-
14 December 2022 | Country Update
Review of hospital debts -
03 April 2019 | Country Update
The Ministry of Finance appoints budgetary supervisors to hospitals -
15 December 2018 | Country Update
Debt management and additional funding for hospitals the end of 2018 -
14 October 2018 | Country Update
Rising hospital debt: 46 billion HUF (142 Mill EUR) -
14 July 2016 | Policy Analysis
New yellow “lamp” is introduced in the on-line, social health insurance entitlement verification system
3.3. Overview of the statutory financing system
Hospital debts have been an ongoing financing and management issue of the Hungarian health system for a long time. In a nutshell, hospitals are often not able to make ends meet with the budget they receive for their operation. Thus, most hospitals follow a practice based on debt accumulation – repaid by the state at the end of the year – to maintain their services. Nonetheless, this practice does not solve the root cause of the issue, but rather encourages debt generation, which is in fact rewarded by this bailing-out policy. During the COVID-19 period, this became a low-priority issue due to the consequences of the pandemic (for example, lockdown measures, delayed diagnoses and interventions), but the pending energy crisis in the winter of 2022–2023 may bring the issue to the forefront again. At the end of 2022, the government allocated 19 billion HUF for this purpose, while the total hospital debt was estimated to be 60 billion HUF. In comparison, at the end of 2020, 80%, and at the end of 2021, 90% of the accumulated debt was covered.
According to Ildikó Horváth, the Secretary of State for Health, budgetary supervisors will be appointed to the most indebted hospitals. During the next five weeks, together with the management of the hospitals, the budgetary supervisors will review the expenditures and financial situation of the hospitals. As Ildikó Horváth said, they expected stronger management discipline from the hospitals on one hand, and on the other hand they planned to identify the main factors leading to the continued indebtedness.
In order to strengthen the supervision and governance of the hospitals, the Ministry of Human Capacities plans to set up a controlling and monitoring system. In addition, after the supervisor report, they would review the financing of the inpatient and outpatient care. Therefore, the budgetary supervisors will have to explore good practices and methodologies of the hospitals for more efficient operation in the future. The supervisors will be appointed and controlled by the Ministry of Finance to support Hospital Directors and Chief Financial Officers.
Authors
The methodology of the “usual” end-of-year debt
management changed in 2018. This year 55 billion HUF (175 million EUR)
will be distributed among public, municipal and church-owned health care
providers. However, since expired debts will rise to over 60 billion
HUF (191 million EUR) by December 31, the government will reallocate
about 30 billion HUF (95 million EUR) to cover the financial holes. In
addition, new incentives of 24 billion HUF (76 million EUR) will be
available to the healthcare providers to support quality of care and
financial management performance.
The Association of Medical Devices
Manufacturers (OSZ) is expecting the suppliers to receive payment for
their services in December. The amount of expired debt in total was
54.2 billion HUF (168 million EUR) at the end of October, and member
companies were affected by approximately 20 billion HUF (62 million
EUR).
Authors
References
According to the latest data of the Hungarian State Treasury (MÁK, end of September), the debts of Hungarian hospitals rose to about 46 billion HUF (142 Mill EUR). Compared to December 2017, the accumulated total debt increased by more than 30 billion HUF (92 Mill EUR), in average with 3.4 billion HUF per month (10,5 Mill EUR) Approximately half of the 46 billion HUF debt was overdue by more than two months, and about three quarters by more than one month. From the 4 billion HUF increase in September, about 3 billion HUF were overdue by 60 days. Hospital managers are intentionally generate some of this debt in the hope of getting a (more profitable)bail out by the end of the year, which has been a recurring measure by the government in recent years.
Authors
The Hungarian social health insurance system has a complex regulation of entitlement. Since 2007, entitlement has had to be verified by providers using an on-line system, based on the social insurance identification number of the patient. Until the 15th of July, 2016, the outcome of the verification process could fall into 4 categories (called „lamps”): green, red, blue and brown. The first two categories indicate a valid, while the last two a not valid social insurance identification number, the difference being that a patient with an invalid number is obliged to cover the costs of the services they utilised, either out-of-pocket or by insurance. Red “lamp” patients are still entitled to receive care under the Hungarian social health insurance system, but are obliged to clarify their entitlement with the Hungarian Tax and Customs Office (for instance by paying in any contribution arrears). A newly introduced yellow category will indicate those insurees, who are entitled to a limited set of health services only. This yellow category mainly affects foreigners, who gain entitlement through individual or inter-country agreements. In this category coverage takes effect only after the contribution has been paid for at least 24 months, or the amount of contribution, which has been paid in is equivalent to that total amount.
