-
19 January 2024 | Country Update
Current health expenditure in 2022: Back to business-as-usual
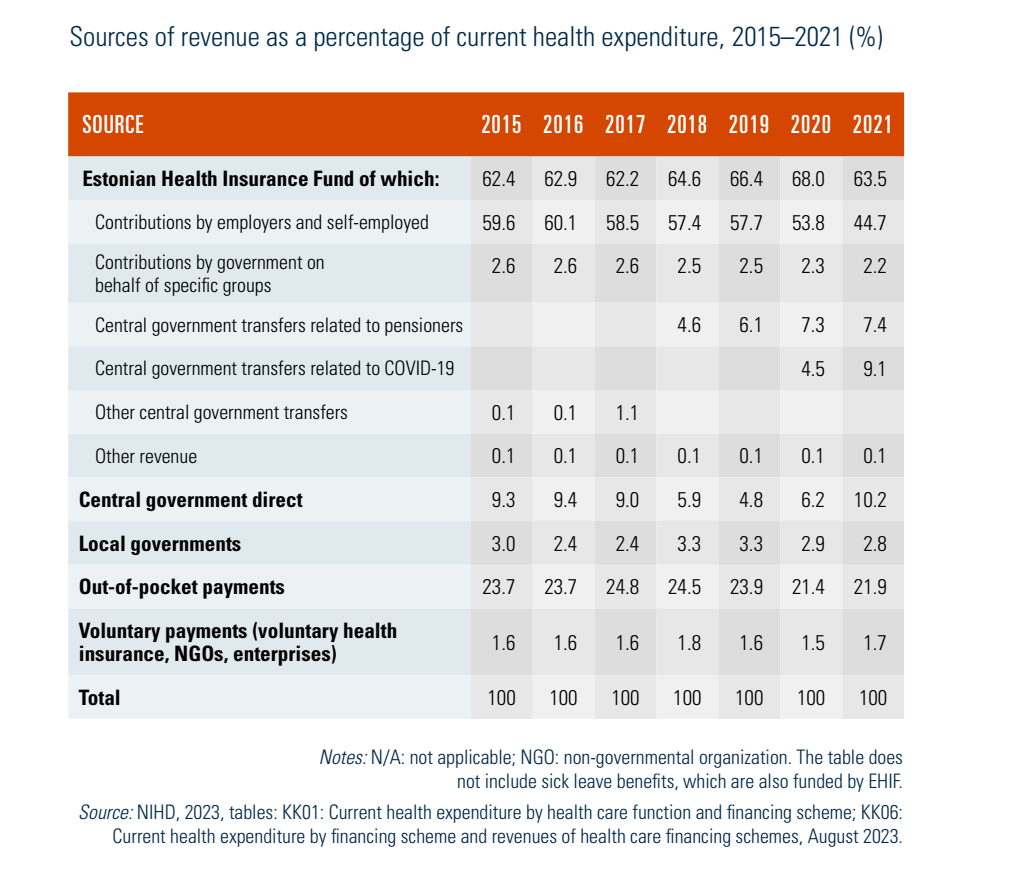
3.2. Sources of revenue and financial flows
The largest source of funding for the health system is mandatory insurance contributions to the EHIF in the form of an earmarked social payroll tax (44.7% of current health expenditure in 2021, see Table3.2). Central government expenditure, which can occur both directly (10.2% in 2021) and via government-paid contributions (2.2% in 2021) or transfers (16.5% in 2021) to the EHIF, is the second source of health system financing in terms of volume (Table3.2). The share of local governments and other voluntary payments (such as voluntary insurance) is negligible (2.8% and 1.7%, respectively, in 2021), but the role of voluntary insurance funded by employers is increasing rapidly (see section 3.5 Voluntary health insurance). The remaining 21.9% of resources came from OOP spending. Fig3.7 depicts the main financial flows in the Estonian system.
| Table3.2 | Fig3.7 |
 | 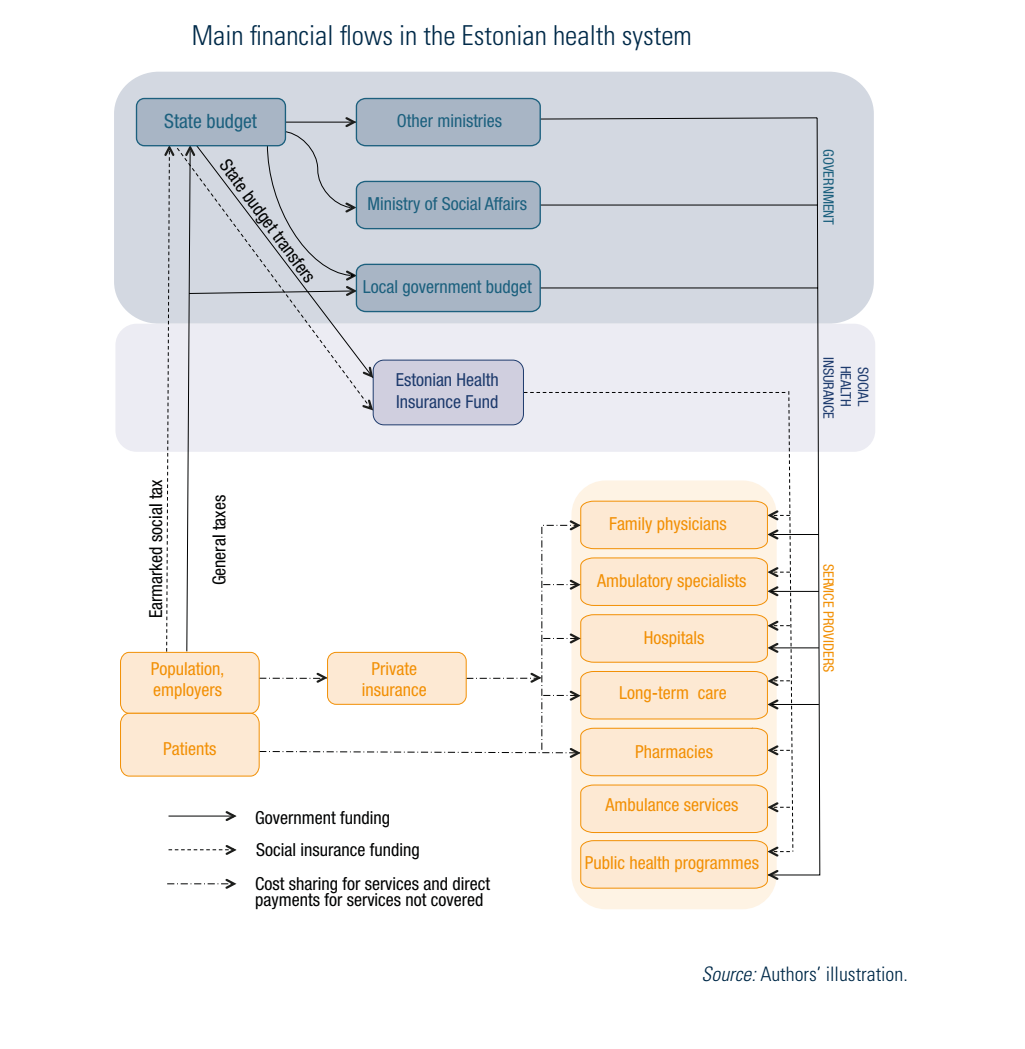 |
The EHIF pools the mandatory contributions and also acts as a single purchaser of care. The EHIF is an independent public body that is responsible for contracting service providers, reimbursing health services and pharmaceuticals, and covering for sick and care leave (see section 2.2.1 The role of the state and its agencies).
The changes between 2015 and 2021 in the structure of the public financing of health care were the result of political decisions and the COVID-19 pandemic. In 2018, the EHIF started receiving additional revenues from the central government, which depends on the total amount of pensions of non-working pensioners. The EHIF also assumed responsibility for emergency care for uninsured people, ambulance care and other public health priorities previously funded by central government (see section 6.1.4 Sequential actions to improve coverage, access and financial protection). As a result, the EHIF’s share of health care expenditure increased from 62.2% to 68.0% from 2017 to 2020. On the other hand, with the COVID-19 pandemic, direct government expenditure temporarily increased in 2020–2021 as the result of purchases of COVID-19 vaccines and tests. Furthermore, the central government allocated funds to the EHIF to cover the additional costs for the COVID-19 response and the decline in revenues.
Other purchasers/payers of health care funded by general taxation include the MoSA, which is responsible for financing some public health programmes, and the Ministry of Justice (see section 3.6 Other financing). The municipalities play a relatively minor role, mainly organizing long-term care and patient transportation (see section 2.2.2 Local governments).
