-
20 August 2025 | Policy Analysis
Ten Year Plan for the English NHS
6.1. Analysis of recent reforms
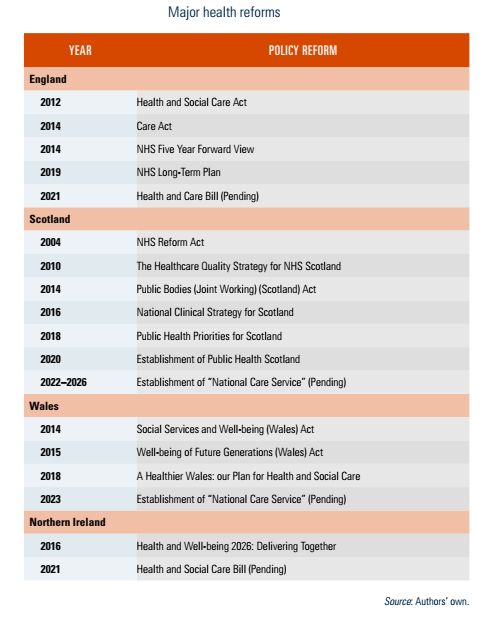
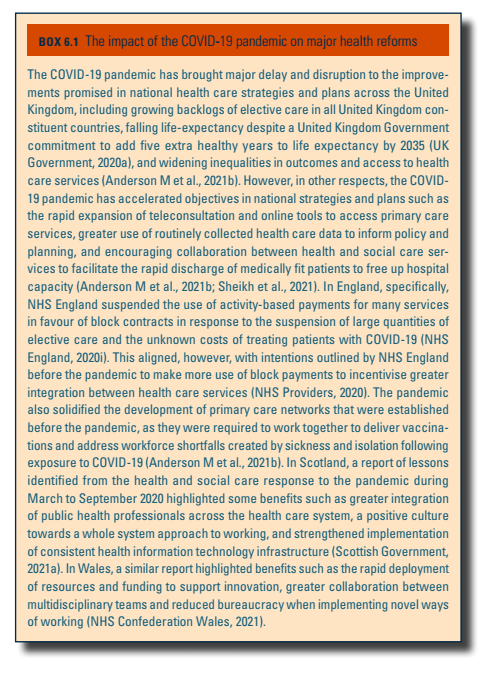
Health policy has been devolved in the United Kingdom since the late 1990s, with governments in England, Scotland, Wales and Northern Ireland taking different approaches to health care reform. A review of major policy reforms is contained in Table6.1. Health policy diverged in the 2000s, as reforms in England emphasized choice and competition as the route to improve quality of care, while governments in Scotland and Wales dismantled the internal market and promoted cooperation. There has been some policy convergence in recent years, as reforms in all countries encouraged collaboration between local agencies and integration of health and social care services. The COVID-19 pandemic has had mixed impacts on the progress of major health reforms across the United Kingdom and this is discussed in Box6.1.
| Table6.1 | Box6.1 |
 |  |
On 3 July 2025, the UK Government published “Fit for the Future: 10 Year Health Plan for England” [1]. This strategic document sets out a long-term vision for changing and improving care delivery and financial resilience in England’s public sector healthcare system. It will be followed by a specific delivery plan, and an updated workforce strategy.
This plan’s creation was announced by the incoming Labour government in July 2024, in the context of a change of ruling party and of historically high dissatisfaction with the English NHS [2]. Its remit and definition of problems were informed by the Darzi Review into the performance of the service [3]. During late 2024, a national engagement effort to inform the plan – “Change NHS” – gathered more than 250 000 contributions from staff, patients and the public. Its drafting emphasizes an urgent need to change, faith that great improvement is possible through efficiency and innovation and the goal of choice and improved experience for patients.
“Shifts” envisaged in the plan
The plan emphasizes “three fundamental shifts” in the English health service, with an extensive collection of commitments and over 200 specific initiatives.
- A shift from “Hospital to community”. This includes a commitment that the share of expenditure on hospital care will fall within three to four years. “Neighbourhood health services” will be created that connect primary and community care services through different contract models. Shared locations for this will be created as 250–300 “neighbourhood health centres” that provide integrated local services that will be staffed by multidisciplinary teams. The plan argues that this shift in resources and structure will enable savings in hospital services. There is a pledge to reform the dental contract, widely seen as unfit for purpose.