Authors
References
Official webpage of the National Health Insurance Fund Administration: http://www.neak.gov.hu/oldalak/nyelvi-oldalak/english
Government Decree No. 217/1997. (XII. 1.) Korm. Article 12/B, inserted by Government Decree No. 35/2007. (III. 7.) Korm. Article 1. for the on-line entitlement verification system
3.3.1. Coverage
In accordance with the constitution (1989/4), Act CLIV of 1997 on Health Care (1997/20) stipulates that every individual has the right to life-saving or preventive health care to avoid serious or permanent damage to his or her health, as well as to relieve any pain or suffering caused by sickness. Furthermore, every individual has a right to health services that are appropriate, continually accessible, equitable and regulated in a properly defined legal framework (1997/20) according to health status. However, Hungarian citizens and residents are not covered for health care treatment by subjective right, except for emergency or life-saving measures.
Currently, Act LXXX of 1997 on Those Entitled to the Services of Social Insurance and Private Pensions and on the Funding of These Services sets out the rules for participating in the health insurance system and defines entitlement to in-kind and cash benefits. Participation in the system is compulsory for all citizens living in Hungary (that is, people with a personal identification card); opting out is not permitted. As a general rule, Hungarian minorities living in neighbouring countries are not entitled to health services in Hungary, but this does not mean that they were denied access to care in the past. Since 2007, a special commission of the Ministry of National Resources evaluates applications by Hungarian minorities living abroad and defines the package of health services they are entitled to.
The population in Hungary is divided into three main groups: (1) insured individuals who are entitled to all services covered by the NHIFA and who pay regular contributions based on their income, (2) individuals who are entitled to medical services but are not required to pay contributions, and (3) all other inhabitants with a personal identification card and permanent residence, who are obliged to pay a medical service fee (that is, a fixed-amount insurance premium) on a monthly basis (1997/8). Foreigners who work in Hungary for a longer period are not obliged to participate but may do so if they wish.
According to the provision of the legal framework, Hungary should have 100% coverage, but the report of the NHIFA to the National Assembly in 2009 shows that the health insurance status of approximately 4% of the population is unclear (Ministry of Health, 2009a). Health services are provided on the basis of a social insurance identification number (Társadalombiztosítási Azonosító Jel; TAJ), which was initially issued to every citizen who applied for it. For many years, the regulation on contributions and their payment was not fully enforced: before 2006, patients could obtain health services simply by presenting the TAJ card to their health care provider, who was unable to check whether they still had a valid NHIFA registration and had actually paid the necessary health insurance contributions. In 2007, however, the government introduced a system to check the validity of the TAJ card. Providers have online access to the relevant database maintained by the NHIFA and can check the validity of the patient’s card ad hoc. Patients will receive necessary care even if their cards are not valid, but they will also be informed that their insurance registration status is unclear and they need to contact the NHIFA. The Tax Office is also notified about such cases for further processing and eventually collecting unpaid contributions retrospectively (2007/2). It is important to stress that necessary care cannot be denied to patients with unpaid contributions. As a result, population coverage is virtually universal.
Scope of coverage
Providing universal and comprehensive coverage was the founding principle of the previous, state-run socialist health care system. Health services were free of charge except for very small co-payments for medicines, medical aids and prostheses. Although this was inconsistent with the scarcity of resources, the problem was neither admitted nor addressed. Rationing probably occurred through queuing, implicit waiting lists, the dilution of services and informal payments.
In the early 1990s, government reforms placed greater emphasis on structural transformations than on setting priorities related to health care benefits. Parallel to the establishment of the HIF, a list of services to be covered was defined in amendments to Act II of 1975 on Social Insurance (1992/1). The benefit package was almost exhaustive, with the exception of aesthetic and recreational purposes (1992/7). The HIF does not offer benefits over and above those specified in the established benefits package.
