-
18 March 2024 | Country Update
Fee-paying afternoon surgeries introduced in public hospitals -
18 March 2024 | Policy Analysis
Afternoon surgeries in public hospitals are introduced with patients paying out of pocket for these services -
01 December 2023 | Country Update
Establishing the National Network of Enhanced Care Units for the treatment of patients with Vascular Stroke -
31 May 2023 | Country Update
Establishment of Hospital at Home and Home Health Care
5.4. Specialized ambulatory care / inpatient care
On 5 March 2024, Greece launched the operation of afternoon surgeries in public hospitals. The new measure aims to reduce the long waiting lists for surgeries in these hospitals.
Afternoon surgeries will be paid for by patients, who will be able to choose which doctor will operate on them, thus bypassing the existing waiting list for free operations carried out during the regular operating hours of public hospitals. Irrespective of their social health insurance status, patients taking up this option will pay a fee ranging from EUR 300 to 2000, based on the complexity of the operation.
Doctors’ unions and the Panhellenic Medical Association have raised strong objections, citing existing staff shortages within public hospitals as an impediment to implementation. Other critiques focus on the negative impact on the principle of equity in access to health care; failure to adequately invest and address personnel shortages in National Health System hospitals; and the policy’s potential to incentivize supplier induced demand for such privately funded operations.
See the corresponding Policy Analysis: Afternoon surgeries in public hospitals are introduced with patients paying out of pocket for these services, 18 March 2024.
Authors
References
Joint Ministerial Decision No G2a/10666, “Surgeries and other invasive operations that are carried out outside the regular operating hours of the National Health System hospitals and require a stay in the hospital beyond the daily hospitalization”. Official Government Gazette, Issue B’, Number 1485/05-03-2024 (available at: https://www.et.gr/api/DownloadFeksApi/?fek_pdf=20240201485) (in Greek).
Ministry of Health, “The operating framework of the afternoon surgeries was presented in a press conference by the Minister of Health Adonis Georgiadis and the Deputy Minister of Health Marios Themistokleous” (available at: https://www.moh.gov.gr/articles/ministry/grafeio-typoy/press-releases/12205-to-plaisio-leitoyrgias-twn-apogeymatinwn-xeiroyrgeiwn-paroysiasan-se-synenteyksh-typoy-o-ypoyrgos-ygeias-adwnis-gewrgiadhs-kai-o-yfypoyrgos-ygeias-marios-themistokleoys) (in Greek).
Context and impetus for the reform
The operation of afternoon surgeries in public hospitals was launched on 5 March 2024 by the Joint Ministerial Decision signed by the Health Minister and the Deputy Minister of Economy and Finance.
According to the Ministry of Health, the new measure aims to reduce the long waiting lists for surgeries in public hospitals, with some patients waiting up to three years for an operation. Based on the Ministry’s estimations, about 102 634 patients are waiting for a surgery across the country, out of which 43% of cases wait less than 4 months, 31% wait from 4 to 12 months and the remaining 26% wait for more than 12 months. The Ministry of Health is also in favour of the measure arguing that with this policy, employees within the National Health System, namely doctors and nurses, are given an opportunity to increase their incomes in a legal way.
Content of the reform
Afternoon surgeries will be paid for by patients, who will be able to choose which doctor will operate on them, thus bypassing the existing waiting list for free operations that are carried out during the regular operating hours of public hospitals.
These surgeries will be carried out after the regular operating hours of the National Health System hospitals and patients, irrespective of their social insurance status, will have to pay a fee ranging from EUR 300 to 2000, based on the complexity of the operation. The price list is as follows:
- very minor operation: EUR 300
- minor operation: EUR 500
- medium operation: EUR 900
- major surgery: EUR 1200
- heavy surgery: EUR 1600
- extremely heavy surgery: EUR 2000
For example, for a cataract operation, the patient will have to pay EUR 300 to EUR 500; for an inguinal hernia operation, which is considered a minor surgery, the cost will reach EUR 500; for cholecystectomy, prices start at EUR 500 and can reach up to EUR 1200; for knee arthroplasty, the price can reach up to EUR 1600.
