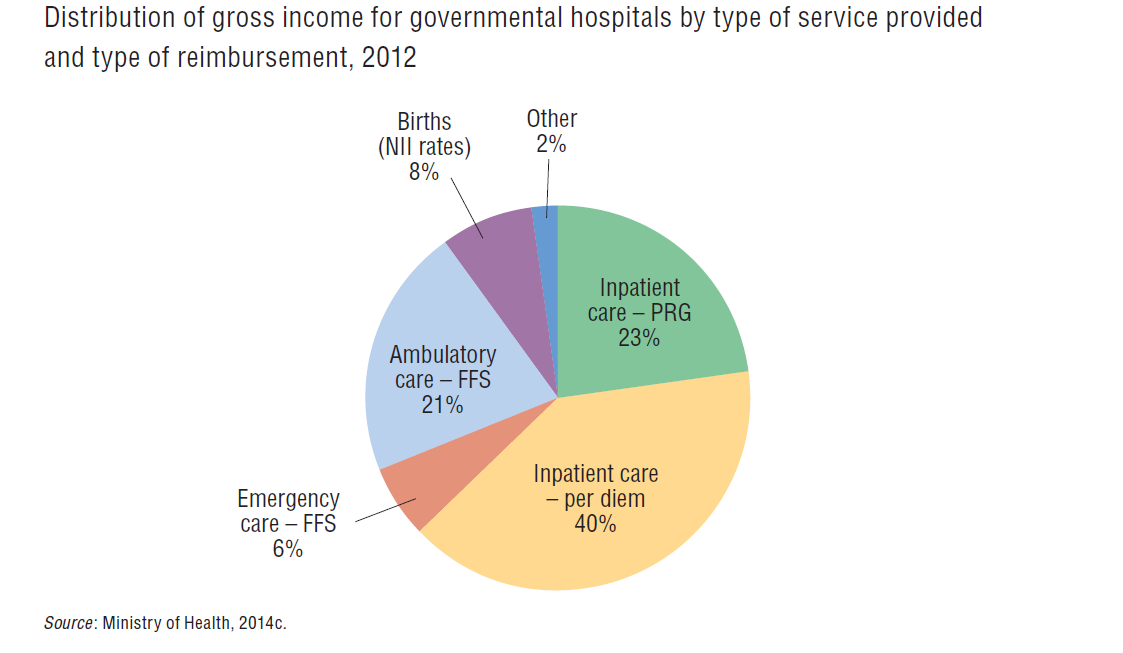
Since the enactment of the NHI Law in 1995, public hospitals in Israel are reimbursed for inpatient care primarily by per diem fees and secondarily by case payments. Ambulatory care in hospitals is paid on a FFS basis (Fig3.10). Maximum price lists for public and non-profit-making hospitals are mandated by law and set by the government through a joint Ministry of Health and Ministry of Finance Pricing Committee. Government hospitals are subsidized by the government retrospectively.
Fig3.10
Until 2010, Ministry of Health price lists were not based on a methodical costing process. Per diem and FFS rates were set about three decades earlier based on the historical expenditure of certain hospitals. Since then, rates had been updated for inflation, but no major recalculations were undertaken despite significant changes in cost structure from technical and medical advances. Consequently, some activities were underpaid and others overpaid. The gaps between costs and prices create a series of inefficiencies caused by the influence of economic considerations on medical decisions.
In order to tackle these inefficiencies, the Ministry of Health concluded that it was important to narrow the gap between costs and prices through two changes: building a consistent costing and pricing mechanism and substituting the per diem payments with payments based on activity. The Ministry of Health thus initiated a hospital payment reform (the PRG reform), which consisted of gradually costing hospital activities and setting differential pricing for inpatient care per procedure. Once the price for a specific procedure has been set, the per diem payment is replaced by the PRG. This process has been an ongoing incremental reform that started in 2002 and has been enhanced since 2010 by the Ministry of Health. In 2015, there were over 280 PRGs, which account for half of the procedures. The plan is to adjust the PRG for case mix and severity of illness in the future (Brammli-Greenberg et al., in press).