The NHIFA offers services in kind to the insured and other entitled persons, as well as cash benefits to the insured (Table 3.2), including sick pay and child care and maternity benefits. The responsibility for funding disability pensions used to lie with the NHIFA but was transferred to the PIF in 2008. In contrast, the responsibility for funding the child care fee, which is available to parents until the child is 2 years old, used to belong to the central government but was transferred to the NHIFA in two steps, in 2007 and 2008. The HIF covers treatment abroad as long as individuals have (a) received permission from the NHIFA or (b) obtained this treatment in accordance with bilateral international treaties or the European Commission Regulation 883/2004, which deals with the provision of health care in EU Member States.
Before 2004, there was no systematic, formal or transparent process for deciding which services would be included in or excluded from the benefits package. With EU accession in May 2004, Hungary was obligated to adopt Council Directive 89/105/EEC. This regulation aimed to ensure that transparent measures are adopted by national authorities in the pricing and reimbursement of pharmaceuticals. Adopting this regulation, the government established the process of HTA to evaluate applications by pharmaceutical companies (2006/8). The NHIFA uses various criteria in the decision-making process, such as health needs, cost-effectiveness and budget impact (2004/4) in order to classify certain pharmaceuticals for different categories of reimbursement (see sections 2.7.2 and 2.8.4).
The first steps towards a less generous benefits package were taken during the economic crisis of 1995, when the HIF deficit led to calls for urgent action (see section 3.3.3). Act XLVIII of 1995 on the Amendments of Various Acts for the Purpose of Economic Stabilization subsequently curtailed both in-kind and cash benefits. The main item excluded from the benefits package was tooth-preserving dental services for adults. Subsidies for balneotherapy were also removed, a co-payment for patient transfer (i.e. ambulance) services was introduced, and sickness benefits were reduced (1995/5). In addition, employers became responsible for financing occupational health services (1995/8). The adverse effects of these measures – for example, a sharp drop in the use of dental services – forced the government in power from 1994 to 1998 to reconsider the exclusion policy and reintroduce dental services with some co-payments (1996/1) for adults. The next government abolished co-payments for tooth-preserving dental treatments in 2001, thus restoring the original situation (2001/10). Nevertheless, the share of OOP spending on dental services has remained very high, with total OOP expenditure in this category amounting to HUF 106 billion (€418.7 million) in 2007 and thus exceeding total NHIFA expenditure on dental services by a factor of five (OECD, 2010). OOP expenditure in this category represents 19.3% of the total private expenditure on health in Hungary.
Act LXXXIII of 1997 on the Services of Compulsory Health Insurance and related decrees define which health services are free of charge, which are covered but require some user charges, and which are excluded from HIF coverage. The Act defines a negative list based on the premise that, in principle, health services are covered and exclusions must be stipulated (1997/9). Also in 1997, new legislation on health and health insurance was enacted to address the issues of rationing and priority setting in a more systematic manner. Act CLIV of 1997 on Health introduced the concept of waiting lists and stipulated that waiting list priority must be assigned based on uniform and explicit criteria, taking into account patient health status (1997/20). Act LXXXIII of 1997 has made it possible to deviate from the waiting list order only in cases where both the reason for and the importance of the outcome of the intervention have been attested to officially (1997/9). Thus far, central waiting lists have been set up for organ and tissue transplantation and positron emission tomography/computer tomography (PET/CT) services, which are managed by the National Blood Supply Service (NBSS; Országos Vérellátó Szolgálat). Waiting lists for all other services are to be set up by the providers contracted by the NHIFA in the event of persistent shortages in the capacity to provide the necessary care (1997/9, 2006/9). Outpatient institutions must keep ordered lists of patient access (appointment lists), based on the priority of service provision dates that is established. Between 2007 and the first half of 2010, the waiting and appointment lists were supervised by the Health Insurance Supervisory Authority (HISA) (2006/10, 2006/14) and in certain cases by the NPHMOS. Then, upon abolition of the HISA, this task was partly transferred to the NHIFA (2010/9, 2010/10, 2010/11).