- A shift from “analogue to digital”. This would enhance the existing English NHS App, widely downloaded during the COVID-19 pandemic but limited in usage and functionality into a central interface for patient self-referral, appointment booking to neighbourhood health services, repeat prescription management, and collecting patient feedback shared with care providers. There is also to be a mandated single patient record by 2028. The plan envisages a rapidly growing role for both patient-facing and clinician support AI, with a national scheme to procure “Ambient AI” scribing interactions for care records.
- A shift from “sickness to prevention”. New public health measures include easier access to weight loss medications, restrictions on junk food advertising and restrictions on high caffeine energy drink sales to minors. The plan commits to “genomics population health service” with universal screening for newborns.
Other measures
The plan also contains several other significant policy commitments, on quality, workforce, technology and innovation, structure, and financing.
- Self-referral enabled for services such as mental health, audiology, podiatry and musculoskeletal care via the NHS App.
- An aspiration for high-performing provider bodies in the NHS to earn greater autonomy and to be rewarded with financial incentives, with 50% fewer officials employed in the central bodies of the health service.
- An emphasis on “strategic commissioning” (purchasing) as the core role of Integrated Care Boards, which are the regional fund-holding bodies of the English NHS covering populations typically around 2 million.
- Health technology appraisals conducted by NICE for compulsory adoption will be expanded to medical devices and digital products. The body will also review previously approved pharmaceutical products to eliminate those that are no longer cost effective.
- There will be a trial of “Patient power payments”, a concept where patients are contacted after care and decide whether to deduct an amount from the provider’s payment based on satisfaction with their care.
- The plan continues the long-standing interest of the English NHS in expanding the roles of different professions to take on tasks traditionally reserved for those with certain medical and nursing qualifications. It aims to expand the paradigm of training healthcare workers to individual tasks rather than wider roles, and states that there are “significant opportunities to move beyond traditional professional boundaries in a safe and productive way.”
- Measures to enhance personalized care, including the introduction of personal health budgets for up to one million people by 2030, with universal availability by 2035. A new standard that, by 2027, 95% of people with complex needs will have an agreed care plan.
- A maximum 10% reliance on overseas recruitment by 2035 – reliance on staff trained outside the UK is currently far higher, and above 50% for newly registering qualified doctors [4].
Reaction and analysis
Expert and representative bodies in the UK broadly welcomed the direction of the “three shifts” and accepted the problems the plan aims to address. Many expressed some scepticism around delivery. Common concerns were that such an expansive agenda would be difficult to deliver properly or sustainably given the relatively modest increases in the budget announced following the plan; that details of contracts and timescales were limited; and that social care and public health services in England remained unreformed and underfunded, creating a difficult context [5, 6]. The emphasis on adopting innovation has the potential to increase costs [7].
Several reactions noted that the plan brings back a higher reliance on financial incentives, competing providers and a divide between purchasers and providers [8]. This partially reverses previous moves towards greater collaboration to drive integrated care, though many of these initiatives are being retained or redeveloped as well.
References
[1] https://www.gov.uk/government/publications/10-year-health-plan-for-england-fit-for-the-future
[3] https://www.gov.uk/government/publications/independent-investigation-of-the-nhs-in-england
[4] Rolewicz L, Dayan M, Hemmings N, Palmer W (2025). Immigration crackdown threatens NHS workforce, data show. BMJ 2025; 390:r1554 doi: https://doi.org/10.1136/bmj.r1554 (Published 5 August 2025)
[6] https://nhsproviders.org/resources/on-the-day-briefing-spending-review-2025
6.1.1. England
In 2012, the Conservative–Liberal Democrat Coalition Government introduced major reforms to the NHS in England. New Labour governments in the 2000s had used a mix of market-based approaches to try to improve NHS care, including supply-side reforms (for example, by giving patients more choice of health care provider), demand-side reforms (for example, more diversity in health care providers), transactional reforms (for example, new fixed price activity-based payments for hospitals) and changes to the health system management and regulation (for example, by the enforcement of quality standards) (Mays & Jones, 2011). The 2012 Health and Social Care Act sought to strengthen the role of competition in the English NHS and devolve decision-making (UK Government, 2012).