However, the Minister of Health declared that 50 000 afternoon surgeries are to be free of charge as they will be funded by the EU Recovery and Resilience Fund under Greece’s National Recovery and Resilience Plan 2021–2026. These surgeries concern patients who remain on the surgery list for a long time and their prioritization will be done in chronological order (from oldest to newest), as reflected in the Unified List of Surgeries (See Country Update: The newly launched Unified Digital List of Surgeries aims to reduce hospital waiting times, 6 February 2024).
Policy implications
Four questions have been raised about the new policy.
The first is the feasibility of implementing the measure. Not all hospitals will be able to implement the afternoon surgeries. Currently, three big hospitals in Athens and one in Thessaloniki are assigned the task of implementing afternoon surgery. This is because about 40% of operating rooms in public hospitals are closed due to personnel shortages. The Panhellenic Federation of Public Hospital Employees, the Federation of Greek Hospital Doctors’ Associations and the Panhellenic Medical Association have raised strong objections to the afternoon surgeries due to staff shortages, especially in anesthesiologists, and have pointed to shortages in nursing personnel as well as to bed capacity. Additionally, the gruelling work schedules of doctors and nurses far exceed the maximum weekly limits on working hours, calling into question the feasibility of the additional burden of evening work beyond morning and on-call work. A consequence may be that doctors may concentrate on those patients who use the private option at the expense of patients in the public system, resulting in a reduction in surgeries conducted during the regular operating hours and an increase in surgeries conducted in the afternoon.
The second issue is related to patients’ participation in the cost of the services provided and the economic burden posed on them, possibly resulting in catastrophic health expenditure. This is a basic reason why, according to the results of a recent poll, 59.5% of the respondents were against this practice. From the perspective of patients paying out of pocket for afternoon surgery, the new measure may have more adverse effects than those expected by the Ministry of Health. Under the current policy, instead of hiring additional personnel, the health system imposes an extra charge on patients who already pay social security contributions and yet do not receive the services they need. Moreover, critics point out that the attempt to operate the for-payment afternoon surgeries of public hospitals as market competitors of private hospitals with price lists that burden patients violates the principle of equity in access to health care within the National Health System.
A third criticism is that with this measure the Ministry of Health is trying to avoid the necessary increases in the salaries of public hospital personnel by legitimizing the practice of informal payments and formalizing them into extra payments routed to doctors and other healthcare staff engaged in the afternoon surgeries. However, critics argue that the new arrangements will not eradicate informal payments: rather, existing shortages in health resources in the public hospital system will also put limitations on afternoon surgeries, leading to the risk that patients will have to resort to additional (informal) payments on top of the formal fee to gain a slot and have the procedure done privately in the public system.
Authors
References
Joint Ministerial Decision No G2a/10666, “Surgeries and other invasive operations that are carried out outside the regular operating hours of the National Health System hospitals and require a stay in the hospital beyond the daily hospitalization”. Official Government Gazette, Issue B’, Number 1485/05-03-2024 (available at: https://www.et.gr/api/DownloadFeksApi/?fek_pdf=20240201485) (in Greek).
Ministry of Health, “The operating framework of the afternoon surgeries was presented in a press conference by the Minister of Health Adonis Georgiadis and the Deputy Minister of Health Marios Themistokleous” (available at: https://www.moh.gov.gr/articles/ministry/grafeio-typoy/press-releases/12205-to-plaisio-leitoyrgias-twn-apogeymatinwn-xeiroyrgeiwn-paroysiasan-se-synenteyksh-typoy-o-ypoyrgos-ygeias-adwnis-gewrgiadhs-kai-o-yfypoyrgos-ygeias-marios-themistokleoys) (in Greek).
Keep Talking Greece, “Pay or Die: Greece’s Health Ministry introduces Afternoon Surgeries” (available at: https://www.keeptalkinggreece.com/2024/03/05/greece-afternoon-surgeries-pay-or-die-health-ministry).
On 19 May 2023, a Joint Ministerial Decision from the Ministers of
Health and Economics was published, concerning the establishment of home
health care and hospital at home systems for targeted sensitive groups
of patients with chronic disabilities. It provides for home care
combined with parallel organized support from health care units for
children, adolescents and adults with serious chronic health problems
that cause long-term or permanent disabilities.
The aim
is to improve the quality of life of patients while freeing up hospital
beds and saving resources for the national healthcare system. In
particular, this decision concerns patients, children and adults, with
different underlying primary disease (chronic respiratory obstructive or
restrictive diseases, rapidly or slowly progressive neurological
diseases such as motor neuron disease, myasthenia, cystic fibrosis,
chronic heart failure and other chronic diseases) and oncology patients
who need specialized long-term care and oncology treatment at home.