Depth of coverage
Co-insurance and co-payments are required for pharmaceuticals, medical aids and prostheses, balneotherapy, dental prostheses, treatment in sanatoria, long-term chronic care and some hotel services in hospitals. Co-payments are also due if:
- non-emergency specialist services are obtained without a referral from an authorized physician, normally the family doctor;
- patients choose to visit a provider other than the one they were referred to (see also section 2.9.2);
- patients desire more services than those prescribed by their physician (1997/9, 1997/18).
Special rules apply to a few services, such as infertility treatments, for which the number of attempts covered by HIF is limited (1997/16). The costs of medical examinations required to certify an individual’s fitness to drive or hold firearms are not covered (1997/18). Treatments for aesthetic or recreational purposes are explicitly excluded, as are those which have not proved effective in improving health. The latter include services that are not included in the International Classification of Procedures in Medicine, introduced in 1976 by WHO. In addition, cosmetic surgery, massage, abortion or sterilization without medical indication, and the prostate-specific antigen test for screening purposes are not covered (1997/9, 1997/14). Since 2007, treatment for injuries resulting from extreme sport activities and vaccinations that are not part of the government’s mandatory immunization programme are also not covered by public sources (1997/14).
3.3.2. Collection
General government budget
There is an increasing participation of the central government budget in financing the budget of the HIF, and the common assumption that countries with SHI rely predominantly on wage-related contributions to fund their health system no longer holds in Hungary.
According to the NHIFA, the total transfer from the central government budget, including deficit financing, is planned to be almost five times higher in 2010 (covering 47.5% of the HIF expenditure) than it was in 1997 (covering 10.9%). Hence the role of general taxes in funding of the HIF has become as important as the role of the wage-related contributions. From the perspective of the whole health care system, the share of tax funding among public sources was very high already in 2002 and 2003, when the share of tax funding (with 38.5%) exceeded the share of wage-related contributions (33.6%) in 2003, considering the deficit financing and hypothecated health care tax among tax sources in the budget of the HIF (Table3.4).
Table3.4
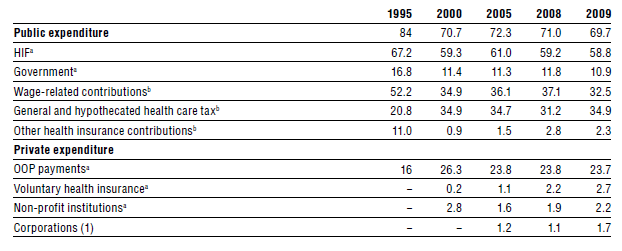
The hypothecated health care tax was introduced (1996/9) in 1997 to supplement the resources of the HIF and was initially paid by employers for each employed person as a lump sum (Table3.5). It was intended to compensate the HIF for social groups entitled to services but not paying contributions and the abolition of transfers from the PIF following the pension reform (1996/8, 1996/12). This measure had an insignificant impact on the resources of the HIF: as calculated by the authors based on NHIFA data, its share combined with the remaining contribution of the central budget (once the PIF transfer was abolished) reached 19.6% of the HIF budget for services excluding cash benefits in 1997 compared to 21.2% before the reform. This is an example of a change in the revenue mix without substantial impact on the overall income of the HIF budget.
Table3.5
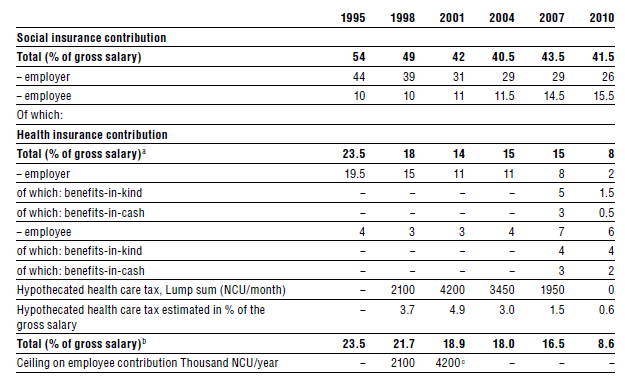
The government in power between 1998 and 2002 added a proportional component to the hypothecated health care tax as of January 1999. The 11% proportional tax was levied on types of income previously exempt from HIF contributions, such as dividends, in-kind allowances and letting property. Furthermore, the lump-sum component of the hypothecated health care tax was increased from HUF 1800 (€6.8) in 1997 to HUF 4500 (€17) in 2002. However, the government in power between 2006 and 2010 reduced it again to HUF 1950 (€7.7) in 2006, then abolished it completely in 2010. The proportional component is still in effect.