The FFS charge list in outpatient care. A FFS charge list established by the government regulates payment for hospital outpatient care in ambulatory clinics and EDs. The list includes 1500 rates for ambulatory care and about 65 rates for day hospitalizations. The day hospitalization component has been increasing as technologies improve and allow procedures to be performed with no need of overnight stays. Payment for outpatient department services accounts for approximately 20% of hospital revenue; emergency care accounts for an additional 6% (Fig3.10).
The per diem rate. Two thirds of inpatient admissions are reimbursed on a per diem basis; they account for half of the interventions performed. In 2015, there were about 50 per diem rates, which differ according to the department (e.g. intensive care units are higher than the standard rate, while geriatric and mental health units are lower) and period of hospitalization (the first three days are more costly that the fourth and so on). In a few specific cases, there are different rates by age (e.g. intensive care for children younger than 4 years).
Case payments, PRGs. During the 1990s, differential case payments were established for about 30 types of admission. The defining characteristic of the case is the principal procedure carried out (rather than the diagnosis, as is the case in countries using diagnosis-related group systems). Since 2010, the range of conditions for which case payments have been established (as an alternative to per diem reimbursement) has significantly increased. In mid-2015, case payments accounted for approximately 23% of total hospital revenues, and 33% of hospital inpatient revenues (Brammli-Greenberg et al., in press).
The revenue cap
A significant proportion of a hospital’s expenditure is fixed and does not vary according to the volume of hospital activity. The prices HPs pay for services purchased from hospitals reflect “average prices”, which include fixed costs and are, therefore, higher than the marginal cost of the service purchased. A payment scheme that relied solely on these average prices would have created incentives for hospitals to increase volume (either hospitalization days or procedures), which would have led to increases in HP expenditure on hospitalization services, increases in public expenditure on health, and might even have led to moral hazard. In order to remove this incentive, a hospital revenue cap was established in 1997, and the rules of the capping regime are modified every three years. The capping system’s goal has been to eliminate incentives for hospitals to overprovide inpatient care, and to constrain growth in expenditure, particularly that related to hospital services.
A revenue cap is set by the government for each hospital vis-à-vis each HP; since 2014, this is not published publicly. It is a function of the previous year’s HP’s consumption in each hospital plus an adjustment to reflect projected demographic growth, hospital bed growth and price change (in particular, the Ministry of Health’s PRG price list and per diem rates).[14]
The model set in 2013 for the years 2014–2016 is innovative in relation to previous ones in that it sets a minimum for the total amount that each HP will pay each hospital each year (95% of the previous year’s consumption by the HP). This is done to financially protect the hospitals. In addition, the current capping system has three steps, each with different payment rates and incentives. HPs that purchase services beyond the cap pay the cap plus a percentage of the price of those services purchased beyond the cap.[15]
Individual agreements set between hospitals and health plans
HPs and hospitals also are allowed to negotiate alternative reimbursement contracts, which, if both sides agree, can take the place of the official cap. This is intended to allow greater flexibility and risk sharing among players. Since the early 2000s, HPs have set individual arrangements with more than 80% of hospitals, in which the hospitals provided bigger discounts than the capping mechanism. The individual contracts provide discounts that vary among HPs and among hospitals.
By virtue of its role as the owner of the government hospitals, the Ministry of Health reviews and approves all contracts with the government hospitals. Until recently, the Ministry did not play a significant regulatory role in determining the nature of contracts signed by other hospitals. It was felt that this would not be appropriate, since the Ministry, as the owner of its own hospitals, is also competing with those other hospitals. However, in recent years, the Ministry of Health has been more active in this regard.
Additional considerations
Despite the reimbursement mechanisms, the Ministry of Health subsidizes retrospectively almost all public hospitals. Subsidies have more than doubled in the last decade (from around €75 million in 2006 to €170 million in 2012) (Ministry of Health, 2014c). Nevertheless, both public and non-profit-making hospitals have faced growing deficits in recent years. The extreme case of this was the near-bankruptcy of the private non-profit-making Hadassah Medical Center in 2014. The hospital did not break up because the Ministry of Health provided massive financial aid and increased the cap ceiling.
