-
31 March 2025 | Country Update
Robert Fitzgerald Kennedy Jr. is confirmed as Secretary of U.S. Department of Health and Human Services -
01 May 2023 | Policy Analysis
Private Equity in US Health Care
2.2. Organization
On 13 February 2025, Robert Fitzgerald Kennedy Jr. was confirmed as Secretary of the Department of Health and Human Services, responsible for public health and biomedical research agencies such as the Centers for Disease Control and Prevention (CDC), the Food and Drug Administration (FDA) and the National Institutes of Health (NIH).
Under a motto of “Make American Healthy Again”, Kennedy holds controversial views on several health policies. Foremost is his view on vaccination. Although he denies being against vaccination, Kennedy holds that vaccines are not safe, and he blames them for causing autism, an association that has been disproven. He considers COVID-19 vaccines to be the most unsafe, and he unsuccessfully petitioned the FDA to revoke approval. He is founder and former chair of the Children’s Health Defense, a major anti-vaccination organization.
Already his anti-vaccination sentiment has led to fewer vaccinations, and parts of the United States are experiencing a measles outbreak. This has prompted “qualified support” from Kennedy that falls short of urging the public to get vaccinated. Instead, he promotes alternative, unproven treatments.
Kennedy postponed the meeting of CDC’s advisory committee on immunization, which makes recommendations to the CDC about vaccines, and he plans to change committee membership. Kennedy wants to focus on “informed consent” in the vaccination process, which may mean focusing on the potential risks of vaccines and downplaying their benefits. He has canceled a flu vaccination advertising campaign that has been running since 2023. More generally, Kennedy wants to reprioritize funding from infectious to chronic diseases.
For the most part Kennedy has not opposed Trump’s executive order reducing HHS funding, including lowering NIH funding and cutting CDC and FDA staffing. Regarding the FDA, Kennedy is looking at changing membership on committees that advise the FDA.
Kennedy’s confirmation has been opposed by much of the medical community. Led by a by a progressive advocacy group, 18,000 physicians signed a letter opposed to his confirmation. Public health officials, practitioners, and organizations have also publicly expressed opposition. The American Public Health Association has issued public statements and letters to Congress.
Authors
References
https://www.apha.org/news-and-media/news-releases/apha-news-releases/2024/rfk-jr-hhs-nomination
Burki, T. (2025). Robert F Kennedy Junior-how concerned should we be? The Lancet. Infectious Diseases, 25(1), e19–e20. https://doi.org/10.1016/S1473-3099(24)00825-9
Dyer, O. (2025). Robert F Kennedy cancels flu vaccination ad campaign and key vaccine policy meeting. BMJ (Clinical Research Ed.), 388, r389. https://doi.org/10.1136/bmj.r389
Dyer, O. (2025). Robert F Kennedy Jr offers qualified support for MMR vaccine as measles spreads across US and Canada. BMJ (Clinical Research Ed.), 388, r454. https://doi.org/10.1136/bmj.r454
Jaffe, S. (2025). Robert F Kennedy Jr’s promises. Lancet (London, England), 405(10480), 684–685. https://doi.org/10.1016/S0140-6736(25)00398-8
Tanne, J. H. (2025). Robert F Kennedy is likely to be confirmed as head of US health department after contentious committee vote. BMJ (Clinical Research Ed.), 388, r259. https://doi.org/10.1136/bmj.r259
Wise, J. (2025). Over 18 000 doctors urge Senate to reject Robert F Kennedy Jr as health secretary. BMJ (Clinical Research Ed.), 388, r60. https://doi.org/10.1136/bmj.r60
In 2021, private equity (PE)—groups of investors that use large unregulated pools of money to buy into and restructure companies—put $206 billion into 1,400 U.S. health care acquisitions. PE currently owns 4% of U.S. hospitals, 11% of nursing homes, and 2% of doctor’s offices. It is infiltrating other health care sectors such as home care, urgent care, psychiatric facilities, addiction treatment centers, dental offices, eye clinics, and clinical trials. It also is building a presence in the Accountable Care Organization’s “REACH” program.
PE has a goal of acquiring quick financial gain with little commitment to the organization being purchased. It typically accomplishes its quick returns by assigning debt to the practices it buys, cutting labor costs, changing services to the most lucrative ones, upcoding charges, merging or shutting practices, then selling the facilities within 3–7 years and/or letting them go bankrupt.
Due to this behavior, PE has been shown to have negative effects on the quality of, access to, and cost of health care. Regarding health care quality, PE cuts staff, lowers licensed to unlicensed staffing ratios, and does not adequately train staff, resulting in inadequate numbers of staff with adequate education and training. It also reduces services and supplies. The negative effects of these practices on the quality of care can be seen in emerging research. Recent studies have found that being admitted to a PE-owned nursing home increases the short-term probability of death by about 10% and increases rate of emergency department visits by 11% and hospitalizations by 4%.
PE debt financing results in financially stressed hospitals and hospital closures, which reduces access to care. Hospital closures often involve rural and underserved areas. One example is that of Hahnemann Hospital, which served low-income residents in Philadelphia. PE sold Hahnemann assets with the profits going back to the investors, while the hospital incurred the debts and eventually had to declare bankruptcy and close in 2019.
In contrast to inadequate access to care, PE encourages overtreatment of patients, which leads to safety and quality issues. This has become most apparent in dental care, where PE-owned dental centers have been found to perform unnecessary dental procedures, such as root canals for babies.
PE increases health care costs by increasing the number of services (churn), upcoding the charges for services, charging surprise bills to patients, and engaging in kickbacks.