A new type of hybrid tax, the simplified contribution payment, was launched in 2005, applicable for persons or entrepreneurs working in the media or arts (2005/6) up to a certain income ceiling. Instead of the regular HIF contributions and income tax, the employees and employers in these occupational groups pay an overall (15% employee and 20% employer) contribution, which covers the entirety of their tax and social security obligations. Eleven percentage points of this employer contribution is earmarked as a health insurance contribution.
Among other public sources of financing are general and local taxes, other contributions for persons seeking employment and persons classified as being disadvantaged regarding employment, paid by the central government budget, as well as special taxes to be paid by pharmaceutical companies and wholesalers (2006/8). These revenue sources supplement the budget of the HIF to a small extent.
Collection of health insurance contributions
Since 1990, compulsory health insurance contributions have been the primary source of health care financing in Hungary (1989/6). The contribution is calculated as a percentage of gross wages and is therefore mildly regressive. It is determined by the National Assembly and split between employer and employee. In 2010, the HIF contribution amounted to 8% of an employee’s gross wages, with an employer share of 2% and an employee share of 6% (Table3.5). There used to be an upper threshold for the employee share of the contribution (1997/8), but this was eliminated in January 2001 (2000/8). In the third quarter of 2006, however, a minimum contribution base was introduced, which in 2009 amounted to two times the minimum wage.
Special rules apply to the self-employed, who must pay contributions either based on the activity-specific standard income set by the government in advance or on the official minimum wage. Small farmers either pay contributions based on the current minimum wage or, below a certain level of income, they pay health insurance contributions at 20% of their revenue and get benefits-in-kind but no cash benefits (1997/8). In order to qualify for more extensive benefits, they can choose to pay the full contribution rate (employer’s and employee’s combined) based on a special income statement to the Tax Office.
Provision for non-contributing groups has been shared between the social insurance system and the government since 1992: the central government pays the contributions for most of the non-contributing groups but not pensioners (1992/1). In reality, while payments by the PIF reached 20.2% of the expenditure on benefits-in-kind of the HIF, the contribution of the central budget for the non-contributing groups only amounted to 1%, which made practically no difference in the budget of the HIF (NHIFA, 2008).
Unpaid HIF and old age insurance contributions combined peaked at 4.3% of GDP in 1994, but still amounted to 2.5% of the GDP in 2000. In fact, some authors estimate a shadow economy of 25.1% of GDP in Hungary, which is at the lower end of the range for transition economies of central and Eastern Europe, but higher than in Slovakia and the Czech Republic, as well as than the average for OECD countries (Schneider & Klinglmair, 2004).
High HIF contribution rates have certainly provided an incentive for avoidance and evasion, including payment arrears, non-payment and under-reporting of income. Successive governments have attempted to address these problems in several ways. The interventions had three main directions: decreasing the HIF contribution rate, widening the contribution base and stronger enforcement of the payment of contributions.
In 1996, the HIF contribution of the employers was decreased by three percentage points, which was the starting point of an enduring trend in the radical decrease of the employer contribution rate coupled with the more rapidly increasing deficit of the HIF, throughout the following decade. This policy aimed at improving international competitiveness, boosting economic growth and stimulating the employment level. The potential consequences on HIF revenue were not addressed in a systematic manner.