Psychiatric hospitals or psychiatric wards in general hospitals
From the mental health reform in June 2015, HPs purchase psychiatric services from psychiatric and general hospitals. Payments for the services are based mainly on per diem fees. Similar to other hospital services, prices are set by the Ministry of Health. In addition, similar to other hospital services, the government sets maximum revenues caps for each hospital for each HP (Levi, 2013). There are two main differences between the physical health and the mental health cap: (1) there is no required minimum of payment from HPs for mental health service, in order to encourage HPs to divert care from mental health hospitals to the community; and (2) there are two cap ceilings that contain the increase of expenditure on mental health inpatient care by eliminating any incentives for hospitals to increase volumes beyond those prior to the mental health reform.
In addition, HPs and hospitals are allowed to make further arrangements instead, or in addition to, the capping mechanism, similar to the discounts that hospitals provide the HPs for the services of general hospitals.
Public mental health clinics in the community
Until June 2015, the Ministry of Health provided and funded directly mental health services through its own clinics. Since that date, HPs are the providers and purchasers of mental health services and can purchase these services from the Ministry of Health-operated community clinics, which provide outpatient psychosocial services such as psychotherapy, group therapy, mental health rehabilitation (post hospitalization), social work, and pharmacological management and follow-up (Ministry of Health, 2015b). For each patient, the HP will pay the mental health clinic for two initial “diagnostic” visits. Then HPs will pay prospectively for the treatment itself according to a treatment plan set by the clinic, which is a function of the diagnosis. There will be different treatment rates based on (1) age (children and adults), (2) average length of treatment (short or long term), and (3) type of treatment (individual or group).
Public health services
In Israel, the main public health service that is included in the NHI benefits package is the preventive care clinics for early childhood and pregnant women (Tipat Halav). There are about 1000 such clinics, many of which are owned by the Ministry of Health. HPs also own some of the clinics, mainly in towns and rural areas, as do several municipalities, such as Jerusalem and Tel Aviv.
The Ministry of Health provides preventive care directly through its own clinics and purchases services from municipality and HP clinics. The Ministry of Health reimburses municipalities for 70% of their expenditure. For HP clinics, the Ministry of Health provides vaccines free of charge and partially reimburses them retrospectively (based on pay for performance) for services provided.
Dental care
Since 2010, dental care for children up to 12 years of age has been provided within the NHI health basket. HPs are reimbursed prospectively for this type of service based on the number of children under 12 years of age in each HP. This capitation payment for paediatric dental care is separate from the main NHI capitation payment.
Pharmaceutical care
As pharmaceuticals are part of the NHI benefits package, the HPs receive funding for them via the main capitation formula. They also charge coinsurance from insurees (see section 3.4). HPs purchase pharmaceuticals directly from manufacturers. Each HP negotiates prices vis-à-vis each manufacturer.
- Vadim Perman and Boaz Aricha contributed important information and insights for this chapter.
- 14.The cap set for 2014–2016 was the gross spending in the previous year (i.e. disregarding individual discounts given by each hospital to each HP under individual agreements), added to 0.8% for demographic growth, 0.6% for hospital bed growth, and increases in Ministry of Health’s list prices for the coming year.
- 15.From the cap (100%) up to 102%, HPs pay the cap plus 70% of the price of the services; from 102% to 112% of the cap HPs pay no more than 33% of the price; above 112% of the cap HPs pay up to 65% of the price.
3.7.2. Paying health workers
Payment of physicians
In Israel, most physicians work as salaried employees of the HPs or the non-private hospitals; many others work as independent contractors for these institutions. A collective bargaining agreement between the IMA and the major employers governs the payment terms for employed physicians in those institutions. Physicians working independently are not covered by the agreement and instead are engaged via individual contracts.
Community-based services
In Clalit, the PCPs who are employees are paid on a monthly salary basis plus a capitation fee for each patient on the PCP’s roster beyond the norm (which reflects the number of patients, their age and their health status); this is referred to in Israeli as passive capitation as it does not depend on whether the member visited the PCP. Independent PCPs are paid on a straight capitation basis. Specialists are paid on an active capitation basis (i.e. a set amount for each patient who visits during a quarter-year, irrespective of the number of visits) plus FFS payments for various procedures (according to a set fee schedule) up to a quarterly ceiling.