PE has a record of fraudulent activities. Companies owned or managed by PE were fined more than $500 million since 2014 to settle at least 34 lawsuits filed under the False Claims Act.
What should be done about the growth of PE? Some believe that PE does not belong in health care, implying a ban on all private equity. Don Berwick, a physician long involved in health care quality improvement, puts the onus on health care professionals to “become noisier about the conflict between unchecked greed and the duty to heal”. If not fully banned, PE could be regulated. However, there are currently not many ways to regulate it. One way, through antitrust laws, isn’t effective since PE typically acquires practices and hospitals below the $101 million threshold that triggers an antitrust review. Some possible additional regulations could be:
- eliminate tax advantages,
- change coding and billing rules,
- limit the debt imposed on health sector companies,
- control consolidation and monopolies in the health sector,
- utilize the False Claims Act more to prosecute fraud,
- reform bankruptcy laws to assign liability to investors, and
- regulate mergers, closings, and sales of health care facilities.
Authors
References
Berwick, D. (2023). Salve Lucrum: The Existential Threat of Greed in US Health Care. JAMA, 30 January 2023.
Braun RT, Jung HY, Casalino LP, Myslinski Z, Unruh MA. (2021). Association of Private Equity Investment in US Nursing Homes With the Quality and Cost of Care for Long-Stay Residents. JAMA Health Forum. 19 November 2021; 2(11):e213817.
Gupta, et al. (2021). Does Private Equity Investment in Healthcare Benefit Patients? Evidence from Nursing Homes. NBER working paper 28474, February 2021
Lavietes, MH & Rosenthal, E. (2022). Accountable Care’s Reach in Medicare. NEJM, 387:14, 1339–1340.
Matthews S, Roxas R. (2022). Private equity and its effect on patients: a window into the future. Int J Health Econ Manag. 23 May 2022:1–12.
Singh Y, Song Z, Polsky D, Bruch JD, Zhu JM. Association of Private Equity Acquisition of Physician Practices With Changes in Health Care Spending and Utilization. JAMA Health Forum. 2 September 2022; 3(9):e222886.
Schulte, F. (2022). Sick Profit: Investigating Private Equity’s Stealthy Takeover of Health Care Across Cities and Specialties. Kaiser Health News, 14 November 2022, Patients for Profit: How Private Equity Hijacked Health Care https://khn.org/news/tag/patients-for-profit
Young, Kerry Dooley. (2022). The impact of private equity ownership in health care: A research roundup and explainer — Plus 3 reporting tips https://journalistsresource.org/home/private-equity-ownership-in-health-care-research
2.2.1. Overview
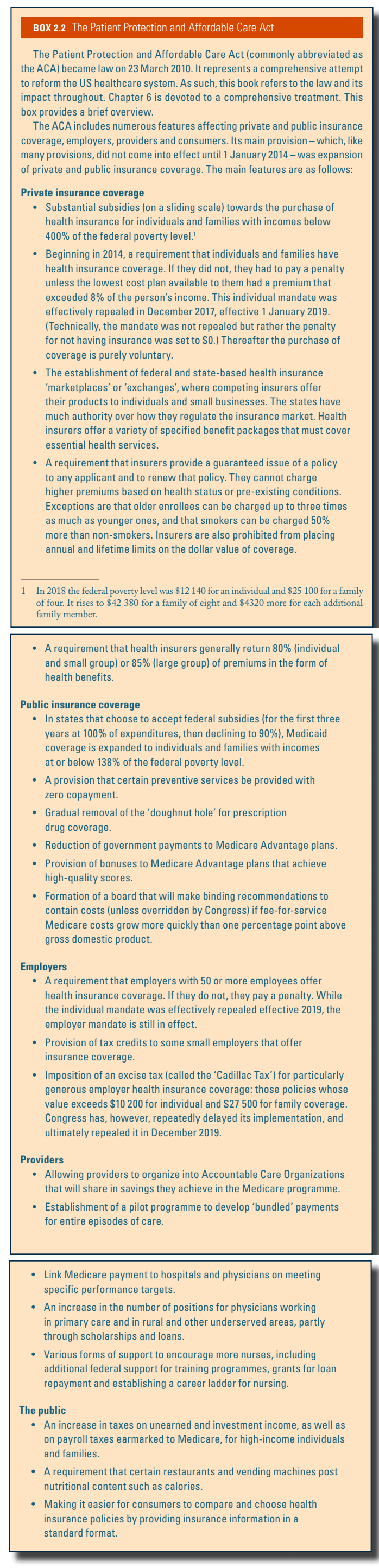
In the US health care system public and private payers purchase health care services from providers subject to regulations imposed by federal, state and local governments as well as by private regulatory organizations. Fig2.1 illustrates the interplay between four main actors: (1) government; (2) private insurance; (3) providers; and (4) regulators, as well as the types of relationship that connect them. The Patient Protection and Affordable Care Act, more commonly referred to as the Affordable Care Act (ACA), signed into law on 23 March 2010, resulted in several significant changes in the US health care system (see Box2.2 and Chapter 6 for more details). Fig2.1 shows what the US health care system looked like in 2020.
Fig2.1 | Box2.2 |
 |  |
Government, insurers, providers, and public and private regulators each play an important role in the US health care system. Government actors include those at the federal, state and local levels. Both the federal and state governments have executive, legislative and judicial branches (although the figure only shows this under the federal government). Under the executive branch of the federal government, the Department of Health and Human Services (HHS) plays the largest administrative role in the US health care system. HHS includes agencies such as the Centers for Medicare and Medicaid Services (CMS) that administer the public Medicare and Medicaid programmes, and the Children’s Health Insurance Program (CHIP). Other selected agencies within HHS include the Agency for Healthcare Research and Quality (AHRQ), the Centers for Disease Control and Prevention (CDC), the Food and Drug Administration (FDA) and the National Institutes of Health (NIH).