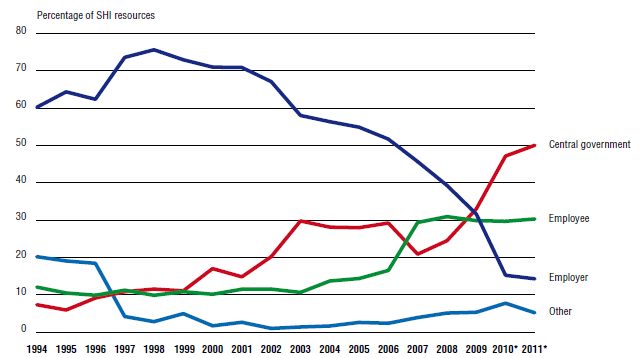
In 1998, contribution rates were decreased further and contribution collection was transferred from the NHIFA to the more authoritative Tax Office, with the aim of making collection less susceptible to tax avoidance, whereas the governance structure of the HIF and NHIFA were reorganized. The employer share of contributions was decreased by another four percentage points to 11% in 1999 (and remained at this level until 2006), while the employee contribution had been lowered by 1% in 1998 (Table 3.5). The government abolished the ceiling for the employee health insurance contribution (2000/8) and added a proportional component to the hypothecated health care tax (see above). The government in power between 2002 and 2006 basically upheld this policy as did the next administration, which further reduced the employer contribution rate from 11% in 2006 to a symbolic 2% in 2010. At the same time, the employee contribution rate increased from 4% in 2006 to 6% in 2010. Over the last 15 years, this policy has resulted in a steep increase in the ratio of employee to employer contribution shares. In the late 1990s, employers provided 75.6% and employees 9.9% of HIF revenue, whereas, in 2011, shares are expected to be around 14.3% and 30.3% respectively, with a parallel increase of the share of the central government to 50.1% (Fig3.6).
Fig3.6
It was expected that increased employment would shrink the shadow economy and increase HIF revenues. Defending their law amendment (2009/5) which decreased the employer contribution rate by three percentage points in 2009, the government argued that a one percentage point decrease in the contribution rate would increase employment by 0.15%. However, evidence from the employment database of the HCSO (HCSO, 2010c) shows that the employment ratio of the population in the 15–64 age group increased from 53.6% in 1998 to 56.0% in 2000 and to 56.7% in 2008, that is, the employment ratio increased only by 3.1% between 1998 and 2008 and by 0.7% between 2000 and 2008. Thus, despite the efforts and measures by successive governments, up to 2010 the level of employment remains nearly as low as in the late 1990s.
Overspending in the pharmaceutical budget, high unemployment and decreasing real wages certainly contributed to the persistent fiscal instability of the HIF, at least in the early phase of economic transition, but the evasion of health insurance contributions stemming from the size of the shadow economy and the substantial, uncompensated decrease of the contribution rate seem to be the core weaknesses of the revenue collection function since the mid-1990s.
3.3.3. Pooling of funds
Although the collection and pooling functions are separated from each other in the Hungarian system of health financing, there is no complicated mechanism to distribute resources from the collecting agency (the Tax Office) to the main pooling agency (the NHIFA), the latter of which is also the single payer in the health insurance system. The Tax Office must transfer the collected payments on a daily basis to the account of the HIF, which is administered by the Treasury, and has to report on the outcome of the collection regularly to the NHIFA (1998/27). Given that there is a single National Risk Pool, no risk-adjusted allocation methods are applied.
The annual process of setting the HIF budget is administered by the Ministry of National Economy,[13] which starts planning by issuing detailed guidelines to the other ministries and government agencies by mid-April in a given year. These include target numbers for the sub-budget level of HIF expenditures and other macroeconomic parameters. The planning process follows a top-down approach, in which needs assessment plays a fairly limited role, while target numbers for the next year are based on the current year, without taking into account realistic calculations of the cost of services in the benefits package. The final version of the budget approved by the government for HIF expenditure in the 2010 financial year differed only slightly from the one originally proposed by the Ministry of National Economy, underlining the weakness of the Ministry of National Resources to influence budget allocation for health. The NHIFA does not bear financial responsibility for any imbalance in the HIF budget and the state has to cover expenditures even if they exceed revenues (1975/1, 1997/8).
The Ministry has been planning the HIF budget with a substantial deficit since 2003. The fact that this has been possible highlights the irregularity of state budget planning regulations. The same regulation stipulates that, when financial data analysis and the trends in the macroeconomic context and HIF expenditures forecast fiscal imbalance, the government is obliged to prepare recommendations to the parliament for ensuring financial stability through increasing revenue, decreasing expenditure or modifying the scope (breadth, depth or height) of benefits (1992/1, 1997/8). Subsequent governments have failed to address the chronic imbalance of the HIF budget in a systematic and transparent manner.