The patient’s home will be assimilated to the hospital environment, (operating as a place of care), under the terms and conditions provided for the provision of hospital care services at home. The program’s Reference Center is defined as the clinic/hospital department, which provides hospital care at home, to patients who have been treated at the clinic in question or at clinics interconnected with the Reference Center. Patients treated at home can return to the Reference Center or, when this is not possible, to an interconnected structure, at any time, to be treated in case of worsening of their condition.
Hospital at
home and health care services are provided by intersectoral –
interdisciplinary teams, with the capacity to supervise 100–120 patients
per year, which are interconnected with short-day hospitalization
departments as well as nursing beds of the Reference Center. According
to the decision, a department with at least two free beds available 24
hours a day, every day of the year must be designated for each Reference
Center.
Authors
References
Joint Ministerial Decision from the Ministers of Health and Economics No G2a/oik.28804, “Hospital at Home and Home Health Care”, Official Government Gazette No. 3396/Issue B’/ 19-5-2023.
5.4.1. Specialized ambulatory/outpatient care
Specialized ambulatory care is provided through private solo or group practices and outpatient departments of public hospitals. Many of the specialists working in their private offices or within diagnostic centres are contracted with EOPYY, providing services on a fee-for-service basis (€10 per visit), with an upper limit of 200 visits per month for each specialist. The uneven geographical distribution of contracted EOPYY physicians is a major problem; most are concentrated in large cities, particularly Athens and Thessaloniki, while other areas of the country lack some specialties (Karakolias & Polyzos, 2014). The highest numbers of specialists are in internal medicine, cardiology, obstetrics/gynaecology and orthopaedics.
The 124 outpatient departments of public hospitals provide specialized outpatient care within the ESY. They cover all specialties and are the major providers of ambulatory care services in urban areas. They provide free services during morning hours and visits are scheduled by appointment. Law 2889/2001 established afternoon services in hospital outpatient departments in which the same publicly employed doctors working in the hospital could provide private consultations on an appointment basis. They are paid directly by patients on a fee-for-service basis with the fee shared between the hospital (40%) and the physician (60%). This used to apply only to hospitals with the necessary infrastructure to support all-day clinics, but in 2010 mandatory all-day functioning was extended to all public hospitals in order to increase access to health services, to cope with extra demand and to increase revenues. The afternoon private consultation fees vary from €16 to €72, depending on physicians’ grades.
5.4.2. Inpatient care
The Greek health care system is strongly centred around hospitals (see Box5.4). In 2014, there were 283 hospitals, of which 124 were public, four were private non-profit-making and 155 were private profit-making. This excludes hospitals with special status (e.g. military or prison hospitals). All have outpatient departments, operating on a rotational basis. Private hospitals are profit-making organizations, usually formed as limited liability companies. According to the type of services they offer, Greek hospitals are categorized as either general or specialized. The former include departments of medicine, surgery, paediatrics and obstetrics/gynaecology, supported by imaging and pathology services. They range from big general hospitals in large urban areas, district hospitals located in the main administrative district to small hospitals in semi-urban areas and towns. Specialized hospitals are referral centres for a single specialty (e.g. obstetrics, paediatric care, cardiology or psychiatry). Hospitals linked to the country’s medical schools offer the most complex and technologically sophisticated services (section 4.1.1). Table5.2 presents the hospital configuration in Greece by legal form of ownership and geographical region.