The Office of Veterans Affairs (VA), which oversees the Veterans Health Administration (VHA) to provide care to military veterans, is a federal agency independent of HHS. The Department of Defense is in charge of providing health care to active duty military and their families through TriCare. The Indian Health Service is a federal-level health system, within the HHS, that provides health services to members of federally recognized tribes of Native Americans and Alaskan Natives.
Public purchasers include federal and state agencies. The public purchaser that spends the most is Medicare. The programme provides nearly universal coverage for Americans aged 65 and older, the disabled and those with end-stage renal disease. State governments, along with funds provided by the federal government, finance health care services through Medicaid and CHIP. Both programmes are state administered and primarily cover low-income families. Medicaid also covers disabled adults, long-term care services after individuals have used up their own income and assets, and, along with Medicare, low-income seniors (these programmes are discussed in more detail in sections 3.3.1 and 3.3.2).
Both state and local government are also involved in health care in a number of ways that make it possible for low-income and other disadvantaged individuals and families to obtain care. These include such functions as operating public hospitals, providing medical and preventive services through state and local health departments and their associated clinics and community health centers (CHCs), as well as other public health activities including regulating restaurant safety.
In addition to government purchasers, private insurers and individuals also purchase health care in the United States. Private insurance falls predominantly into three categories: HMOs, PPOs and high-deductible plans (see section 3.5 for more details) (Claxton et al., 2019). The vast majority of Americans with private insurance obtain it through an employer, though 16.2% have individually purchased coverage. In 2016 there were roughly 28.2 million people living in the United States without any health insurance, constituting 8.8% of the total population (US Census Bureau, 2016a). Federal and state-based insurance marketplaces (also known as ‘exchanges’) began effective January 2014 under the ACA for individuals without access to employer-based insurance and small employers that choose to purchase coverage.
Health services for the uninsured and those on Medicaid are often provided by a safety-net system of public and community clinics, as well as by hospitals and physicians.
The categories of health care providers and services mirror those of other high-income countries and include hospital, physician, dental, prescription drug, home health and long-term care, mental health, other professional, and public health services. The ACA encouraged providers, organizing them into Accountable Care Organizations (ACOs), to share in savings they achieve in the Medicare programme. ACOs sharing responsibility for the health, provision of health care services and costs of Medicaid populations and those with private insurance also exist in the United States.
Regulation of the US health care system, which is discussed in more detail in section 2.7, occurs at three levels: federal, state and private. Much of the regulation at the federal level comes under the HHS. Fig2.2 presents the organization of the regulatory bodies within HHS, which oversees programmes, issues regulations and carries out federal government policy on a number of health care and related matters.
Fig2.2

2.2.2. Federal and state government organizations
The President names the heads of major health agencies at the national level with the consent of the Senate. Governors play the same role in their respective 50 states. These individuals set the agenda, make policy and supervise the implementation of health laws and administrative orders. When a new President is elected, substantial changes may take place at the highest level of leadership in US public health sector organizations. New offices and administrative agencies are sometimes added, and, on occasion, some agencies are eliminated. This reflects the different policy priorities of the newly elected President. Career civil servants are numerous and carry out most of the work. They may serve under department or division heads with quite different priorities over the term of their employment. Congress can also play an administrative role as a legislative body. Those employed in various branches of government receive instruction from the members of Congress who oversee their work. This system works the same way at the state and local levels, where a new governor, new state legislature, new mayor or new local governing board can initiate substantial change.
HHS is the key health agency in the United States. It has broad responsibilities for carrying out the instructions of the Congress and the administration regarding finances, planning/coordination, administration and regulation, as well as the provision of health services. The agency’s head carries the title of “Secretary” and is named by the President with the consent of the Senate. He or she also sits in the President’s Cabinet. HHS has a budget of about 28% of all federal outlays with over 80 000 employees (OMB, 2018). Its various components administer grants and provide/purchase health insurance for about one-third of the population. HHS coordinates and monitors the performance of many state and local health organizations. The financing for many programmes that are jointly administered at the federal government, state and local level flows through HHS. The department includes more than 100 programmes across 11 operating divisions, covering a wide spectrum of activities. These programmes not only provide services nationwide but also enable the collection of national health and other data (US Department of Health and Human Services, 2018).
Key government organizations within HHS include the following (see Fig2.2).
Fig2.2
- CMS is by far the largest agency in HHS because it administers the Medicare, Medicaid and CHIP programmes, which cover about 140 million Americans. It has about 6000 employees and an annual budget on various coverage programmes and agencies of approximately USCMS is by far the largest agency in HHS because it administers the Medicare, Medicaid and CHIP programmes, which cover about 140 million Americans. It has about 6000 employees and an annual budget on various coverage programmes and agencies of approximately US$ 1 trillion in 2018.
- AHRQ focuses on comparative effectiveness, quality improvement and safety, health information technology, preventive and care management, and health care value. It is generally viewed as the main federal government agency that focuses on health services research, although many other organizations address health services. As of 2018, AHRQ had a budget of approximately US$ 321 million.
- The CDC works with partner organizations to accomplish its mission through such areas as health monitoring, prevention research, promotion of healthy behaviours, and fostering safe and healthful environments. Its 2018 budget was nearly US$ 8.3 billion.
- The FDA is responsible for ensuring the safety, efficacy and security of human and veterinary drugs, biological products, medical devices, food supply, cosmetics and products that emit radiation. It also regulates tobacco manufacturing, marketing and distribution, with a special interest in reducing tobacco use by minors. Its 2018 budget was approximately US$ 5.4 billion.