In 2021, outpatient care accounted for the largest share of expenditure (27.1%, see Table3.3, last column), followed by inpatient care (23.2%) and pharmaceuticals (15%). Inpatient care is almost fully financed by mandatory health insurance (95.8%, see first row of Table3.3). The role of OOP payments is significant (35.4%) for outpatient care (mainly dental care, but also specialist care) and long-term care (42.4%), following traditionally high private spending on pharmaceuticals (40.5%) and medical goods (66.4%). The government contribution is largest for preventive care (65.3%), long-term care (31.1%) and medical goods (25.2%). Spending on governance and administration was divided between the general government (60.9%) and the mandatory insurance scheme (39.1%) (see Table3.3).
Table3.3

In 2022, Estonia returned to pre-pandemic level in health spending with current health expenditure (CHE) falling to 7.1% of GDP from a high of 7.6% in the COVID-19 peak years of 2020 and 2021. In absolute terms, €2.54 billion was spent on health, €180 million more than in the previous year – an increase of 7.6%.
Additional expenses, incurred due to the COVID-19 crisis, led to increased healthcare costs in 2020 and 2021. Although the need to compensate for pandemic-related costs eased in 2022, inflationary pressure on employee salaries and rising energy prices increased. In 2022, three quarters of health expenditure came from the public sector. Even though the expenditure by the Estonian Health Insurance Fund (EHIF) and local governments increased, the role of central government expenditure decreased, as COVID-19 vaccination and surveillance costs diminished. As a result, spending on prevention activities decreased from 8.8% of CHE in 2021 to 6.1% in 2022.
In addition, the share of out-of-pocket (OOP) payments rose slightly to 23.2% of CHE (from 22.5% in 2021), which is close to the 10-year average of 23.5%. The largest share of OOP expenditure is still dental care (32%), followed by prescription and over-the-counter medicines (14% and 12%, respectively), long-term care (18%) and outpatient specialist care (11%).
Finally, there’s a small increase in voluntary health funding (VHI, NGOs, enterprises), which rose from 1.7% in 2021 to 2.0% in 2022. Although the role of VHI remains small at 0.7%, it has doubled since 2021.
References
National Institute for Health Development “Health expenditure in Estonia 2021”, press release 23 November 2023: https://tai.ee/et/uudised/leibkondade-omaosalus-tervishoiukuludes-jatkas-tousu-2022-aastal
National Institute for Health Development, Health Statistics and Health Research Database, table KK01: Current health expenditure by health care function and financing scheme https://statistika.tai.ee/pxweb/en/Andmebaas/Andmebaas__04THressursid__10Tervishoiukulud/KK01.px