The 2012 Act meant widespread changes to the structure of the NHS. Various agencies responsible for managing services at a local and regional level, such as Primary Care Trusts and Strategic Health Authorities, were abolished, and CCGs were established to commission most local health care services (see section 2.7.1 Regulation and governance of third-party payers). National governance also changed. NHS England was established to lead the NHS commissioning system. Monitor, which was replaced by NHS Improvement in 2016, was given an expanded role as the economic regulator for health and social care (see section 2.7.2 Regulation and governance of provision). The NHS Trust Development Authority was also established as an executive non-departmental public body of the Department of Health with the objective of offering support to NHS hospitals that were seeking to be granted Foundation Trust status (see section 2.7.2 Regulation and governance of provision). Public Health England was created to improve public health at a national level (although Public Health England has since been replaced by the United Kingdom Health Security Agency and Office for Health Improvement and Disparities; see section 2.2 Organization) and local responsibilities for public health were transferred from the NHS to local governments.
An initial independent assessment of the Act in 2015 concluded that the changes had been “damaging and distracting” for the NHS (Ham et al., 2015). A gap emerged between the formal rules governing the NHS – set out in the 2012 Health and Social Care Act – and the way the health system was managed in practice. The NHS Five Year Forward View was published in 2014, and rejected the notion of promoting competition between health care providers in favour of encouraging collaboration and integration of services within the NHS and between health and social care (NHS England, 2014). Despite having no place in the formal NHS structure, national NHS leaders established regional partnership boards of NHS commissioners, providers and local governments – first called sustainability and transformation plans, in 2015, then ICSs – to plan local services and jointly manage constrained resources (see section 2.2 Organization) (Alderwick & Ham, 2017).
In 2019, NHS England and other national agencies published the NHS Long Term Plan – a 10-year strategy for NHS improvement and reform (NHS England, 2019d) (see section 2.4 Planning). The Plan aimed to expand primary and community care (through the development of primary care networks among other measures), strengthen action on prevention and health inequalities, and improve care quality. ICSs were expected to be established to lead service improvements across populations of around 1 to 3 million people. To help deliver the plan, national NHS bodies called on government to amend NHS legislation to formally establish ICSs as statutory bodies and remove requirements to competitively tender clinical services (Alderwick et al., 2019, 2021). The United Kingdom Government responded to these calls by NHS bodies by proposing legislation (see section 6.2 Future developments), and these and other changes are planned to be introduced from July 2022.
The adult social care system in England has experienced less major reform. In 2014, the United Kingdom Government passed the Care Act, which defined the purpose of adult social care as promoting well-being – including: improving people’s physical and emotional health, relationships with others, control over their life, participation in work, education, training or recreation, sustainability of housing, and more (UK Government, 2014). The 2014 Care Act also legislated for a cap on the maximum amount an individual would need to pay towards their adult social care services – following the approach recommended by the Dilnot Commission in 2011 (Dilnot, 2011). But the cap was not introduced and the social care system continued receiving limited state funding (Anderson M et al., 2021b). In 2021, the United Kingdom Government announced that a lifetime cap on care costs of £86 000 would be introduced in 2023 (see section 6.2 Future developments).
6.1.2. Scotland
After devolution, reforms in Scotland dismantled the NHS internal market and focused on collaboration between agencies and integration of services. The 2004 NHS Reform Act required local NHS boards to establish community health partnerships, responsible for coordinating planning and delivery of services in the NHS and between health and social care (Scottish Government, 2004). However, a review of the partnerships by Audit Scotland in 2011 found that governance and accountability arrangements for community health partnerships were complex and not always clear (Audit Scotland, 2011).
In 2014, the Scottish government created a new legal framework for health and social care integration, through the 2014 Public Bodies (Joint Working) (Scotland) Act (Scottish Government, 2014). Health boards and local governments were required to establish integration authorities (replacing community health partnerships) by 2016, responsible for coordinating health and social care services and improving health against nationally agreed outcomes (see section 2.4 Planning). Nearly all the 31 integration authorities opted to establish IJBs between the NHS and local governments, responsible for planning local services and managing joint budgets. A review in 2018 identified some progress in joining up services, but also found a lack of integration in financial planning and challenges related to leadership and governance (Audit Scotland, 2018).