- The NIH fosters fundamental discoveries, developing resources to prevent disease and promoting scientific integrity. NIH has within it about two dozen institutes and centres, examples of which are the National Cancer Institute, the National Institute on Aging, the National Heart, Lung, and Blood Institute, and the National Library of Medicine. Its 2018 budget was approximately US$ 36.2 billion.
- The Indian Health Service, also under HHS, serves nearly 2 million individuals with an annual budget of about US$ 6.1 billion in 2018, and is funded through federal government general revenues.
Congress is also advised by several federal organizations, including the Congressional Budget Office (CBO) and Medicare Payment Advisory Commission (MedPAC). The CBO produces non-partisan analysis to Congress to support its budget process. CBO reports provide independent analysis to inform the health policy process. MedPAC is an independent body that advises Congress on payments to private health plans, FFS providers, and access and quality of care issues related to the Medicare programme.
The VHA is operated by the US Department of Veterans Affairs. It covers 9 million veterans at 1200 sites across the country, including approximately 170 medical centres, employing more than 300 000 people, and including over 100 academic health systems (US Department of Veterans Affairs, 2018). Spending on VHA medical care exceeded US$ 70.6 billion in 2016 and is covered through general federal government revenues. TriCare – financed through federal general revenues – pays for civilian health services used by active military and their families and some retirees, serving almost 10 million people. Generally, services must be received through the programme’s managed care networks, and require modest premiums and co-payments. Total spending on military care was about US$ 60 billion in 2016 (US Department of Veterans Affairs, 2018).
Public health organizations exist at every level: national, state, county and city. Public health functions are carried out by administrative units in diverse parts of the governmental organizations. The CDC, an HHS agency, is a principal component. Another example is the Commissioned Corps of the United States Public Health Service, headed by the Surgeon General. The public health services are organized as a military unit with a Commissioned Corps of 6500 that includes uniformed service and rankings that parallel military lines. Members of the United States Public Health Service Commission Corps serve throughout the various offices and agencies in HHS, as well as the Environmental Protection Agency and the United States Departments of Defense, Agriculture and Homeland Security.
Each of the main public health systems in the United States has a complex set of structural arrangements. Some health programmes, such as Medicaid, are organized and administered differently in each of the states, which makes it difficult to cover them in any depth here. Medicare is examined in some detail because it is a national programme.
The Social Security Administration (SSA) makes the initial determination as to whether or not an individual who applies for Medicare fulfils the eligibility requirements. The SSA also arranges for premiums to be withheld from the participant’s Social Security benefit cheque and determines an individual’s premium level, as these differ depending on the beneficiary’s income. In addition, the SSA maintains the database for Medicare in conjunction with its own records. The Internal Revenue Service (IRS), which is part of the United States Department of the Treasury, collects Medicare payroll taxes from workers and their employers. IRS data from an individual’s tax return are used to determine eligibility for income-adjusted Medicare subsidies (Klees, Wolfe & Curtis, 2009).
One critical issue is that US government health care system organizations overlap, and programmes between the various actors in Fig2.1 sometimes duplicate one another. This can result in both care coordination problems as well as gaps in services, in particular coverage areas and redundancies in other areas, which can be confusing to patients and providers.
Fig2.1
nbsp;1 trillion in 2018.
Congress is also advised by several federal organizations, including the Congressional Budget Office (CBO) and Medicare Payment Advisory Commission (MedPAC). The CBO produces non-partisan analysis to Congress to support its budget process. CBO reports provide independent analysis to inform the health policy process. MedPAC is an independent body that advises Congress on payments to private health plans, FFS providers, and access and quality of care issues related to the Medicare programme.
The VHA is operated by the US Department of Veterans Affairs. It covers 9 million veterans at 1200 sites across the country, including approximately 170 medical centres, employing more than 300 000 people, and including over 100 academic health systems (US Department of Veterans Affairs, 2018). Spending on VHA medical care exceeded US$ 70.6 billion in 2016 and is covered through general federal government revenues. TriCare – financed through federal general revenues – pays for civilian health services used by active military and their families and some retirees, serving almost 10 million people. Generally, services must be received through the programme’s managed care networks, and require modest premiums and co-payments. Total spending on military care was about US$ 60 billion in 2016 (US Department of Veterans Affairs, 2018).
Public health organizations exist at every level: national, state, county and city. Public health functions are carried out by administrative units in diverse parts of the governmental organizations. The CDC, an HHS agency, is a principal component. Another example is the Commissioned Corps of the United States Public Health Service, headed by the Surgeon General. The public health services are organized as a military unit with a Commissioned Corps of 6500 that includes uniformed service and rankings that parallel military lines. Members of the United States Public Health Service Commission Corps serve throughout the various offices and agencies in HHS, as well as the Environmental Protection Agency and the United States Departments of Defense, Agriculture and Homeland Security.
Each of the main public health systems in the United States has a complex set of structural arrangements. Some health programmes, such as Medicaid, are organized and administered differently in each of the states, which makes it difficult to cover them in any depth here. Medicare is examined in some detail because it is a national programme.
The Social Security Administration (SSA) makes the initial determination as to whether or not an individual who applies for Medicare fulfils the eligibility requirements. The SSA also arranges for premiums to be withheld from the participant’s Social Security benefit cheque and determines an individual’s premium level, as these differ depending on the beneficiary’s income. In addition, the SSA maintains the database for Medicare in conjunction with its own records. The Internal Revenue Service (IRS), which is part of the United States Department of the Treasury, collects Medicare payroll taxes from workers and their employers. IRS data from an individual’s tax return are used to determine eligibility for income-adjusted Medicare subsidies (Klees, Wolfe & Curtis, 2009).