Box5.4
Table5.2
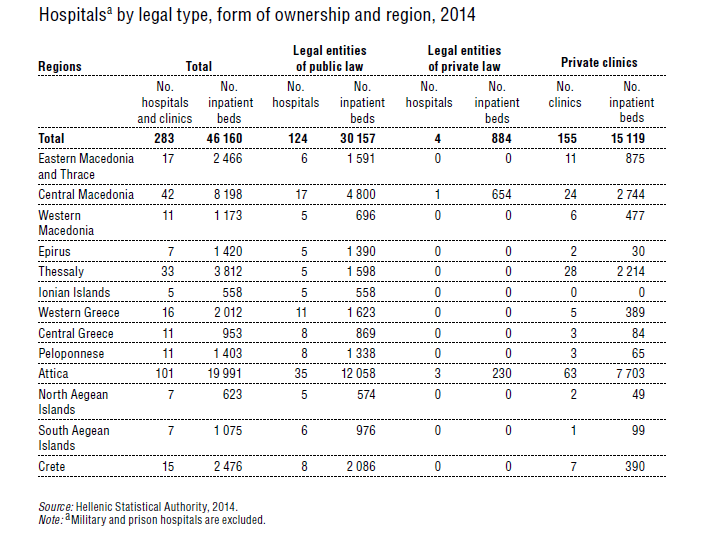
Approximately 65% of beds are in the public sector and 35% in the private sector. The majority of private beds are in small or medium-sized general, obstetric/gynaecological or psychiatric clinics with fewer than 100 beds, low patient occupancy and low staffing rates for all types of personnel. They are mainly contracted with EOPYY, offering services of moderate quality to insured people. A second category of private beds is found in a small number of prestigious high-cost hospitals with 150–400 beds, located mainly in Athens and Thessaloniki and offering high-quality services to private patients and patients with private insurance (Kondilis et al., 2011). One characteristic of the private sector is its high degree of concentration, with fewer private hospitals holding more and more of the market share (Boutsioli, 2007). It is also remarkable that about 43% of the total number of hospital beds in the country are located in Attica, containing 35% of the Greek population and the capital city Athens. Central Macedonia (which contains Thessaloniki, the second largest city in Greece) has the second highest proportion: 17.8% of total beds.
Operationally, hospitals face a number of problems. The management model is outdated and political interference is widespread, particularly in selecting hospital managers and members of governing boards. Human resources management is also problematic, including delayed recruitment processes, lack of substantive staff evaluation and a culture of no accountability for staff underperformance. Lastly, financing and cash flow is still problematic given that the DRG system has not yet been fully developed because of a number of technical problems (Chapters 6 and 7). The quality of services in Greek hospitals is not rated highly by citizens (Box5.5).
Box5.5

In 2011, a number of proposals for hospital restructuring were submitted by an expert committee appointed by the Minister of Health (Liaropoulos et al., 2012) as well as other sources (National School of Public Health, 2011), aiming to achieve economies of scale, optimal allocation of inputs, efficient operation and lower total costs. After public hearings and consultations in the various regional health administrations, which included health managers and other health professional bodies, the final plan was announced in July 2011 (Ministry of Health and Social Solidarity, 2011a). Public hospital management boards were replaced by a total of 82 councils responsible for the administration of all hospitals. In addition, five hospitals that belonged to IKA were transferred to ESY and became branches of five main public hospitals. The total number of beds in ESY hospitals decreased to 30 157; the number of medical departments and units declined by 600 and 15 000 hospital personnel were cut. Additionally, changes were made to the use of eight small hospitals, which were turned into urban health centres, support and palliative care units and hospitals for short-term hospitalization and rehabilitation (Nikolentzos et al., 2015).
In November 2023, Law 5063/2023 was published, providing for the establishment of a National Network of Enhanced Care Units for the treatment of patients with Vascular Stroke. The purpose is:
- to optimize the prevention, treatment and care of patients with vascular stroke and to immediately deal with cases of patients who are in the acute phase;
- to increase functional independence and avoid disability with the implementation of a modern therapeutic approach; and
- to reduce mortality rates and the duration of hospitalization after a stroke.
Authors
References
5.4.3. Day care
Day care units have been slow to develop in Greece. Attempts in the past were fragmented and did not engender the organizational culture required for this type of health care practice. Legislation in 2011 (Law 4025/2011) stalled through a failure to issue a presidential edict defining various operational and technical criteria. Three years later, Law 4254/2014 permitted the establishment of public and private day care units providing diagnosis, curative services and surgical procedures as long as these did not require general, spinal or epidural anaesthesia or hospitalization for more than one day. Public hospitals, PEDYs, health centres, private clinics and private ambulatory care enterprises can establish day care units. A subsequent ministerial decision (No A6/G.P.oik.103516) defined the technical and equipment specifications for day care units to obtain authorization as well as their specialties, including internal medicine, surgery and dentistry. At the time of writing, a number of public and private day care units have been established. However, there are no available data on their exact number or the proportion of care they provide.