NHS reforms in Scotland have been underpinned by a long-standing and systematic approach to quality improvement (OECD, 2016). In 2008, Scotland launched the world’s first national patient safety programme, initially focused on preventing avoidable mortality and harm in acute hospitals (Healthcare Improvement Scotland, 2021). There is widespread use of small-scale testing and revision of new health care quality improvement initiatives (Dayan & Edwards, 2017). A long-term strategy for improving quality in the Scottish NHS was published in 2010, with goals to 2020 (NHS Scotland, 2010). This strategy was complemented by the publication of the National Clinical Strategy for Scotland, which reviewed progress to date and outlined further objectives towards a longer time scale, up to 2025–2030 (Scottish Government, 2016a).
In 2016, a Public Health Review emphasized the cost-effectiveness of preventive approaches and the need for a more proactive public health effort in Scotland, including rationalized organizational arrangements. Public Health Priorities for Scotland (Scottish Government, 2018) was subsequently published in 2018 and national public health functions were consolidated into a new body, Public Health Scotland, in 2020.
The Centre for Sustainable Delivery was launched in 2021 and is focused on delivering transformation and innovation in the NHS (Scottish Government, 2021d). It brings together a range of established programmes including Modernising Patient Pathways, Scottish Access Collaborative, Detect Cancer Early and Unscheduled Care. It is also developing new capabilities, including hosting a new innovation adoption function for NHS Scotland.
6.1.3. Wales
As in Scotland, reforms to the Welsh NHS after devolution led to the removal of the internal market and a focus on cooperation to improve services. The 2014 Social Services and Well-being (Wales) Act introduced a mix of changes to strengthen local partnership working, promote prevention and early intervention, place people and their needs at the heart of services and support people to improve their well-being (Welsh Government, 2014a). The Act also introduced a new legal duty on local authorities to promote integration of services. Regional partnership boards were established between health boards and local authorities, responsible for planning and developing local services to improve health and well-being in their area (see section 2.4 Planning). Regional partnership boards have also been supported by the establishment of a transformation fund and integrated care fund, which have funded the development of specific projects and novel models of care locally. A process evaluation of the reforms found widespread support for the principles of the Act, but also identified some challenges for successful implementation of the reforms, such as lack of parity of funding between health and social care, inconsistency in the approach to integration and limited awareness of the Act (Welsh Government, 2021d).
The 2015 Well-being of Future Generations (Wales) Act also encouraged collaboration between local agencies to improve health and well-being (see section 2.5 Intersectorality). All local authority areas in Wales are required to establish a public service board, with representatives from local governments, health boards and other public and voluntary sector agencies. Each public service board designs and delivers a local well-being plan every five years to contribute to a set of national well-being goals – including a healthier, more equal and resilient Wales. Public bodies also have a duty to consider the long-term impact of their decisions on health and well-being.
6.1.4. Northern Ireland
Since 2000, there has been a series of major reviews of the health system in Northern Ireland. The verdict offered by each has been similar, including the need to reduce reliance on acute hospital care, centralize some services, and place greater focus on prevention and improving health (Heenan & Appleby, 2017). Yet progress on the changes needed has been limited in the last decade. Complex political issues characterized by polarized political parties have slowed health policy change.
In 2016, the Bengoa review – the latest major report on the health system – identified a process of review fatigue: significant time and resources had been spent analysing issues in the health system and making recommendations for change, followed by failure to enact the changes needed (Bengoa, 2016). Bengoa’s report was used to inform a new 10-year plan for the health system in Northern Ireland, Health and Well-being 2026: Delivering Together, which set out an ambitious programme for improvement and reform – including to strengthen preventive services, provide more support in primary care, develop new models of hospital and community care, and create new partnerships between agencies to help deliver the changes (Department of Health Northern Ireland, 2016). According to the plan, cooperation rather than competition is the intended mechanism to achieve improvements. However, progress against the plan appears to be slow and is particularly hampered by limited funding, the suspension of the Northern Ireland devolved government between 2017 and 2020 (Dayan & Heenan, 2019), and the COVID-19 pandemic.