One critical issue is that US government health care system organizations overlap, and programmes between the various actors in Fig2.1 sometimes duplicate one another. This can result in both care coordination problems as well as gaps in services, in particular coverage areas and redundancies in other areas, which can be confusing to patients and providers.
Fig2.1
nbsp;321 million.
Congress is also advised by several federal organizations, including the Congressional Budget Office (CBO) and Medicare Payment Advisory Commission (MedPAC). The CBO produces non-partisan analysis to Congress to support its budget process. CBO reports provide independent analysis to inform the health policy process. MedPAC is an independent body that advises Congress on payments to private health plans, FFS providers, and access and quality of care issues related to the Medicare programme.
The VHA is operated by the US Department of Veterans Affairs. It covers 9 million veterans at 1200 sites across the country, including approximately 170 medical centres, employing more than 300 000 people, and including over 100 academic health systems (US Department of Veterans Affairs, 2018). Spending on VHA medical care exceeded US$ 70.6 billion in 2016 and is covered through general federal government revenues. TriCare – financed through federal general revenues – pays for civilian health services used by active military and their families and some retirees, serving almost 10 million people. Generally, services must be received through the programme’s managed care networks, and require modest premiums and co-payments. Total spending on military care was about US$ 60 billion in 2016 (US Department of Veterans Affairs, 2018).
Public health organizations exist at every level: national, state, county and city. Public health functions are carried out by administrative units in diverse parts of the governmental organizations. The CDC, an HHS agency, is a principal component. Another example is the Commissioned Corps of the United States Public Health Service, headed by the Surgeon General. The public health services are organized as a military unit with a Commissioned Corps of 6500 that includes uniformed service and rankings that parallel military lines. Members of the United States Public Health Service Commission Corps serve throughout the various offices and agencies in HHS, as well as the Environmental Protection Agency and the United States Departments of Defense, Agriculture and Homeland Security.
Each of the main public health systems in the United States has a complex set of structural arrangements. Some health programmes, such as Medicaid, are organized and administered differently in each of the states, which makes it difficult to cover them in any depth here. Medicare is examined in some detail because it is a national programme.
The Social Security Administration (SSA) makes the initial determination as to whether or not an individual who applies for Medicare fulfils the eligibility requirements. The SSA also arranges for premiums to be withheld from the participant’s Social Security benefit cheque and determines an individual’s premium level, as these differ depending on the beneficiary’s income. In addition, the SSA maintains the database for Medicare in conjunction with its own records. The Internal Revenue Service (IRS), which is part of the United States Department of the Treasury, collects Medicare payroll taxes from workers and their employers. IRS data from an individual’s tax return are used to determine eligibility for income-adjusted Medicare subsidies (Klees, Wolfe & Curtis, 2009).
One critical issue is that US government health care system organizations overlap, and programmes between the various actors in Fig2.1 sometimes duplicate one another. This can result in both care coordination problems as well as gaps in services, in particular coverage areas and redundancies in other areas, which can be confusing to patients and providers.
Fig2.1
nbsp;8.3 billion.
Congress is also advised by several federal organizations, including the Congressional Budget Office (CBO) and Medicare Payment Advisory Commission (MedPAC). The CBO produces non-partisan analysis to Congress to support its budget process. CBO reports provide independent analysis to inform the health policy process. MedPAC is an independent body that advises Congress on payments to private health plans, FFS providers, and access and quality of care issues related to the Medicare programme.
The VHA is operated by the US Department of Veterans Affairs. It covers 9 million veterans at 1200 sites across the country, including approximately 170 medical centres, employing more than 300 000 people, and including over 100 academic health systems (US Department of Veterans Affairs, 2018). Spending on VHA medical care exceeded US$ 70.6 billion in 2016 and is covered through general federal government revenues. TriCare – financed through federal general revenues – pays for civilian health services used by active military and their families and some retirees, serving almost 10 million people. Generally, services must be received through the programme’s managed care networks, and require modest premiums and co-payments. Total spending on military care was about US$ 60 billion in 2016 (US Department of Veterans Affairs, 2018).
Public health organizations exist at every level: national, state, county and city. Public health functions are carried out by administrative units in diverse parts of the governmental organizations. The CDC, an HHS agency, is a principal component. Another example is the Commissioned Corps of the United States Public Health Service, headed by the Surgeon General. The public health services are organized as a military unit with a Commissioned Corps of 6500 that includes uniformed service and rankings that parallel military lines. Members of the United States Public Health Service Commission Corps serve throughout the various offices and agencies in HHS, as well as the Environmental Protection Agency and the United States Departments of Defense, Agriculture and Homeland Security.
Each of the main public health systems in the United States has a complex set of structural arrangements. Some health programmes, such as Medicaid, are organized and administered differently in each of the states, which makes it difficult to cover them in any depth here. Medicare is examined in some detail because it is a national programme.
The Social Security Administration (SSA) makes the initial determination as to whether or not an individual who applies for Medicare fulfils the eligibility requirements. The SSA also arranges for premiums to be withheld from the participant’s Social Security benefit cheque and determines an individual’s premium level, as these differ depending on the beneficiary’s income. In addition, the SSA maintains the database for Medicare in conjunction with its own records. The Internal Revenue Service (IRS), which is part of the United States Department of the Treasury, collects Medicare payroll taxes from workers and their employers. IRS data from an individual’s tax return are used to determine eligibility for income-adjusted Medicare subsidies (Klees, Wolfe & Curtis, 2009).