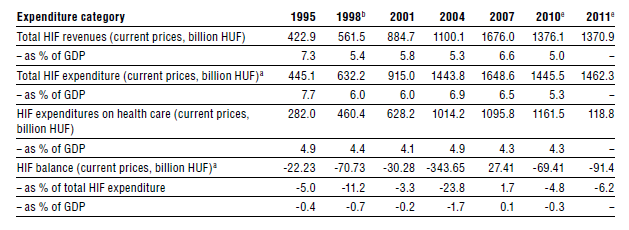
Since the inception of the HIF, its expenditures have always exceeded its revenues with the exception of some fiscal years (1995, 2007 and 2008). This gap has been covered retrospectively at the end of each fiscal year through deficit financing by the government budget. HIF revenues decreased from 7.8% of the GDP in 1993 to 5.5% of the GDP in 2005 (see also Table3.6), while expenditures only fell from 8.5% to 7.2%. The gap between revenues and expenditures peaked in 2005 at 23.8% of total HIF expenditure (amounting to HUF 375 billion or €1.48 billion or 1.7% of GDP). The peculiarity of the budget management stewardship by the Ministry of National Economy is illustrated by the fact that 91% of the gap between revenues and expenditures in 2005 was a planned deficit approved by parliament in 2004 (NHIFA, 2008), while the rest was due almost exclusively to overspending in the pharmaceutical sub-budget. As a result of effective cost-containment measures since 1997, such overspending was not apparent in the inpatient and outpatient health services sub-budgets.
Table3.6
The sudden improvement in the balance of the HIF budget in 2007 and in 2008 was the result of the combined effect of a change in budget planning and of measures to contain pharmaceutical expenditures. First, the parliament decided to reintroduce the obligation of the central budget to pay a certain amount of contributions on behalf of the non-contributing groups by means of the newly established National Risk Pool, leaving the hypothecated health care tax, which has the same goal, intact. This measure, as in 1997, did not increase the financial resources of the HIF, since this budget transfer was calculated to eliminate the planned deficit of the HIF budget. Thus, only the timing and legal form of the central budget contribution changed, but not its amount. The strict cost-containment measures introduced in 2007 have yielded concrete and measurable results in decreasing the overspending of the pharmaceutical sub-budget of the HIF, although this was mainly achieved by increasing patient cost-sharing (2006/9).
While most public revenues are pooled by the HIF, there is some pooling fragmentation. The central and local governments are responsible for capital costs of providers and different municipalities may allocate more or less to health care facilities. This causes great variation in the physical infrastructure quality of the health service delivery system. Richer municipalities usually have better facilities, some poorer municipalities have accumulated debt in order to maintain a proper infrastructure, while others have simply ignored this obligation due to lack of funding. Any debts accumulated by local governments add to the overall government budget deficit, forcing the central government to formulate stricter regulations on the level of debt local governments are allowed to accumulate. Although the central government provides grants to support the development of infrastructure by municipalities, there is no explicit strategy for reducing the inequalities created by this fragmented pooling and resource allocation arrangement.
- 13. Before the reorganization in 2010 the Ministry of Finance. ↰
3.3.4. Purchasing and purchaser–provider relations
The organizational relationship between purchaser and providers is based on a contract model since 1990, when the NHIFA was established and the ownership of most public health care facilities was transferred to local governments (1990/1). Although the NHIFA is a single payer with a monopsonistic market power, it has very limited discretion over purchasing decisions, for example to set the terms of the contract and to contract selectively with providers. The National Assembly and the government regulate the most important elements of the provider contract in acts and decrees, including reimbursement price, capacities, quantity of outputs, payment methods and financing of capital costs. As pointed out in published comparative literature, active contracting does not actually take place in Hungary, but is often a formality for establishing the basis for provider reimbursement (Figueras, Robinson & Jakubowski, 2005).