In Maccabi, the majority of physicians (over 80%) are independent contractors. Both PCPs and specialists are paid on an active capitation basis plus FFS for various procedures, with the FFS component being a large share of compensation for the specialists.
In Leumit, the employed PCPs are paid on a passive capitation basis (i.e. irrespective of whether patients visited during the most recent quarter-year). Specialists and the relatively small number of independent PCPs are paid on active capitation basis, as were employed PCPs until recently.
Meuhedet uses a mix of these reimbursement systems.
Hospital services
In the government and non-profit-making hospitals, physicians generally work on a salaried basis, and for most such hospitals the terms are specified in the collective bargaining agreement. Salary levels are primarily a function of role (resident, board-certified specialist, department chair, etc.) and years of work experience.
In addition, some physicians (usually surgeons) in Ministry of Health hospitals are given the opportunity to work beyond the standard working hours for premium pay, which can be either in the form of an hourly rate or a per procedure rate. In the Clalit hospitals, there is a similar arrangement. In the Hadassah hospitals, physicians can also receive additional FFS payments for treating patients enrolled in the private medical service programme (see section 3.4.2).
In Assuta, a network of private hospitals owned by Maccabi, surgeons are not paid through the hospital but are typically paid on a FFS basis by patients’ private insurance programmes. Assuta pays other physicians, such as radiologists and anaesthetists, on either a salaried or FFS basis. Similar arrangements are in place in many of the other profit-making hospitals.
Physician pay levels
According to OECD health database, Israeli physicians’ annual salaries have risen significantly in recent years (OECD, 2015). For example, for board-certified specialists employed by the Ministry of Health or Clalit, annual salaries have increased by approximately 50% (in dollar exchange rate terms) between 2010 and 2014. This rate of increase was unusual among the countries for which data are available.
The OECD data also suggest that Israeli specialists are currently reasonably well-paid in comparison with their counterparts in most OECD countries, both in dollar terms and relative to the average wage in the country. However, any international comparisons of income levels should be treated with great caution because of differences in measurement methodology and differences in tax rates (which in Israel are relatively high).
The new financial incentives
In 2011, major new financial incentives were put in place to encourage physicians to live and work in the periphery and to pursue careers in distressed specialties.
The agreement provided for an immediate 10% addition to the ongoing monthly salaries of residents working in the periphery, with the size of the addition increasing to 25% by 2013. Similarly, in the case of board-certified physicians, who are not hospital directors or deputy directors, the agreement provided for an immediate increase of 8%, growing to 17% by 2013.
The agreement also awarded one-time payments to all physicians who begin working in the periphery; the size of these payments is NIS 500 000 (about €125 000) in the case of distressed specialties and NIS 300 000 (about €75 000) in other specialties. Initially, the payments are awarded as interest-free loans, but if the physician remains in the periphery for a specified number of years, the loans are transformed into grants that do not have to be repaid. To put the size of these payments into perspective, it is worth noting that the average annual income of Israeli physicians is approximately NIS 300 000 (about €75 000) and the median is approximately NIS 240 000 (about €60 000).
Physicians working in distressed specialties (such as anaesthesiology), irrespective of where they work, also received substantial bonuses; some observers believe that these bonuses have reduced somewhat the power of the incentives created for working in the periphery.
The number of physicians applying for the bonuses has been substantially greater than originally anticipated, creating substantial budgetary pressure. As a result, by the end of 2014 the allocated budget of about NIS 700 million that had been planned to last until 2019 had been exhausted.
At the beginning of 2015, the Ministry of Finance agreed to allocate an extra NIS 75 million (about €18 million) for bonuses for residents only, for one more year. This sum is considerably lower than what had been spent per year in previous years. In accordance, the number of distressed specialties receiving a bonus has been reduced, and residents working in the periphery will not receive a bonus unless working in a distressed specialty (in which case their bonus will be higher than that of their colleagues working in the centre). The size of the payments will be decided in 2016, contingent on the number of residents who will be eligible for the bonuses.