One critical issue is that US government health care system organizations overlap, and programmes between the various actors in Fig2.1 sometimes duplicate one another. This can result in both care coordination problems as well as gaps in services, in particular coverage areas and redundancies in other areas, which can be confusing to patients and providers.
Fig2.1
nbsp;5.4 billion.
Congress is also advised by several federal organizations, including the Congressional Budget Office (CBO) and Medicare Payment Advisory Commission (MedPAC). The CBO produces non-partisan analysis to Congress to support its budget process. CBO reports provide independent analysis to inform the health policy process. MedPAC is an independent body that advises Congress on payments to private health plans, FFS providers, and access and quality of care issues related to the Medicare programme.
The VHA is operated by the US Department of Veterans Affairs. It covers 9 million veterans at 1200 sites across the country, including approximately 170 medical centres, employing more than 300 000 people, and including over 100 academic health systems (US Department of Veterans Affairs, 2018). Spending on VHA medical care exceeded US$ 70.6 billion in 2016 and is covered through general federal government revenues. TriCare – financed through federal general revenues – pays for civilian health services used by active military and their families and some retirees, serving almost 10 million people. Generally, services must be received through the programme’s managed care networks, and require modest premiums and co-payments. Total spending on military care was about US$ 60 billion in 2016 (US Department of Veterans Affairs, 2018).
Public health organizations exist at every level: national, state, county and city. Public health functions are carried out by administrative units in diverse parts of the governmental organizations. The CDC, an HHS agency, is a principal component. Another example is the Commissioned Corps of the United States Public Health Service, headed by the Surgeon General. The public health services are organized as a military unit with a Commissioned Corps of 6500 that includes uniformed service and rankings that parallel military lines. Members of the United States Public Health Service Commission Corps serve throughout the various offices and agencies in HHS, as well as the Environmental Protection Agency and the United States Departments of Defense, Agriculture and Homeland Security.
Each of the main public health systems in the United States has a complex set of structural arrangements. Some health programmes, such as Medicaid, are organized and administered differently in each of the states, which makes it difficult to cover them in any depth here. Medicare is examined in some detail because it is a national programme.
The Social Security Administration (SSA) makes the initial determination as to whether or not an individual who applies for Medicare fulfils the eligibility requirements. The SSA also arranges for premiums to be withheld from the participant’s Social Security benefit cheque and determines an individual’s premium level, as these differ depending on the beneficiary’s income. In addition, the SSA maintains the database for Medicare in conjunction with its own records. The Internal Revenue Service (IRS), which is part of the United States Department of the Treasury, collects Medicare payroll taxes from workers and their employers. IRS data from an individual’s tax return are used to determine eligibility for income-adjusted Medicare subsidies (Klees, Wolfe & Curtis, 2009).
One critical issue is that US government health care system organizations overlap, and programmes between the various actors in Fig2.1 sometimes duplicate one another. This can result in both care coordination problems as well as gaps in services, in particular coverage areas and redundancies in other areas, which can be confusing to patients and providers.
Fig2.1
nbsp;36.2 billion.
Congress is also advised by several federal organizations, including the Congressional Budget Office (CBO) and Medicare Payment Advisory Commission (MedPAC). The CBO produces non-partisan analysis to Congress to support its budget process. CBO reports provide independent analysis to inform the health policy process. MedPAC is an independent body that advises Congress on payments to private health plans, FFS providers, and access and quality of care issues related to the Medicare programme.
The VHA is operated by the US Department of Veterans Affairs. It covers 9 million veterans at 1200 sites across the country, including approximately 170 medical centres, employing more than 300 000 people, and including over 100 academic health systems (US Department of Veterans Affairs, 2018). Spending on VHA medical care exceeded US$ 70.6 billion in 2016 and is covered through general federal government revenues. TriCare – financed through federal general revenues – pays for civilian health services used by active military and their families and some retirees, serving almost 10 million people. Generally, services must be received through the programme’s managed care networks, and require modest premiums and co-payments. Total spending on military care was about US$ 60 billion in 2016 (US Department of Veterans Affairs, 2018).
Public health organizations exist at every level: national, state, county and city. Public health functions are carried out by administrative units in diverse parts of the governmental organizations. The CDC, an HHS agency, is a principal component. Another example is the Commissioned Corps of the United States Public Health Service, headed by the Surgeon General. The public health services are organized as a military unit with a Commissioned Corps of 6500 that includes uniformed service and rankings that parallel military lines. Members of the United States Public Health Service Commission Corps serve throughout the various offices and agencies in HHS, as well as the Environmental Protection Agency and the United States Departments of Defense, Agriculture and Homeland Security.
Each of the main public health systems in the United States has a complex set of structural arrangements. Some health programmes, such as Medicaid, are organized and administered differently in each of the states, which makes it difficult to cover them in any depth here. Medicare is examined in some detail because it is a national programme.
The Social Security Administration (SSA) makes the initial determination as to whether or not an individual who applies for Medicare fulfils the eligibility requirements. The SSA also arranges for premiums to be withheld from the participant’s Social Security benefit cheque and determines an individual’s premium level, as these differ depending on the beneficiary’s income. In addition, the SSA maintains the database for Medicare in conjunction with its own records. The Internal Revenue Service (IRS), which is part of the United States Department of the Treasury, collects Medicare payroll taxes from workers and their employers. IRS data from an individual’s tax return are used to determine eligibility for income-adjusted Medicare subsidies (Klees, Wolfe & Curtis, 2009).
One critical issue is that US government health care system organizations overlap, and programmes between the various actors in Fig2.1 sometimes duplicate one another. This can result in both care coordination problems as well as gaps in services, in particular coverage areas and redundancies in other areas, which can be confusing to patients and providers.