On the one hand professional associations do not have negotiation rights on prices and outputs in the contractual process, on the other hand the NHIFA is obliged to contract the providers that are selected or approved through the capacity regulation processes of the government (see also section 2.8.2). Similarly, family doctors, who are for the most part private entrepreneurs, contract with the local government to provide services for the local population, and the NHIFA is obliged to conclude a payment contract with all those family doctors who have a local government contract. Physicians working in outpatient and inpatient facilities are mostly salaried employees and not contracted separately by the NHIFA, although they do have a contract for the outpatient prescription of pharmaceuticals (for the role of the NHIFA regarding pharmaceuticals see section 2.8.4).
Institutional health service providers have to contract with the NHIFA in order to become eligible for reimbursement. The contract defines provider capacities in terms of outpatient specialist consultation hours, and acute and chronic hospital beds. Based on these contracts, individual health care providers are then reimbursed from the sub-budgets by various methods of payment: family physicians are paid by adjusted capitation, outpatient specialist services by fee-for-service points, and acute and chronic inpatient services by HDGs (Homogén Betegségcsoportok, HBCs) and patient-days respectively. Until 2001, contracted capacities were determined per county and specialty by law according to a special formula of local health needs (on the basis of certain socioeconomic indicators of the local population), while the county consensus committees agreed on the distribution of contracted capacities across individual health care providers (1996/4). In 2001, Act LXIII of 1996 was repealed, and the actual contracted capacities became the basis of future contracting (2001/5). The law allowed greater flexibility for local governments to downsize and restructure capacities. At the same time, capacity extensions had to be approved by the then Ministers of Health and Finance. In 2006, the new government froze provider capacities on 31 December 2006, then downsized and restructured inpatient capacities (2006/12) (see more detail in 2.8.2).
As mentioned above, the NHIFA is not allowed to engage in selective purchasing, and its contracting process is not based on systematic health needs assessment. It has to contract with all providers who have a territorial supply obligation. Until 2007 the quantity and quality of outputs were not stipulated in the contract, except for a few high-cost, high-tech interventions, like liver transplantation, for which the annual number of procedures was set in advance. Since the beginning of 2004, the government has set output limits for inpatient and outpatient care by defining the number of HDGs and fee-for-service points, which are paid for by the NHIFA, for each health care provider (see also section 3.7). Above the set quantities health care providers receive no additional payment. Quality control, on the other hand, is a task of the NPHMOS. The NHIFA has the right to monitor contracts, mainly by controlling the validity of providers’ reports on output.
Private providers contracted by the NHIFA are family physicians, pharmacies, pharmaceutical wholesalers and traders, and providers of certain diagnostic services and kidney dialysis, dental care services, patient delivery transport services, district mother and child nurse and school health services, as well as a few outpatient specialist care and inpatient care providers. This latter group includes hospitals owned by churches or charities, which are fully integrated into the publicly financed health insurance system. There is one private profit-making hospital contracted only for the provision of same-day surgical procedures.
The participation of private providers in health service delivery in Hungary started with the dialysis services in the early 1990s, followed by diagnostic services as of 1996. Private providers were initially involved in the outsourcing of various types of medical services and then increasingly in ancillary services, such as laundry, catering, accounting and performance reporting. However, since the mid-2000s, the entire management of hospitals and outpatient specialist providers (polyclinics) can be subject to outsourcing (functional privatization, i.e. when only the management of the service provider has been contracted out).
The management of hospitals owned by local governments has been contracted out in many cases. Contracting out the provision of certain services and management is a widespread phenomenon, which started in the mid-1990s and has been evolving towards the corporatization of providers. Thus, a large number of private providers, with varying scopes and levels of services, can take part in the provision of health care services without a formal contract with the NHIFA. In the case of functional privatization, the private management company takes over NHIFA contracting from the local government, which remains the owner of the facilities. In hospital care, the first concession contract for operating a hospital was signed in 2004 and more followed. However, the flagship actor in the private health industry (Hospinvest) declared bankruptcy in 2009 and returned management rights to the owners, that is, the respective local governments, causing intensive public and media debate across the country. Its failure was a serious blow to the functional privatization model.
In 2009, the State Audit Office published a study on the contracting out of hospital services and on concession contracts for operational rights. The report concludes that in most cases the outsourcing process has been determined by private companies rather than by public authorities (State Audit Office, 2009b).