Fig2.1
nbsp;6.1 billion in 2018, and is funded through federal government general revenues.
Congress is also advised by several federal organizations, including the Congressional Budget Office (CBO) and Medicare Payment Advisory Commission (MedPAC). The CBO produces non-partisan analysis to Congress to support its budget process. CBO reports provide independent analysis to inform the health policy process. MedPAC is an independent body that advises Congress on payments to private health plans, FFS providers, and access and quality of care issues related to the Medicare programme.
The VHA is operated by the US Department of Veterans Affairs. It covers 9 million veterans at 1200 sites across the country, including approximately 170 medical centres, employing more than 300 000 people, and including over 100 academic health systems (US Department of Veterans Affairs, 2018). Spending on VHA medical care exceeded USCMS is by far the largest agency in HHS because it administers the Medicare, Medicaid and CHIP programmes, which cover about 140 million Americans. It has about 6000 employees and an annual budget on various coverage programmes and agencies of approximately US$ 1 trillion in 2018.
Congress is also advised by several federal organizations, including the Congressional Budget Office (CBO) and Medicare Payment Advisory Commission (MedPAC). The CBO produces non-partisan analysis to Congress to support its budget process. CBO reports provide independent analysis to inform the health policy process. MedPAC is an independent body that advises Congress on payments to private health plans, FFS providers, and access and quality of care issues related to the Medicare programme.
The VHA is operated by the US Department of Veterans Affairs. It covers 9 million veterans at 1200 sites across the country, including approximately 170 medical centres, employing more than 300 000 people, and including over 100 academic health systems (US Department of Veterans Affairs, 2018). Spending on VHA medical care exceeded US$ 70.6 billion in 2016 and is covered through general federal government revenues. TriCare – financed through federal general revenues – pays for civilian health services used by active military and their families and some retirees, serving almost 10 million people. Generally, services must be received through the programme’s managed care networks, and require modest premiums and co-payments. Total spending on military care was about US$ 60 billion in 2016 (US Department of Veterans Affairs, 2018).
Public health organizations exist at every level: national, state, county and city. Public health functions are carried out by administrative units in diverse parts of the governmental organizations. The CDC, an HHS agency, is a principal component. Another example is the Commissioned Corps of the United States Public Health Service, headed by the Surgeon General. The public health services are organized as a military unit with a Commissioned Corps of 6500 that includes uniformed service and rankings that parallel military lines. Members of the United States Public Health Service Commission Corps serve throughout the various offices and agencies in HHS, as well as the Environmental Protection Agency and the United States Departments of Defense, Agriculture and Homeland Security.
Each of the main public health systems in the United States has a complex set of structural arrangements. Some health programmes, such as Medicaid, are organized and administered differently in each of the states, which makes it difficult to cover them in any depth here. Medicare is examined in some detail because it is a national programme.
The Social Security Administration (SSA) makes the initial determination as to whether or not an individual who applies for Medicare fulfils the eligibility requirements. The SSA also arranges for premiums to be withheld from the participant’s Social Security benefit cheque and determines an individual’s premium level, as these differ depending on the beneficiary’s income. In addition, the SSA maintains the database for Medicare in conjunction with its own records. The Internal Revenue Service (IRS), which is part of the United States Department of the Treasury, collects Medicare payroll taxes from workers and their employers. IRS data from an individual’s tax return are used to determine eligibility for income-adjusted Medicare subsidies (Klees, Wolfe & Curtis, 2009).
One critical issue is that US government health care system organizations overlap, and programmes between the various actors in Fig2.1 sometimes duplicate one another. This can result in both care coordination problems as well as gaps in services, in particular coverage areas and redundancies in other areas, which can be confusing to patients and providers.
Fig2.1
nbsp;70.6 billion in 2016 and is covered through general federal government revenues. TriCare – financed through federal general revenues – pays for civilian health services used by active military and their families and some retirees, serving almost 10 million people. Generally, services must be received through the programme’s managed care networks, and require modest premiums and co-payments. Total spending on military care was about USCMS is by far the largest agency in HHS because it administers the Medicare, Medicaid and CHIP programmes, which cover about 140 million Americans. It has about 6000 employees and an annual budget on various coverage programmes and agencies of approximately US$ 1 trillion in 2018.
Congress is also advised by several federal organizations, including the Congressional Budget Office (CBO) and Medicare Payment Advisory Commission (MedPAC). The CBO produces non-partisan analysis to Congress to support its budget process. CBO reports provide independent analysis to inform the health policy process. MedPAC is an independent body that advises Congress on payments to private health plans, FFS providers, and access and quality of care issues related to the Medicare programme.
The VHA is operated by the US Department of Veterans Affairs. It covers 9 million veterans at 1200 sites across the country, including approximately 170 medical centres, employing more than 300 000 people, and including over 100 academic health systems (US Department of Veterans Affairs, 2018). Spending on VHA medical care exceeded US$ 70.6 billion in 2016 and is covered through general federal government revenues. TriCare – financed through federal general revenues – pays for civilian health services used by active military and their families and some retirees, serving almost 10 million people. Generally, services must be received through the programme’s managed care networks, and require modest premiums and co-payments. Total spending on military care was about US$ 60 billion in 2016 (US Department of Veterans Affairs, 2018).
Public health organizations exist at every level: national, state, county and city. Public health functions are carried out by administrative units in diverse parts of the governmental organizations. The CDC, an HHS agency, is a principal component. Another example is the Commissioned Corps of the United States Public Health Service, headed by the Surgeon General. The public health services are organized as a military unit with a Commissioned Corps of 6500 that includes uniformed service and rankings that parallel military lines. Members of the United States Public Health Service Commission Corps serve throughout the various offices and agencies in HHS, as well as the Environmental Protection Agency and the United States Departments of Defense, Agriculture and Homeland Security.
Each of the main public health systems in the United States has a complex set of structural arrangements. Some health programmes, such as Medicaid, are organized and administered differently in each of the states, which makes it difficult to cover them in any depth here. Medicare is examined in some detail because it is a national programme.
The Social Security Administration (SSA) makes the initial determination as to whether or not an individual who applies for Medicare fulfils the eligibility requirements. The SSA also arranges for premiums to be withheld from the participant’s Social Security benefit cheque and determines an individual’s premium level, as these differ depending on the beneficiary’s income. In addition, the SSA maintains the database for Medicare in conjunction with its own records. The Internal Revenue Service (IRS), which is part of the United States Department of the Treasury, collects Medicare payroll taxes from workers and their employers. IRS data from an individual’s tax return are used to determine eligibility for income-adjusted Medicare subsidies (Klees, Wolfe & Curtis, 2009).
One critical issue is that US government health care system organizations overlap, and programmes between the various actors in Fig2.1 sometimes duplicate one another. This can result in both care coordination problems as well as gaps in services, in particular coverage areas and redundancies in other areas, which can be confusing to patients and providers.
Fig2.1
nbsp;60 billion in 2016 (US Department of Veterans Affairs, 2018).
Public health organizations exist at every level: national, state, county and city. Public health functions are carried out by administrative units in diverse parts of the governmental organizations. The CDC, an HHS agency, is a principal component. Another example is the Commissioned Corps of the United States Public Health Service, headed by the Surgeon General. The public health services are organized as a military unit with a Commissioned Corps of 6500 that includes uniformed service and rankings that parallel military lines. Members of the United States Public Health Service Commission Corps serve throughout the various offices and agencies in HHS, as well as the Environmental Protection Agency and the United States Departments of Defense, Agriculture and Homeland Security.
Each of the main public health systems in the United States has a complex set of structural arrangements. Some health programmes, such as Medicaid, are organized and administered differently in each of the states, which makes it difficult to cover them in any depth here. Medicare is examined in some detail because it is a national programme.
The Social Security Administration (SSA) makes the initial determination as to whether or not an individual who applies for Medicare fulfils the eligibility requirements. The SSA also arranges for premiums to be withheld from the participant’s Social Security benefit cheque and determines an individual’s premium level, as these differ depending on the beneficiary’s income. In addition, the SSA maintains the database for Medicare in conjunction with its own records. The Internal Revenue Service (IRS), which is part of the United States Department of the Treasury, collects Medicare payroll taxes from workers and their employers. IRS data from an individual’s tax return are used to determine eligibility for income-adjusted Medicare subsidies (Klees, Wolfe & Curtis, 2009).
One critical issue is that US government health care system organizations overlap, and programmes between the various actors in Fig2.1 sometimes duplicate one another. This can result in both care coordination problems as well as gaps in services, in particular coverage areas and redundancies in other areas, which can be confusing to patients and providers.
Fig2.1
2.2.3. Private organizations
Purchasers and providers have national-level professional organizations that represent their common interest, operate as spokespersons for them and lobby policy-makers in Congress to advance their respective policy preferences. For example, America’s Health Insurance Plans (AHIP) is a national organization that represents about 1300 private for-profit companies that provide health insurance coverage, dental insurance, long-term care insurance and disability income insurance, as well as a variety of other insurance products.
Each payer listed in Fig2.1 has a different organizational structure, though they share some organizational characteristics. Most private sector employers that offer health insurance are publicly traded. They have corporate structures and are subject to the accounting and reporting obligations of the Securities and Exchange Commission (the stock exchange). Employers that qualify as private companies (not listed on the stock exchange) have greater freedom and fewer reporting obligations than public companies.
Fig2.1
Under ACA’s employer mandate implemented in 2014, employers in the United States with 50 or more employees are required to provide health insurance for their employees. Most very large employers, public or private, “self-insure”, which means that they offer health insurance to their employees directly rather than purchasing it from an insurance company. They may hire an outside agency or an insurance company, sometimes referred to as a third party administrator, to manage their company health insurance plan. Companies that self-insure assume the financial risk, but they may purchase insurance to cover any employees that incur large medical costs, a practice that is referred to as reinsurance.
In addition, there are some significant private or independent organizations that play an important role. For example, the National Committee for Quality Assurance (NCQA) measures and reports on quality of care of those physicians, hospitals and health plans that pay to be evaluated. Another is the Joint Commission that accredits and monitors the quality of health care organizations.
2.2.4. States
The 50 state government organizations are major actors in the US health care system. Under the Trump Administration they received even more responsibilities. They share important roles with the federal government in finance, planning, administration, regulation and the provision of health care through Medicaid, mental health services, public hospitals and health departments (with the cities and counties). They monitor and enforce environmental regulations, some of which are issued by the federal government. They license physicians, nurses and other health care workers and regulate the sale of health insurance.
States accomplish their roles in the health care system through various organizational structures. Most states have a Division of Insurance as well as a Department of Health, Human Services or Social Services. These administrative departments are generally organized much like their equivalents on the federal level. Most states, unlike the federal government, may not legally run a budgetary deficit and this affects how they fulfil their functions. States emphasize health care to varying degrees, which makes for wide variations between the states in health services offered to citizens.
Medicaid is jointly funded by the federal and state governments. Although administered by the states, numerous federal requirements apply, and Medicaid eligibility varies widely across the states.